

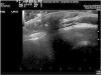

A boy aged 7 years presented for assessment of a congenital lesion of the vertex. The physical examination revealed a bulging bald patch soft to the touch surrounded by a hair collar (Fig. 1). The subcutaneous ultrasound scan showed continuity of the bone without defects (Fig. 2). The magnetic resonance image scan showed the presence of an atretic meningocele and a Dandy-Walker malformation of the cisterna magna (Fig. 3).



The term “hair collar” sign was introduced by Commens et al. in 1989.1 It refers to a ring of long, dark and coarse hair surrounding a congenital bald nodule with a cystic, bullous or atrophic appearance in the scalp. This is considered a sign of cranial dysraphism.2 It may take the form of true meningoceles or encephaloceles resulting from herniation of intracranial contents through a cranial defect, atretic meningoceles or encephaloceles in which a small cranial bone defect remains and the intracranial connection appears as a fibrous tract, and rudimentary meningoceles (heterotropic brain tissue) in which the connection has closed completely and there is no residual cranial defect.
Imaging tests are essential to rule out cranial defects, communication to the intracranial space and associated intracranial vascular anomalies. Computed tomography is the most accurate method, although sonography is a harmless technique that provides real-time information for detection of bone abnormalities. If a bony defect is identified, performance of magnetic resonance imaging is indicated to assess for the presence of heterotropic brain tissue.3
