




Male neonate born at 37 weeks of gestation, with no obstetric or maternal history of interest. The first physical examination revealed a mass in the right elbow (Fig. 1), with no other abnormalities.

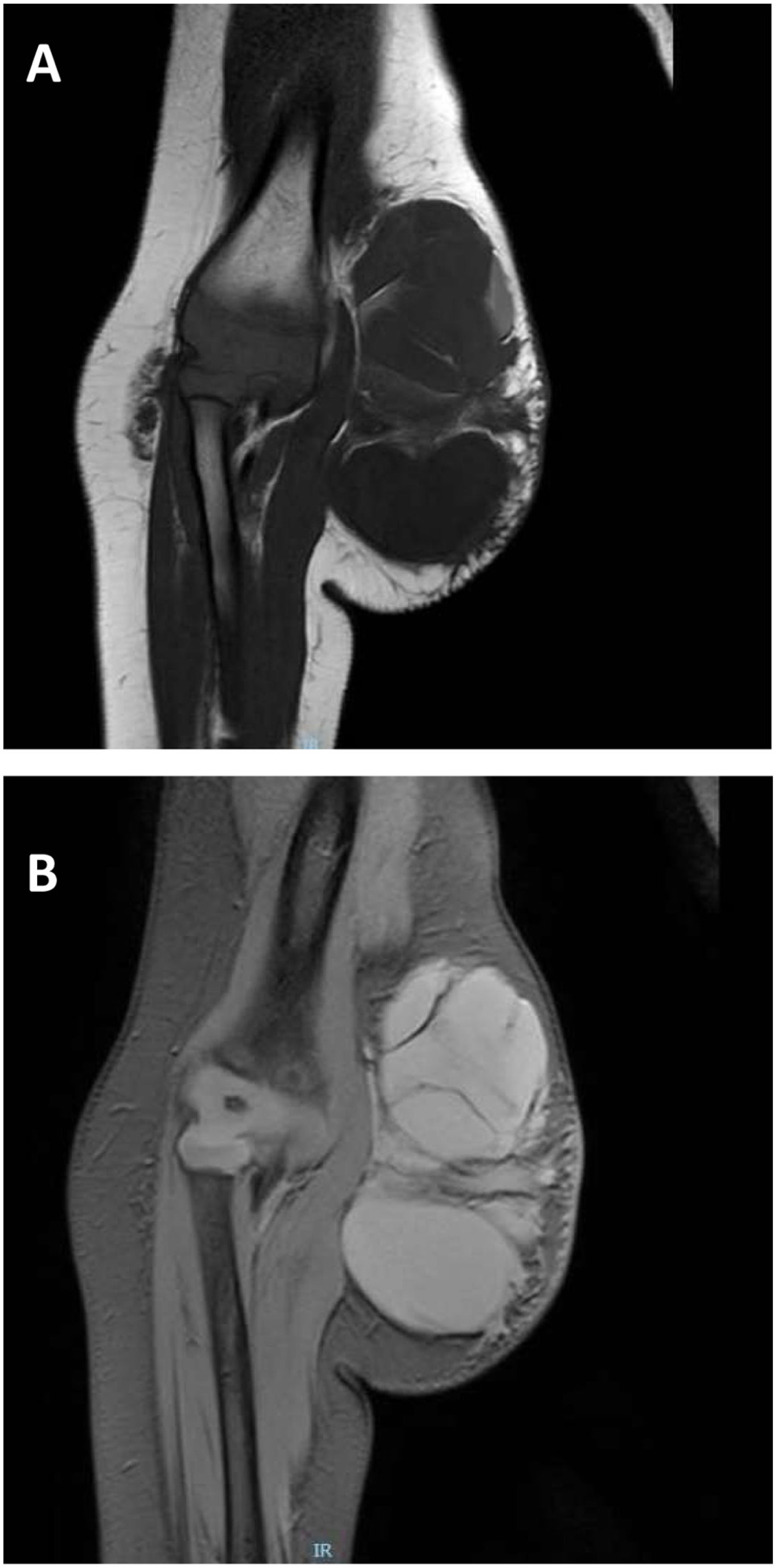
The infant was assessed in the paediatric surgery and radiology departments (Figs. 2 and 3), leading to diagnosis of a microcystic lymphatic malformation.1–3 Following a multidisciplinary evaluation, the decision was made to surgically remove the lesion with intraoperative neurophysiological monitoring at age 1.5 years. The histological examination of the specimen confirmed the suspected diagnosis, with detection of the D2 40 marker (+). No further abnormalities have been identified in the follow-up to date.
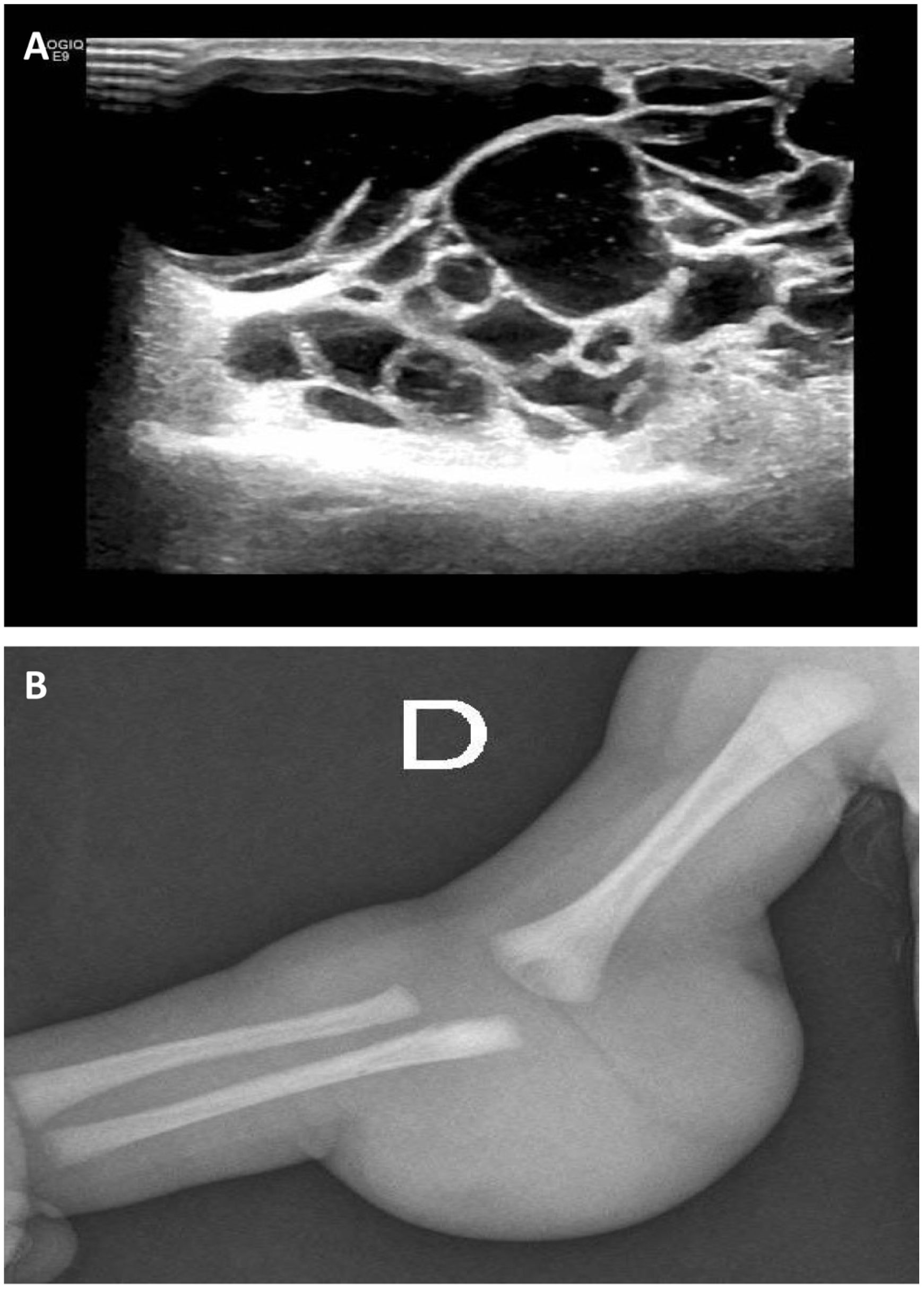
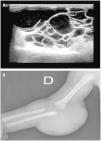
Ultrasound scan and plain radiograph of the lesion.
(A) Ultrasound scan of the right upper extremity: multicystic lesion measuring 52 × 34 × 52 mm (CC × AP × TR), predominantly avascular, located in the subcutaneous tissue of the posterior elbow and extending into the adjacent compartments. No involvement of bone, joints or muscle tissue. (B) Plain radiograph of the right upper extremity showing a tumour in the right elbow.
Lymphatic malformations, formerly known as lymphangiomas, are congenital malformations resulting from the obstruction of lymphatic vessels, usually in the cervical region.1,3 It is rarely found in the upper extremities. Sonography2 is useful for their diagnosis, as it can detect the presence of cysts. They rarely progress to malignant tumours. Watchful waiting is a controversial approach, as these masses rarely regress spontaneously.1 There are several options for medical management2,3 (sirolimus, OK-432 or doxycycline) reserved for macrocystic malformations. However, surgical management1–3 continues to be the most frequent approach, although the appropriate timing is still under debate: some authors recommend surgery at birth, and others after 1–2 years of life.
