



Sickle cell disease is an autosomal recessive disease in which red blood cells with abnormal haemoglobin S take on a sickle shape, causing obstruction of capillary blood blow and haemolysis.1 Vaso-occlusive crises with bone involvement (bone infarction) are the most common clinical manifestation, mainly in the humerus, tibia and femur.1,2 Tissue devitalization after vaso-occlusive crises, the saturation of macrophages with products derived from chronic haemolysis and splenic dysfunction predispose to bone infection,1,2 and Salmonella is the most frequent causative agent.1 Clinical manifestations are similar in both cases (tenderness, warmth, erythema and swelling)2 and the findings of conventional imaging techniques (radiography and ultrasonography) are frequently inconclusive. In the field of nuclear medicine, dual-tracer bone scintigraphy (with diphosphonate and colloid tracers) is available for the purpose of differential diagnosis.
We present the case of a boy aged 12 years with sickle cell disease that visited the emergency department with pain in the proximal region of the left tibia lasting 48h in the absence of trauma. The patient initially improved with analgesic treatment (morphine hydrochloride) but worsened on the third day, with exacerbation of pain, local oedema and elevation of acute phase reactants and procalcitonin. The patient did not have leukocytosis or fever (although the absence of fever is infrequent, it has been described to reach proportions of up to 22% of cases in some series3).
A radiograph and an ultrasound examination were ordered due to the need to make a differential diagnosis between bone infarction and osteomyelitis. Both showed nonspecific inflammatory soft tissue changes in the anterior region of the left tibia and neither allowed differentiation of the disease. Empirical intravenous antibiotherapy was initiated, and a bone scintigraphy was ordered.
The patient underwent a bone scintigraphy scan, with capture of static images in the blood pool phase (at 5min) and the metabolic phase (2h) following intravenous injection of 335MBq of 99mTc-HDP. The images revealed increased distribution in the vascular and interstitial compartment and increased osteogenic activity in the left tibial tuberosity, with very faint and diffuse tracer uptake in the two proximal thirds of the ipsilateral tibial diaphysis, and no other abnormalities in the rest of the examined structures. This scintigraphic pattern may appear in bone infarcts as well as osteomyelitis.1
A bone marrow scintigraphy was performed at 24h to differentiate between the two diseases. Images were captured in a similar position 20min after the intravenous injection of 201MBq of 99mTc-sulfur colloid. Imaging showed normal uptake in the tuberosity of the left tibia, with decreased uptake in the two proximal thirds of the ipsilateral tibial shaft (Fig. 1).
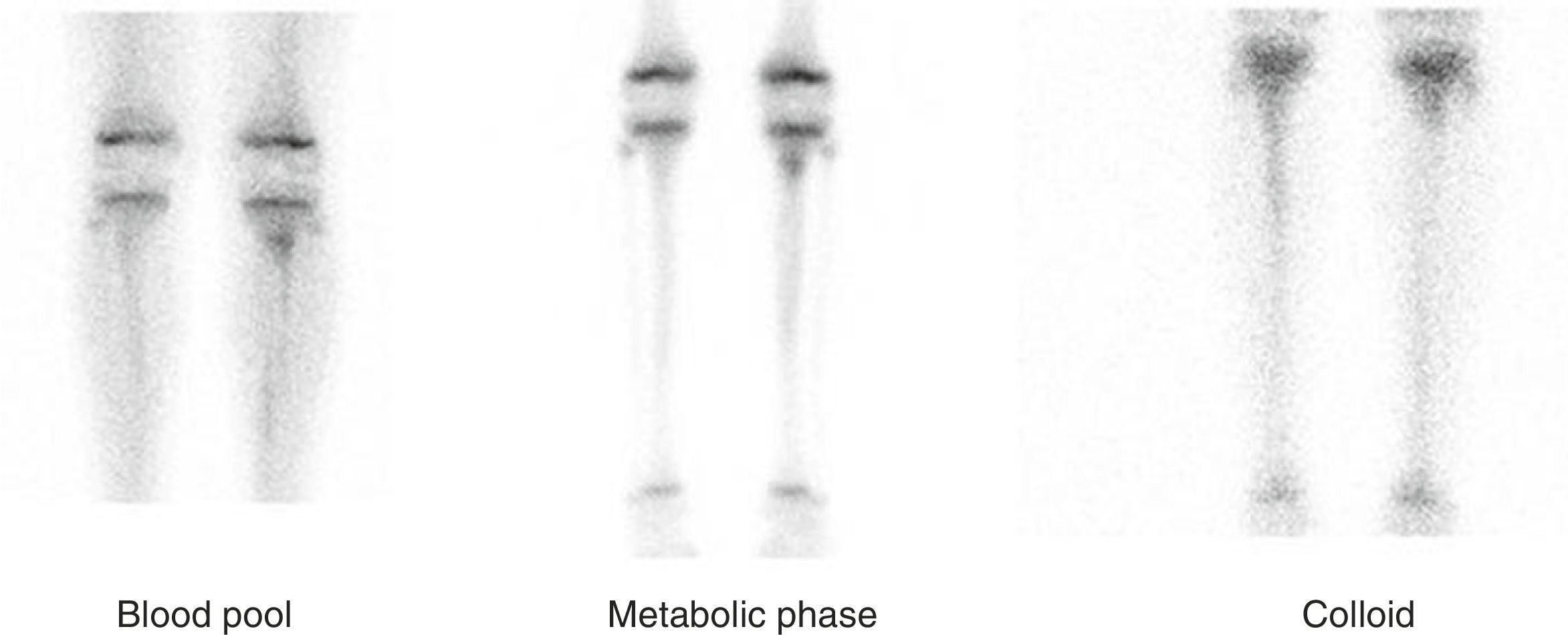
During the blood pool phase, the bone scan showed an increased diffusion of the radiotracer in the vascular-interstitial compartment in the left tibial tuberosity. In the metabolic phase and the colloid study: focal increased uptake in the left tibial tuberosity, with normal uptake in the colloid study. Slightly increased diffuse uptake in the two proximal thirds of the left tibial diaphysis, with decreased uptake in the colloid study.
The scintigraphic pattern was compatible with osteomyelitis in the tuberosity of the left tibia and with bone infarction in the two proximal thirds of the ipsilateral tibial diaphysis.
Early in the course of disease, it is difficult to differentiate between osteomyelitis and bone infarction based on clinical or radiological features. Nevertheless, plain radiography is used as the initial imaging technique to rule out other diseases (tumours and fractures). The characteristic radiologic findings cannot be detected until at least 10 days have elapsed since the onset of symptoms.4
An ultrasound examination may be useful in sites that can be accessed with this technique, mainly for the detection of collections and abscesses in soft tissue.1,4
Dual-tracer bone scintigraphy can differentiate between bone infarction and osteomyelitis. On scintigraphy, osteomyelitis presents with increased tracer uptake (there may be decreased uptake in the early stages). Increased uptake is also observed in cases of bone infarction during the revascularization phase, starting from the third day from onset (uptake may be normal or decreased before the third day).2,5
It is during the revascularization phase that bone marrow scintigraphy can differentiate between the two diseases, as bone infarction continues to exhibit decreased uptake, whereas osteomyelitis exhibits normal tracer uptake.1,2
Bone marrow scanning targets the reticuloendothelial system of bone marrow, while bone scanning reflects the reparative osteoblastic response.6 Bone scintigraphy is abnormal in both osteomyelitis and bone infarction, whereas bone marrow scintigraphy is normal in osteomyelitis.
In the context of sickle-cell disease, it is important to take into account the medical history, as previous bone infarctions may continue to exhibit decreased uptake2 and it is not possible to determine whether they are new or old lesions by means of scintigraphy, which requires consideration of current manifestations and the previous history in their assessment.
In conclusion, currently available nuclear medicine techniques can be very useful, as dual-tracer bone scintigraphy makes possible the early differential diagnosis of bone infarction versus osteomyelitis through non-invasive means, which is important in children with sickle cell disease in who both diseases overlap.
Please cite this article as: Sandoval-Moreno C, Castillejos-Rodríguez L, García-Alonso MP, Rubio-Gribble B, Penín-González FJ. Papel de la medicina nuclear en el diagnóstico diferencial entre infarto óseo y osteomielitis en el contexto de drepanocitosis. An Pediatr (Barc). 2017;87:353–355.
