





Self-limiting sternal tumours of childhood (SELSTOC) are characterised by the development of a sternal tumour unrelated to previous trauma, rapidly growing and with spontaneous resolution.1,2
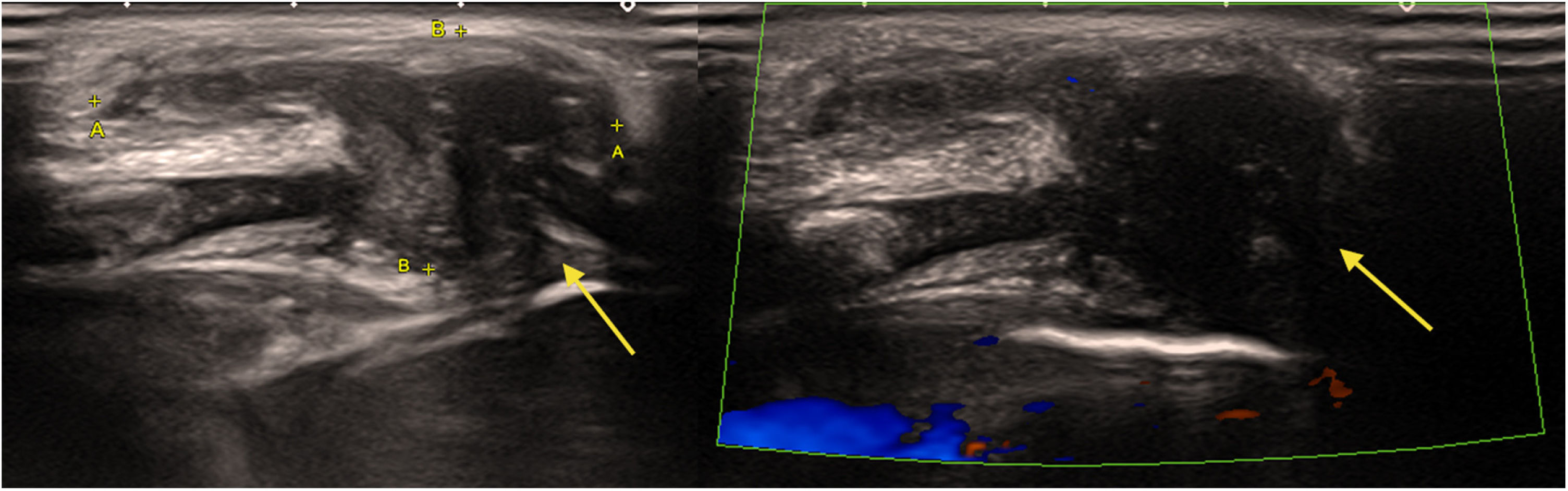
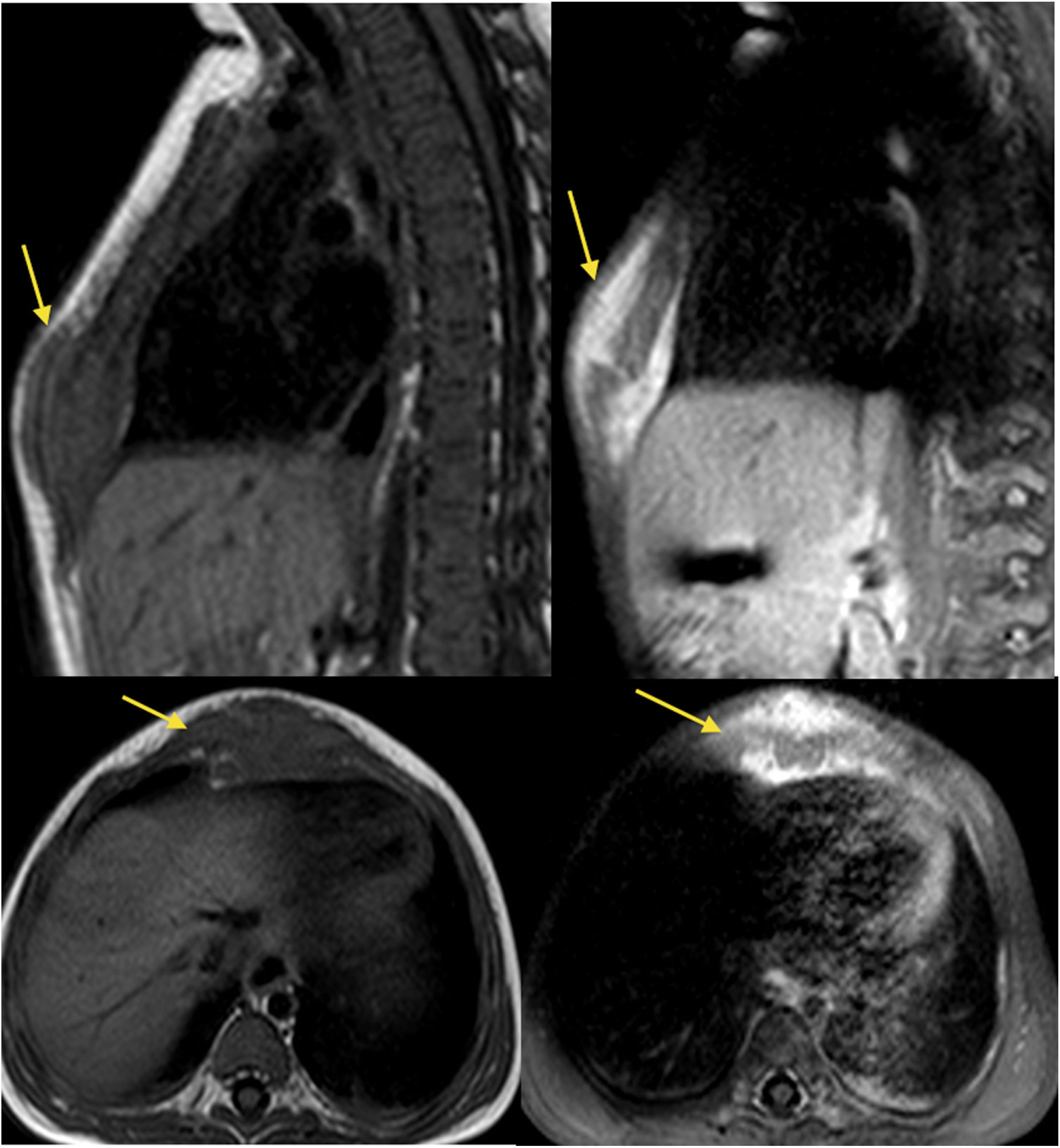
We present the case of a female infant aged 7 months who presented with a tumour in the lower third of the sternum (Fig. 1) detected 2 months prior, of solid consistency, mildly tender on palpation and coughing. The family reported there was no previous trauma and no associated constitutional symptoms. The ultrasound scan (Fig. 2) and magnetic resonance imaging (Fig. 3) showed a solid lesion (31 × 14 × 16 mm) at the level of the cartilage between the sternal body and the xiphoid process with involvement of the cartilage of the right 6th and 7th costochondral joints. The examination of a biopsy specimen of the lesion showed mature fibrocartilaginous material with no signs of malignancy. The patient remained in follow-up at the outpatient level, with observation of the gradual regression of the tumour until it nearly disappeared and resolution of symptoms.

The detection of a solid sternal mass in childhood requires differential diagnosis including inflammatory, infectious and malignant diseases. If a patient presents with a rapidly growing mass and no relevant history, the possibility of SELSTOC must be considered. This clinical spectrum could encompass Tietze syndrome, an infrequent self-limited inflammation of the costochondral junction described in the paediatric age group.3 In some cases, imaging tests may be required, and possibly a biopsy for the histological examination of the lesion. The course is self-limiting, usually with spontaneous regression, and the symptoms may be managed with analgesics as needed.
