
For decades dairy products have been a major source of iodine. The purpose of this study was to determine the iodine nutritional status and its relationship with dairy consumption in pre-schooler children between 2 and 5 years old in a rural area with 27847 inhabitants.
Patients and methodsIt was planned to study 200 participants, selected by random sampling, proportional to the size of the municipality, age, and sex. Parents provided urine samples to analyse urinary iodine, as well as the nutritional information through an interview. A glass of milk or a slice of cheese was considered as a ration, and a portion of other milk derivatives were considered as half rations. The nutritional status of iodine was interpreted with the median (P[percentile]50) of the urinary iodine levels, and iodine intake was estimated using the mean of ration/day of milk and dairy products, fish, and eggs.
ResultsOf the total of 198 subjects that took part, 193 provided urine specimens for the determination of iodine levels. The mean dairy ration/day was 3.8 (SD:1.4). More than two-thirds (69.9%) drank ≥2 glasses of milk/day, and 88.1% consumed a dairy ration of another dairy product. The median urinary iodine level was 184μg/L, but was dependent on glasses of milk/day (282.5μg/L ≥ 4 glasses) and/or the type of milk (233.0μg/L in semi-skimmed). An intake of 117.4μg/day to 178.6μg/day of iodine was estimated, and that milk was the food which provided more iodine (89.9μg/day).
ConclusionsIodine intake was adequate, although higher than necessary when four or more glasses of milk were consumed, and/or when the milk was skimmed. The consumption of dairy products should be monitored to prevent both excessive and deficient intake of iodine.
Hace décadas que los lácteos son una fuente principal de yodo. El fin del estudio fue conocer la situación nutricional de yodo y su relación con el consumo de lácteos, en preescolares de 2–5 años de una zona rural con 27847 habitantes.
Pacientes y métodosSe planificó estudiar a 200, seleccionados por muestreo aleatorio proporcional al tamaño del municipio, edad y sexo. Los progenitores aportaron muestras de orina para analizar yoduria e información nutricional a través de entrevista. Equivalencia de un vaso de leche y una porción de queso a una ración, y la unidad de otros derivados a media ración. El estado nutricional del yodo se interpretó con la mediana (P[percentil]50) de las yodurias y se estimó la ingesta de yodo con la media de raciones/día de leche y derivados, pescado y huevos.
ResultadosParticiparon 198. De 193 se analizaron yodurias. Media ± desviación estándar de raciones de lácteos/día de 3,8 ± 1,4. El 69,9% tomaba ≥ 2 vasos de leche/día y el 88,1% una ración de otros lácteos. Mediana de yodurias de 184μg/L, dependiente de los vasos de leche/día (282,5μg/L en ≥ 4 vasos) y/o del tipo de leche (233,0μg/l en semidesnatada). Se estimó una ingesta de 117,4–178,6μg/día de yodo, y la leche el alimento que más yodo proporcionaría (89,9μg/día).
ConclusionesLa ingesta de yodo resultó adecuada, aunque superior a la necesaria cuando bebían 4 o más vasos de leche y/o cuando la leche era semidesnatada. Se debe vigilar el consumo de lácteos para prevenir tanto excesos como déficits en la ingesta de yodo.
Iodine deficiency has historically affected mankind extensively, especially populations living inland or at high altitudes. Iodine was first associated with thyroid function in the late nineteenth century, and a few decades later there was evidence that its deficiency caused a series of health problems generally labelled “iodine deficiency disorders” (IDDs) that affect foetal and child development (cretinism, physical and cognitive development, increased rate of miscarriage and childhood mortality, and congenital anomalies) as well as the adult population (hypothyroidism and goitre).1
From the late twentieth century, the World Health Organisation (WHO), the United Nations Children's Fund and the International Council for Control of Iodine Deficiency Disorders have promoted numerous initiatives that seek to raise awareness in citizens and national and regional governments regarding the importance of eradicating these disorders by increasing dietary iodine intake. Since it is very cost-effective, iodised salt has been the measure adopted by most countries in the world.2 In 1983, Spain regulated the iodisation of salt for human consumption, establishing an amount of 60mg of iodine per kilogram of salt with a tolerance margin of ±15% (51–69mg/kg).3
In 1982, goitre was endemic in Asturias.4 For that reason, in 1983 the Asturias Council of Public Health started launching campaigns to promote the consumption of iodised salt in homes and mandated its use in school canteens. Recommended iodine intakes were achieved in 1992, so the campaigns were considered a success.4,5 A study conducted in 2010 found that iodised salt was used in 66% of the homes and 100% of school canteens, with median urinary iodine levels of 180μg/L in children aged 6–14 years and 176μg/L in women of child-bearing age that corresponded to optimal dietary intakes of iodine.5
On the other hand, iodine supplementation of animal feeds to prevent IDDs in poultry and cattle (which was regulated by the European Economic Community in 19706) resulted in increases in the iodine contents of foods of animal origin (which were highest in egg yolks and milk). Thus, in the past three decades, the high frequency of consumption of milk and dairy products and the amounts consumed have made these foods major sources of iodine in several countries, including Spain.7–10 Since dairy consumption is high in the young population, our study focused on the population aged 2–5 years to assess the impact of dairy in iodine intake.
We conducted our study in the south west of Asturias, a rural area that at the time of the study had a population of 27,847 inhabitants holders of a personal public health care card (Tarjeta Sanitaria Individual [TSI]), and where cattle farming and mining are the main economic sectors. In 1986, this region had the highest prevalence of goitre in the autonomous community of Asturias, and while the prevalence declined significantly by 1994, it was still of 16.4%.11
Patients and methodsWe conducted a cross-sectional descriptive study between October 2013 and February 2014 that was approved by the Clinical Research Ethics of Asturias and the Fiscalía de Menores (Child Welfare Office).
Population and sampleThe universe of the study consisted of children holders of a TSI for Health Area II of Asturias aged between 2 and 5 years in 2013. We planned to study 200 children, chosen randomly in proportion to the size of municipality of residence, age and sex, and included 286 to be able to count on replacements to make up for potential losses to follow up. We invited families to participate in the study by postal mail, sending information about the study and a copy of the informed consent form. Subsequently, we phoned the parents, making three attempts at different times of the day, and scheduled an appointment for those that agreed to participate at the corresponding health care centre to obtain a random urine sample from the child and conduct a dietary interview. In all municipalities except Tineo (Cangas del Narcea, Pola de Allande, Ibias and Degaña) arrangements were made so that participants that were unable to go to the health care centre in the morning could go in the afternoon. The exclusion criteria were presence of autoimmune thyroid disease, use of diapers or residence outside the health area.
Dietary surveyThe survey consisted of a personal interview, and we collected data for sociodemographic variables (sex, date of birth, municipality of residence, school attended), history of thyroid disease, use of school canteen services, habitual consumption (daily or weekly) of glasses of milk (noting the brand and type of milk) and of single units of yoghourt, flan, custard or Petit Suisse®, eggs, servings of cheese and fish. We also asked about the consumption of iodised salt including the information provided by the label in the salt packaging; for schools, we obtained this information through a telephone call.
Urine sample management and measurement of urinary iodine levels (μg/L)The collected urine samples were transported under refrigeration to the laboratory of the Hospital Comarcal Carmen y Severo Ochoa, where aliquots were prepared and frozen. Aliquots were then submitted to the Hospital Central de Asturias where urinary iodine levels were measured by high-resolution chromatography.
Statistical analysisOverall dairy daily servings were calculated by considering one glass of milk (200mL) and one serving of cheese as one serving, and single units of other dairy products a half serving. We calculated the mean and standard deviation (SD) for the different sociodemographic variables.
We measured daily consumption of milk and dairy servings, and weekly consumption of eggs and fish. We considered that the children consumed iodised salt when parents reported that the label in the salt packaging indicated that it was “iodised”. All variables under analysis were quantitative, and we obtained the absolute frequencies and percentages and the 95% confidence interval (CI) of the main variables, such as the consumption of iodised salt and the total servings of dairy.
We estimated iodine intake based on the mean daily servings consumed of milk, dairy products, fish and eggs. For milk, we used the iodine content data corresponding to Oviedo in the study by Soriguer et al.,9 and for the other foods, we used the information of the Spanish Food Composition Database (Base de Datos Española de Composición de Alimentos12 [BEDCA]), averaging the minimum and maximum values of the most frequently consumed foods.
The indicator used to assess iodine nutritional status in our sample was the median (fiftieth percentile [P50]) urinary iodine level, analysing its distribution in all the variables under study, and we interpreted their values according to the criteria established by the WHO for school-aged children13,14: median of less than 100μg/L as iodine deficiency, median of 100–199μg/L as adequate iodine intake, median of 200–299μg/L as intake exceeding recommendations, and median of 300 or more μg/L as excessive intake. We calculated the 25th and 75th percentiles (P25 and P75) to assess the dispersion in the distribution of urinary iodine levels.
We used the chi square test to analyse the differences between percentages, the Student's t test for differences between means in independent samples, and the Mann–Whitney U test or Kruskal–Wallis test to analyse the difference between two or more medians, respectively. We defined statistical significance as a p-value of less than .05 in the two-tailed test. We performed the statistical analysis with SPSS® version 12.0 for Windows®.
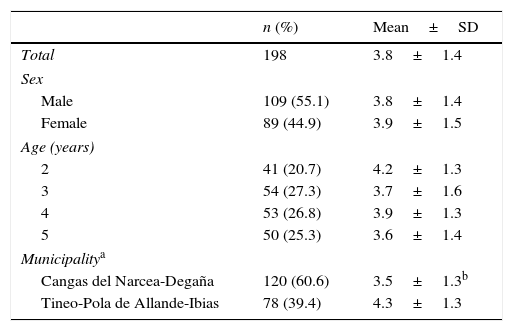
ResultsNutritional information was obtained from 198 preschool-aged children and urinary iodine levels from 193 (97.5%). Of these, 20.2% (n=40) were replacements, 22 due to refusal to take part in the study and the rest because of change of address or lack of response to telephone calls. The distribution of the sample by socio-demographic variables (Table 1) mirrors the population, with the exception of 3-year olds, which are over-represented (27.3% versus 23.6%). Boys accounted for 55.1% and the majority came from the municipalities of Cangas del Narcea (57.1%) and Tineo (31.8%). Most children (77.8%) had lunch at home while the remaining 22.2% had lunch at the school canteen from Monday to Friday.
Mean number of dairy servings consumed per day by sex, age and municipality of residence (n=198).
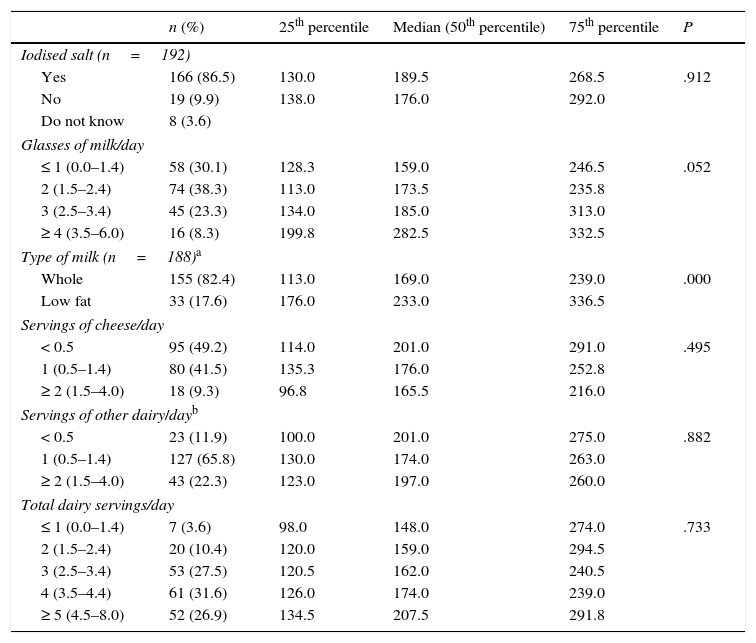
The use of iodised salt was reported by 80.7% of the parents and 100% of school canteens. From both sources, we estimated that of 86.5% of our sample (95% CI, 81.4–91.6) consumed iodised salt (Table 2), of whom 6.0% only consumed it at school.
Distribution of intake of iodised salt, milk and dairy products, and corresponding urinary iodine levels (μg/L) (median, 25th percentile and 75th percentile) (n=193).
| n (%) | 25th percentile | Median (50th percentile) | 75th percentile | P | |
|---|---|---|---|---|---|
| Iodised salt (n=192) | |||||
| Yes | 166 (86.5) | 130.0 | 189.5 | 268.5 | .912 |
| No | 19 (9.9) | 138.0 | 176.0 | 292.0 | |
| Do not know | 8 (3.6) | ||||
| Glasses of milk/day | |||||
| ≤ 1 (0.0–1.4) | 58 (30.1) | 128.3 | 159.0 | 246.5 | .052 |
| 2 (1.5–2.4) | 74 (38.3) | 113.0 | 173.5 | 235.8 | |
| 3 (2.5–3.4) | 45 (23.3) | 134.0 | 185.0 | 313.0 | |
| ≥ 4 (3.5–6.0) | 16 (8.3) | 199.8 | 282.5 | 332.5 | |
| Type of milk (n=188)a | |||||
| Whole | 155 (82.4) | 113.0 | 169.0 | 239.0 | .000 |
| Low fat | 33 (17.6) | 176.0 | 233.0 | 336.5 | |
| Servings of cheese/day | |||||
| < 0.5 | 95 (49.2) | 114.0 | 201.0 | 291.0 | .495 |
| 1 (0.5–1.4) | 80 (41.5) | 135.3 | 176.0 | 252.8 | |
| ≥ 2 (1.5–4.0) | 18 (9.3) | 96.8 | 165.5 | 216.0 | |
| Servings of other dairy/dayb | |||||
| < 0.5 | 23 (11.9) | 100.0 | 201.0 | 275.0 | .882 |
| 1 (0.5–1.4) | 127 (65.8) | 130.0 | 174.0 | 263.0 | |
| ≥ 2 (1.5–4.0) | 43 (22.3) | 123.0 | 197.0 | 260.0 | |
| Total dairy servings/day | |||||
| ≤ 1 (0.0–1.4) | 7 (3.6) | 98.0 | 148.0 | 274.0 | .733 |
| 2 (1.5–2.4) | 20 (10.4) | 120.0 | 159.0 | 294.5 | |
| 3 (2.5–3.4) | 53 (27.5) | 120.5 | 162.0 | 240.5 | |
| 4 (3.5–4.4) | 61 (31.6) | 126.0 | 174.0 | 239.0 | |
| ≥ 5 (4.5–8.0) | 52 (26.9) | 134.5 | 207.5 | 291.8 | |
Of all participants, 69.9% consumed two or more glasses of milk a day (83.3% in Tineo-Pola de Allande-Ibias and 61.7% in Cangas del Narcea-Degaña), and most of them consumed whole milk (82.4%) from the Central Lechera Asturiana® brand (63.2%). Cheese consumption was reported in 79.8%: 49.2% fewer than one serving a day, 56.1% semi-cured cheese, and 39.4% fresh cheese. Furthermore, 88.1% consumed one serving of other type of dairy every day, which was yoghourt in 98.0% (whole fat in 98.5%), Petit Suisse® in 70.7%, custard in 37.9% and flan in 24.2% (Table 2).
When it came to the total daily consumption of dairy, 37.9% of the sample consumed two to three servings a day, and 58.5% (95% CI, 51.5–65.3) more than three. Table 1 shows a mean±standard deviation consumption of 3.8±1.4 (95% CI, 3.6–4.0) servings of dairy a day, and we found no differences based on sex or age, although we did find a difference based on the municipality of residence, with the highest consumption found in children from the towns of Tineo-Pola de Allande-Ibias (4.3 versus 3.5 servings/day in children from Cangas del Narcea-Degaña; P=.000).
In our sample, 80.3% of participants reported that they usually consumed between two and four eggs a week, and 73.1% reported consuming two or more servings of fish a week.
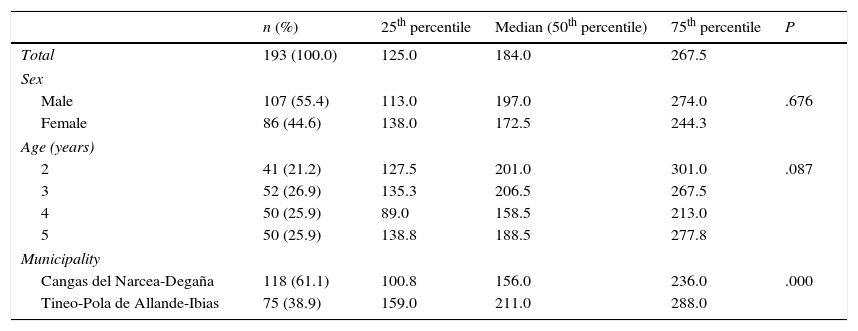
Urinary iodine levels (μg/L)The median urinary iodine level of the population under study was 184μg/L. It exceeded 150μg/L in both boys and girls and in all age groups, with the highest levels of more than 200μg/L found in children aged 2 and 3 years of age. The median level in children from Tineo, Pola de Allande and Ibias was 35% greater than in children from Cangas del Narcea and Degaña (211.0 versus 156.0μg/L; P=.000) (Table 3).
Distribution of urinary iodine levels (μg/L) (median, 25th percentile and 75th percentile) by demographic characteristics (n=193).
| n (%) | 25th percentile | Median (50th percentile) | 75th percentile | P | |
|---|---|---|---|---|---|
| Total | 193 (100.0) | 125.0 | 184.0 | 267.5 | |
| Sex | |||||
| Male | 107 (55.4) | 113.0 | 197.0 | 274.0 | .676 |
| Female | 86 (44.6) | 138.0 | 172.5 | 244.3 | |
| Age (years) | |||||
| 2 | 41 (21.2) | 127.5 | 201.0 | 301.0 | .087 |
| 3 | 52 (26.9) | 135.3 | 206.5 | 267.5 | |
| 4 | 50 (25.9) | 89.0 | 158.5 | 213.0 | |
| 5 | 50 (25.9) | 138.8 | 188.5 | 277.8 | |
| Municipality | |||||
| Cangas del Narcea-Degaña | 118 (61.1) | 100.8 | 156.0 | 236.0 | .000 |
| Tineo-Pola de Allande-Ibias | 75 (38.9) | 159.0 | 211.0 | 288.0 | |
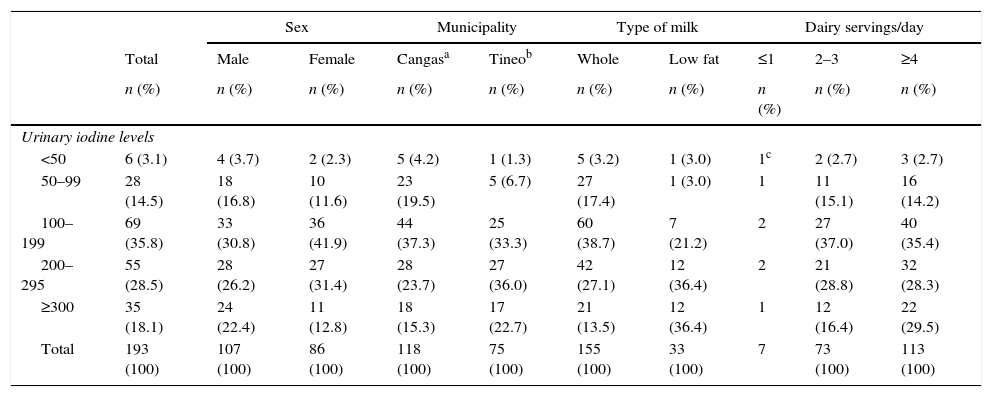
We found levels below 50μg/L in 3.1% of participants (4.2% in the municipalities of Cangas and Degaña and 1.3% in the others) and exceeding 300μg/L in 18.1% (and in more than 20% in the following subsets: boys, residents of Tineo-Pola de Allande-Ibias, consumers of low fat milk, and consumers of four or more servings of dairy/day) (Table 4).
Percentage distribution of urinary iodine levels (μg/L) by sex, municipality, type of milk and servings of dairy/day (n=193).
| Sex | Municipality | Type of milk | Dairy servings/day | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Male | Female | Cangasa | Tineob | Whole | Low fat | ≤1 | 2–3 | ≥4 | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Urinary iodine levels | ||||||||||
| <50 | 6 (3.1) | 4 (3.7) | 2 (2.3) | 5 (4.2) | 1 (1.3) | 5 (3.2) | 1 (3.0) | 1c | 2 (2.7) | 3 (2.7) |
| 50–99 | 28 (14.5) | 18 (16.8) | 10 (11.6) | 23 (19.5) | 5 (6.7) | 27 (17.4) | 1 (3.0) | 1 | 11 (15.1) | 16 (14.2) |
| 100–199 | 69 (35.8) | 33 (30.8) | 36 (41.9) | 44 (37.3) | 25 (33.3) | 60 (38.7) | 7 (21.2) | 2 | 27 (37.0) | 40 (35.4) |
| 200–295 | 55 (28.5) | 28 (26.2) | 27 (31.4) | 28 (23.7) | 27 (36.0) | 42 (27.1) | 12 (36.4) | 2 | 21 (28.8) | 32 (28.3) |
| ≥300 | 35 (18.1) | 24 (22.4) | 11 (12.8) | 18 (15.3) | 17 (22.7) | 21 (13.5) | 12 (36.4) | 1 | 12 (16.4) | 22 (29.5) |
| Total | 193 (100) | 107 (100) | 86 (100) | 118 (100) | 75 (100) | 155 (100) | 33 (100) | 7 | 73 (100) | 113 (100) |
When it came to dairy products, we only found a significant association between urinary iodine levels and the consumption of milk, with iodine levels increasing linearly with the number of glasses consumed (P=.052, almost statistically significant), and a median level of 282.5μg/L in participants that consumed four or more glasses of milk. The median in participants that consumed low fat milk was 38% higher than the median in those that consumed whole milk (233.0 versus 169.0μg/L; P=.000). We also found a dose-dependent association between urinary iodine levels and the number of servings of any type of dairy consumed a day, but this result was not statistically significant (Table 2).
The median intake was higher in children that consumed iodised salt compared to children that did not (189.5 versus 176.0μg/L), although this difference was not statistically significant (Table 2). We did not find an association between urinary iodine levels and the consumption of eggs or fish.
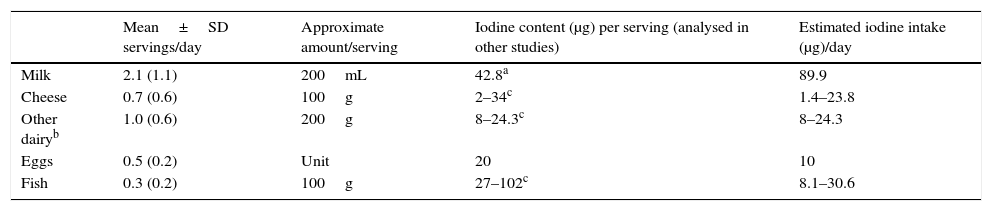
Estimation of iodine intake based on the mean daily consumption of milk and derivatives, fish and eggsThe estimated iodine intake ranged between 117.4 and 178.6μg a day. Milk was the main source, contributing 89.9μg a day. Between 8 and 24.3μg a day of iodine would come from dairy products such as yoghourt, Petit Suisse®, flan and custard, while eggs would contribute 10μg a day. The iodine contribution of cheese and fish varies widely depending on the food consumed (Table 5).
Estimation of iodine intake based on the mean daily servings of dairy, eggs and fish (n=198).
| Mean±SD servings/day | Approximate amount/serving | Iodine content (μg) per serving (analysed in other studies) | Estimated iodine intake (μg)/day | |
|---|---|---|---|---|
| Milk | 2.1 (1.1) | 200mL | 42.8a | 89.9 |
| Cheese | 0.7 (0.6) | 100g | 2–34c | 1.4–23.8 |
| Other dairyb | 1.0 (0.6) | 200g | 8–24.3c | 8–24.3 |
| Eggs | 0.5 (0.2) | Unit | 20 | 10 |
| Fish | 0.3 (0.2) | 100g | 27–102c | 8.1–30.6 |
BEDCA (latest update in August 2010): minimum and maximum values for foods consumed most frequently: Cheese (2mg/100g of fresh cheese, cabrales blue cheese, goat cheese or ricotta requesón, and 34mg/100g Manchego cheese). Other dairy (8mg/100g Petit Suisse and 24.3mg/100g whole milk yoghourt). Fish (27–37mg/100g of sardines, hake, sole and salmon and 60–102mg/100g of octopus, squid and fried cod).
We found an adequate iodine intake in the sample under study, with a median urinary iodine level that was higher than the one observed in the 6-to-14-year old population of Asturias in 20105,15 (184μg/L versus 180μg/L) and in other regions of Spain, such as La Axarquía in 1997–1998 (120μg/L)8 and the Basque Country in 2012 (147μg/L).7
The mean number of dairy servings consumed per day was also higher than the one observed in the age 6-to-14 years population in 20105,15 (3.8 versus 3.3). The current recommendation for children is two to three servings a day,16 but 58.5% of the sample under study consumed more than three servings a day. There was a clear difference in consumption between municipalities (4.3 versus 3.5 servings/day) that was accompanied by a difference in the corresponding urinary iodine levels, with participants from Tineo-Pola de Allande-Ibias consuming amounts of iodine that exceeded recommendations and participants from Cangas del Narcea-Degaña of preschool age having a higher risk of insufficient iodine intake. The difference in dairy consumption patterns may be related to the livestock that predominates in the towns with the highest populations, such as beef cattle in Cangas del Narcea and dairy cattle in Tineo (in 2013 Tineo produced 18.8% of the milk in Asturias).17
Most children consumed at least two glasses of milk a day and one serving a day (equivalent to two units) of dairy products, mainly yoghourt and Petit Suisse®. Although cheese was consumed frequently, it was in lesser amounts.
We found an association between urinary iodine levels and milk intake measured in glasses consumed. Children that drank four or more glasses of milk a day had an iodine intake that could be a mild health hazard due to exceeding daily requirements (urinary iodine level, 282.5μg/L), something that was also observed in consumers of low fat milk (urinary iodine level, 233μg/L).
Considering that both deficiencies and excesses in intake need to be prevented,13,18 a salient finding in our study was that 26.1% of participants had extreme urinary iodine levels of less than 50 or of 300 or more micrograms per litre. Extreme intake can lead to problems associated with hyperthyroidism in individuals with a history of goitre that reside in previously iodine-deficient areas (Jod Basedow effect), autoimmune thyroiditis13,14,18 and subclinical hypothyroidism.19 In 2013, ten countries in the world were categorised as having excessive iodine intake,18 and in 2005 the European Union, concerned that peak levels of iodine in milk and eggs could be exceeding the levels allowed in adolescents and adults,20 mandated the reduction of the iodine content in cattle and poultry feeds from 10 to 4ppm.21
Milk was already described as a significant source of iodine in 1997–1998 in La Axarquía8 and in subsequent studies in Spain.9,10 This is also consistent with the fact that in the United Kingdom—the first country in Europe that implemented iodine fortification of livestock feed, before 1940—, while sales of iodised salt in the continent amounted to only 5% of the total salt, adequate iodine levels were achieved when consumption of milk increased in schoolchildren due to its promotion by successive governments.18,22 The decrease in milk consumption observed in recent years has resulted in the resurgence of iodine deficiency in this country.18,23
The lack of a statistically significant association between increased urinary iodine levels and increased overall consumption of dairy products in our study could be due to the lower content of iodine in dairy products and the variability of iodine intake depending on the product consumed. The dairy products consumed most frequently were whole milk yoghourt and Petit Suisse®, estimated to contribute 6 and 8μg/100g of iodine, respectively.12
The contribution of eggs and fish to the total iodine intake is modest, as these foods are not consumed daily.13 Most of the sample under study consumed an adequate amount of eggs (2–4/week) and while consumption of fish was frequent, only 16% consumed the recommended four servings per week.
The daily recommended allowance of iodine in children aged 1 to 8 years is 90μg/day,9 and in the sample under study, this requirement would be met by consumption of milk alone, as it contributed 98.4μg/day (a value obtained from adjusting the estimate of 89.9μg/day, as in the analysis of iodine content in milk in the form of iodide, the amount recovered is 87%10). This estimate is similar to the one calculated by Arrizabalaga et al.10 of 50μg of iodine for one serving of 200–250mL of milk based on the weighted annual mean of monthly analyses of the iodine content of milk samples, with the highest iodine concentrations occurring between January and May and the lowest between July and November, and intermediate concentrations from June to December. Our study was conducted between October and February, and thus encompasses a full range.
The consumption of iodised salt was higher than it was in Asturias in 20105,15 (85.9% versus 66%). Since neither study verified iodine intake by checking the packaging label of the salt consumed, both may have overestimated intake. A study conducted in the Basque Country in 2012 that assessed intake based on the packaging label reported consumption of iodised salt in 53% of households.7 We also ought to note that iodised salt brands do not always reach the established concentrations, as in 1995 only 15% of salt packages distributed in Madrid and Cuenca had adequate iodine contents,24 and in 2014 in Asturias, 12 out of the 16 commercial brands did not meet regulatory standards (contents were either insufficient or excessive), although in April 2015, this issue had been resolved in 10 out of the 12 brands after appropriate measures were taken by the General Directorate of Public Health.25 Furthermore, iodine contents may decrease in households due to humidity. For all the above reasons, it is difficult to guarantee adequate iodine intake through salt consumption, even if the latter is widespread.
Conclusions- 1.
Dairy consumption must be monitored to adjust it to current recommendations, because while we observed an overall adequate intake of iodine in preschool-aged children, iodine intake may be insufficient or excessive in a considerable percentage.
- 2.
In order to maintain an optimal intake in the population, the health authorities should periodically monitor iodine concentrations in milk, as there may be changes in the production process or in dietary habits.7
This study was funded by the General Directorate of Public Health of the Health Department of the Autonomous Community of Asturias.
Conflicts of interestThe authors of this article have no conflicts of interest to declare.
We want to thank the medical specialist in epidemiology, Carmen Mosquera Tenreiro, for her continued support and advice; Ana Araceli Eyo González, Guillermo Agramunt García-Sala (Hospital Carmen y Severo Ochoa), and Juan Carlos Fernández (Hospital Universitario Central de Asturias) for their work in the laboratory analysis of iodine levels; the entire staff of the Health Care Centres that provided us with the space to carry out the interviews and helped us manage unexpected issues; and, needless to say, all parents that decided to participate and spend the time necessary to go to the health care centres and answer all the questions in the interview.
Please cite this article as: Arbesú Fernández E, Serrano Peraza MH, Eguia Angeles HA, Sotelo García CO, Saint Jean CH, Musa Martín NI. Yodurias y consumo de lácteos en preescolares del Área Suroccidental de Asturias. An Pediatr (Barc). 2017;87:18–25.
Previous presentation: a summary of this study was presented orally and as a poster at the XXII Encuentro de Residentes de Medicina y Enfermería Familiar y Comunitaria de Asturias, and Jornadas de Atención Primaria; April 10–11, 2014; Cangas de Onís, Spain.

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals