

We read with attentive interest the article “Novelties in the pediatric cardiopulmonary resuscitation recommendations and lines of development in Spain”, by López-Herce et al. on behalf of the Spanish Group of Paediatric and Neonatal Cardiopulmonary Resuscitation (GERCPPYN).1
First of all, we want to underscore the active role of the GERCPPYN in the dissemination of knowledge on the management of paediatric cardiac arrest in Spain as well as its coordination, and are grateful for the effort to facilitate the involvement in this process of all paediatricians and health care professionals who deliver care to children.
We understand that the purpose of the article was to analyse international guidelines for paediatric life support/cardiopulmonary resuscitation (CPR) (terms accepted for interchangeable use by the Consejo Español de Reanimación Cardiopulmonar [CERCP, Spanish Council of Cardiopulmonary Resuscitation]) and to identify and disseminate the main changes that have been made since the 2015 guidelines of the European Resuscitation Council (ERC2 and the adaptations to be applied in Spain. However, in our opinion, the article was not always sufficiently clear in differentiating between the ERC-2021guidelines,3 the 2020 International Liaison Committee on Resuscitation (ILCOR) Consensus on Science with Treatment Recommendations (CoSTR4 and the adaptations proposed by the GERCPPYN. The aim of this letter is to present structured supplemental information to attempt to facilitate its comprehension.
The article highlights many of the ILCOR/CoSTR-20204 and the ERC-20213 recommendations: teamwork, the use of tools to aid the initial evaluation (ABCDE), the management of septic shock and bradycardia, calling for help after delivery of the first 5 rescue breaths in basic life support, involving two rescuers in delivering bag-valve-mask ventilation, initiating ventilation with settings based on the respiratory rate for age after securing the airway, considering the stepwise escalation of the energy dose for defibrillation in refractory arrhythmias, the use of capnography and sonography, post-resuscitation care goals and ethical and training considerations. However, some of the novelties, perhaps due to the limited length of the article, are not mentioned and we consider that detailing them would be relevant (Table 1). In addition, other recommendations presented as novel had already been implemented in clinical practice, as is the case of the administration of adrenaline “as soon as possible” in nonshockable rhythms, a current recommendation based on studies included in the development of the ILCOR/CoSTR-20204 that support administration after 3min, whereas previous guidelines had recommended establishing vascular access and administrating adrenaline, but not waiting until having delivered 3min of chest compressions to initiate it, as could be inferred from the article. There is also the recommendation regarding the use of paddles for defibrillation of charging them once they have been placed on the chest (an aspect that was not featured in the ERC-20152 but did appear in subsequent ERC-CERCP training materials5). In the ERC-20213 set-up, the safety of rescuers is prioritised over saving time, but the guideline also states that the use of self-adhesive pads is preferred and that shocks should be delivered within 5 seconds to minimise the time without chest compressions.
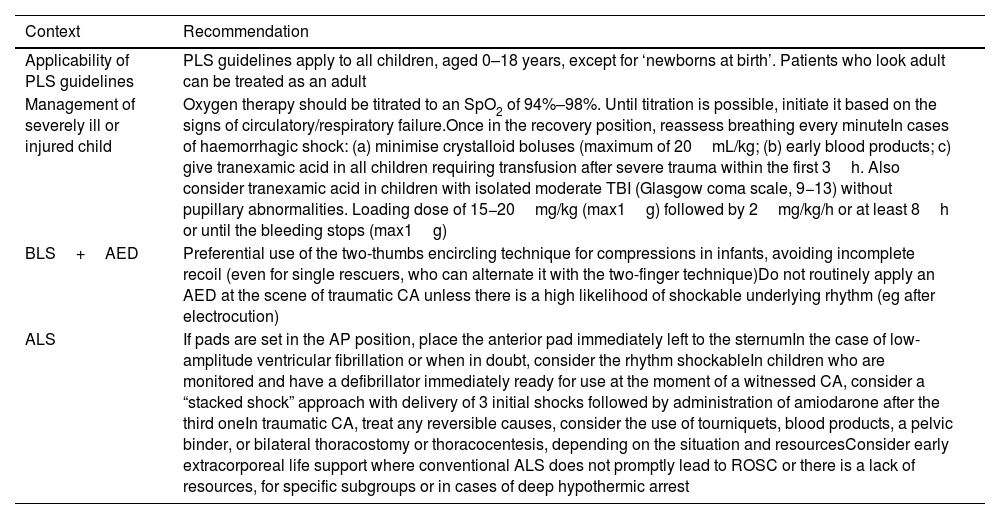
Additional novelties in the ERC-2021 paediatric life support recommendations.3
| Context | Recommendation |
|---|---|
| Applicability of PLS guidelines | PLS guidelines apply to all children, aged 0–18 years, except for ‘newborns at birth’. Patients who look adult can be treated as an adult |
| Management of severely ill or injured child | Oxygen therapy should be titrated to an SpO2 of 94%–98%. Until titration is possible, initiate it based on the signs of circulatory/respiratory failure.Once in the recovery position, reassess breathing every minuteIn cases of haemorrhagic shock: (a) minimise crystalloid boluses (maximum of 20mL/kg; (b) early blood products; c) give tranexamic acid in all children requiring transfusion after severe trauma within the first 3h. Also consider tranexamic acid in children with isolated moderate TBI (Glasgow coma scale, 9−13) without pupillary abnormalities. Loading dose of 15−20mg/kg (max1g) followed by 2mg/kg/h or at least 8h or until the bleeding stops (max1g) |
| BLS+AED | Preferential use of the two-thumbs encircling technique for compressions in infants, avoiding incomplete recoil (even for single rescuers, who can alternate it with the two-finger technique)Do not routinely apply an AED at the scene of traumatic CA unless there is a high likelihood of shockable underlying rhythm (eg after electrocution) |
| ALS | If pads are set in the AP position, place the anterior pad immediately left to the sternumIn the case of low-amplitude ventricular fibrillation or when in doubt, consider the rhythm shockableIn children who are monitored and have a defibrillator immediately ready for use at the moment of a witnessed CA, consider a “stacked shock” approach with delivery of 3 initial shocks followed by administration of amiodarone after the third oneIn traumatic CA, treat any reversible causes, consider the use of tourniquets, blood products, a pelvic binder, or bilateral thoracostomy or thoracocentesis, depending on the situation and resourcesConsider early extracorporeal life support where conventional ALS does not promptly lead to ROSC or there is a lack of resources, for specific subgroups or in cases of deep hypothermic arrest |
AED, automated external defibrillator; ALS, advanced life support; AP: anteroposterior; BLS, basic life support; CA, cardiac arrest; ERC, European Resuscitation Council; PLS, paediatric life support; SpO2, partial oxygen saturation; VF, ventricular fibrillation.
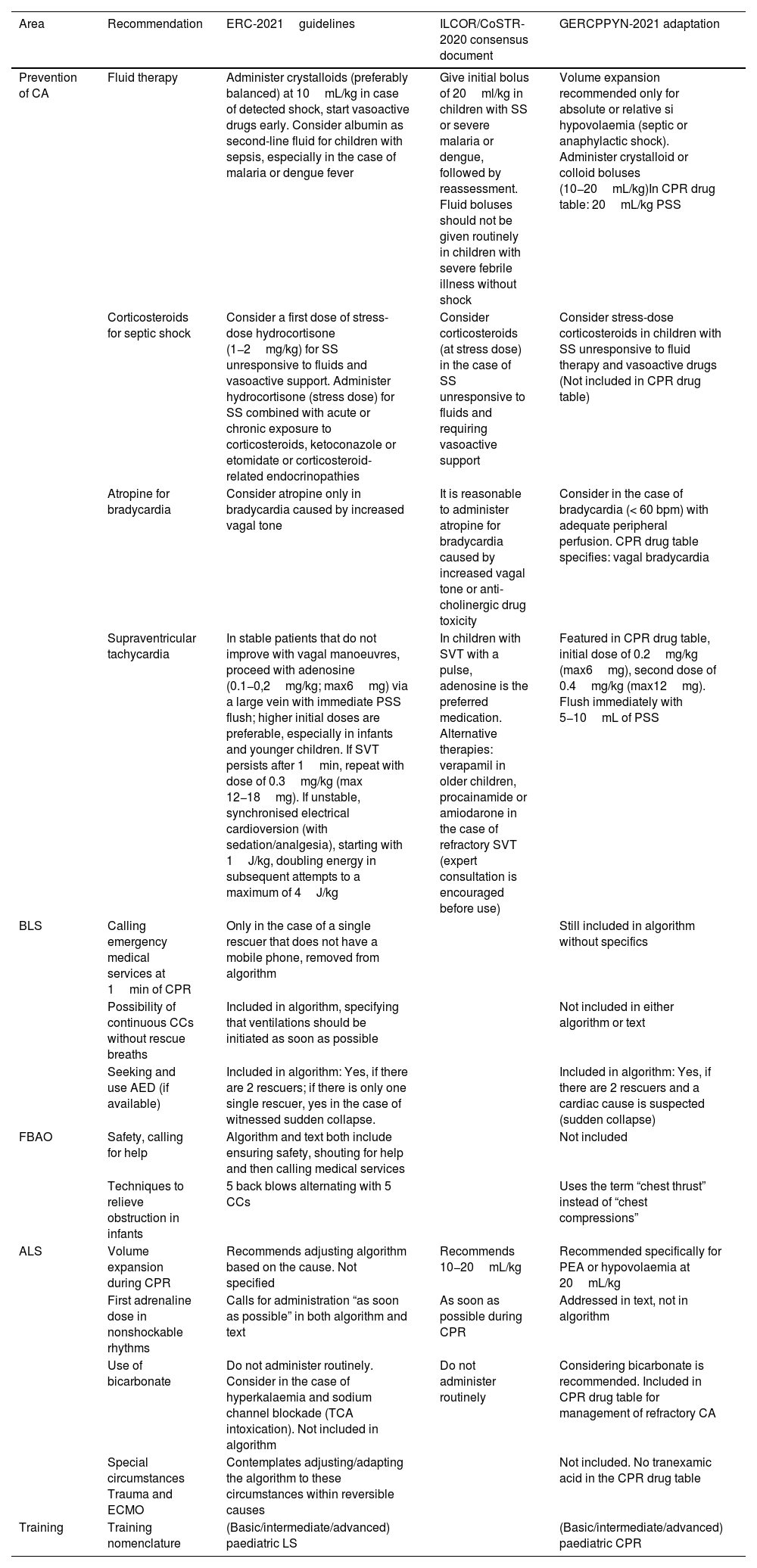
Last of all, with the aim of supplementing the information on the recent recommendations offered by López-Herce et al. and to promote a better understanding of their source (ILCOR/CoSTR-20204 or ERC-20213), the changes that have taken place and the adaptations proposed by GERCPPYN for their implementation in Spain, we developed Table 2.
| Area | Recommendation | ERC-2021guidelines | ILCOR/CoSTR-2020 consensus document | GERCPPYN-2021 adaptation |
|---|---|---|---|---|
| Prevention of CA | Fluid therapy | Administer crystalloids (preferably balanced) at 10mL/kg in case of detected shock, start vasoactive drugs early. Consider albumin as second-line fluid for children with sepsis, especially in the case of malaria or dengue fever | Give initial bolus of 20ml/kg in children with SS or severe malaria or dengue, followed by reassessment. Fluid boluses should not be given routinely in children with severe febrile illness without shock | Volume expansion recommended only for absolute or relative si hypovolaemia (septic or anaphylactic shock). Administer crystalloid or colloid boluses (10−20mL/kg)In CPR drug table: 20mL/kg PSS |
| Corticosteroids for septic shock | Consider a first dose of stress-dose hydrocortisone (1−2mg/kg) for SS unresponsive to fluids and vasoactive support. Administer hydrocortisone (stress dose) for SS combined with acute or chronic exposure to corticosteroids, ketoconazole or etomidate or corticosteroid- related endocrinopathies | Consider corticosteroids (at stress dose) in the case of SS unresponsive to fluids and requiring vasoactive support | Consider stress-dose corticosteroids in children with SS unresponsive to fluid therapy and vasoactive drugs (Not included in CPR drug table) | |
| Atropine for bradycardia | Consider atropine only in bradycardia caused by increased vagal tone | It is reasonable to administer atropine for bradycardia caused by increased vagal tone or anti-cholinergic drug toxicity | Consider in the case of bradycardia (< 60 bpm) with adequate peripheral perfusion. CPR drug table specifies: vagal bradycardia | |
| Supraventricular tachycardia | In stable patients that do not improve with vagal manoeuvres, proceed with adenosine (0.1−0,2mg/kg; max6mg) via a large vein with immediate PSS flush; higher initial doses are preferable, especially in infants and younger children. If SVT persists after 1min, repeat with dose of 0.3mg/kg (max 12−18mg). If unstable, synchronised electrical cardioversion (with sedation/analgesia), starting with 1J/kg, doubling energy in subsequent attempts to a maximum of 4J/kg | In children with SVT with a pulse, adenosine is the preferred medication. Alternative therapies: verapamil in older children, procainamide or amiodarone in the case of refractory SVT (expert consultation is encouraged before use) | Featured in CPR drug table, initial dose of 0.2mg/kg (max6mg), second dose of 0.4mg/kg (max12mg). Flush immediately with 5−10mL of PSS | |
| BLS | Calling emergency medical services at 1min of CPR | Only in the case of a single rescuer that does not have a mobile phone, removed from algorithm | Still included in algorithm without specifics | |
| Possibility of continuous CCs without rescue breaths | Included in algorithm, specifying that ventilations should be initiated as soon as possible | Not included in either algorithm or text | ||
| Seeking and use AED (if available) | Included in algorithm: Yes, if there are 2 rescuers; if there is only one single rescuer, yes in the case of witnessed sudden collapse. | Included in algorithm: Yes, if there are 2 rescuers and a cardiac cause is suspected (sudden collapse) | ||
| FBAO | Safety, calling for help | Algorithm and text both include ensuring safety, shouting for help and then calling medical services | Not included | |
| Techniques to relieve obstruction in infants | 5 back blows alternating with 5 CCs | Uses the term “chest thrust” instead of “chest compressions” | ||
| ALS | Volume expansion during CPR | Recommends adjusting algorithm based on the cause. Not specified | Recommends 10−20mL/kg | Recommended specifically for PEA or hypovolaemia at 20mL/kg |
| First adrenaline dose in nonshockable rhythms | Calls for administration “as soon as possible” in both algorithm and text | As soon as possible during CPR | Addressed in text, not in algorithm | |
| Use of bicarbonate | Do not administer routinely. Consider in the case of hyperkalaemia and sodium channel blockade (TCA intoxication). Not included in algorithm | Do not administer routinely | Considering bicarbonate is recommended. Included in CPR drug table for management of refractory CA | |
| Special circumstances Trauma and ECMO | Contemplates adjusting/adapting the algorithm to these circumstances within reversible causes | Not included. No tranexamic acid in the CPR drug table | ||
| Training | Training nomenclature | (Basic/intermediate/advanced) paediatric LS | (Basic/intermediate/advanced) paediatric CPR |
AED, automated external defibrillator; ALS, advanced life support; BLS, basic life support; CA, cardiac arrest; CC, chest compression; CoSTR, International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations; CPR, cardiopulmonary resuscitation; CC, chest compression; ECMO, extracorporeal membrane oxygenation; ERC, European Resuscitation Council; FBAO, foreign body airway obstruction; GERCPPYN, Grupo Español de Reanimación Cardiopulmonar Pediátrica y Neonatal; ILCOR, International Liaison Committee on Resuscitation; LS, life support; PEA, pulseless electrical activity; PSS, physiological saline solution; SS, septic shock; SVT, supraventricular tachycardia; TCA, tricyclic antidepressant.
We hope that our contribution may supplement the work carried out by the GERCPPYN and serve to clarify or qualify some points.

