




Idiopathic facial aseptic granuloma (IFAG) is a recently described disease that affects the paediatric age group.1 It is characterised by the development of one or more nodules in the cheeks and the differential diagnosis must include other facial nodules acquired in childhood, including pilomatrixomas, dermoid cysts, bacterial infection by Leishmania or mycobacteria and vascular malformations. For this reason, it is probably underdiagnosed.
We conducted a retrospective observational study of all cases of IFAG diagnosed in our hospital over a 12-year period. Table 1 summarises the characteristics of these cases. The mean age of the patients was 3 years. Three of the patients had multiple lesions. Five of the patients received oral antibiotherapy: 2 amoxicillin–clavulanic acid, 1 cefuroxime, 1 clarithromycin and 1 amoxicillin–clavulanic acid followed by azithromycin with no clear evidence of improvement. The disease tended to resolve spontaneously by a mean of 13 months. Two patients underwent surgical removal of the lesions. None of the patients experienced complications or recurrence during the follow-up.
Patient characteristics.
| Case | Sex | Age | Clinical features | Histological examination | Ultrasound | Time to resolution |
|---|---|---|---|---|---|---|
| 1 | Male | 5 years | Indurated nodule in right cheek | Yes | Yes | Surgical removal |
| 2 | Male | 4 months | Several papules in left cheek. Plaque with central crust | Yes | No | 15 months |
| 3 | Male | 9 years | Soft nodule in left cheek | Yes | Yes | 15 months |
| 4 | Male | 2 years | Nodule in left cheekPerioral pink papulesEpisodes of facial erythema | Yes | No | 9 months |
| 5 | Male | 8 months | Purulent papule in left cheek | No | No | 14 months |
| 6 | Female | 2 years | Nodule in right cheekBleedingPapule in left cheekChalazion | Yes | Yes | Surgical removal |
| 7 | Female | 6 years | Nodule in left cheek | No | Yes | Ongoing |
The histological examination revealed a granulomatous reaction of the dermis, with lymphocyte and plasma cells and negative results of staining for detection of microorganisms (Fig. 1C). In one of the cases, the examination found remnants of an epidermoid cyst.
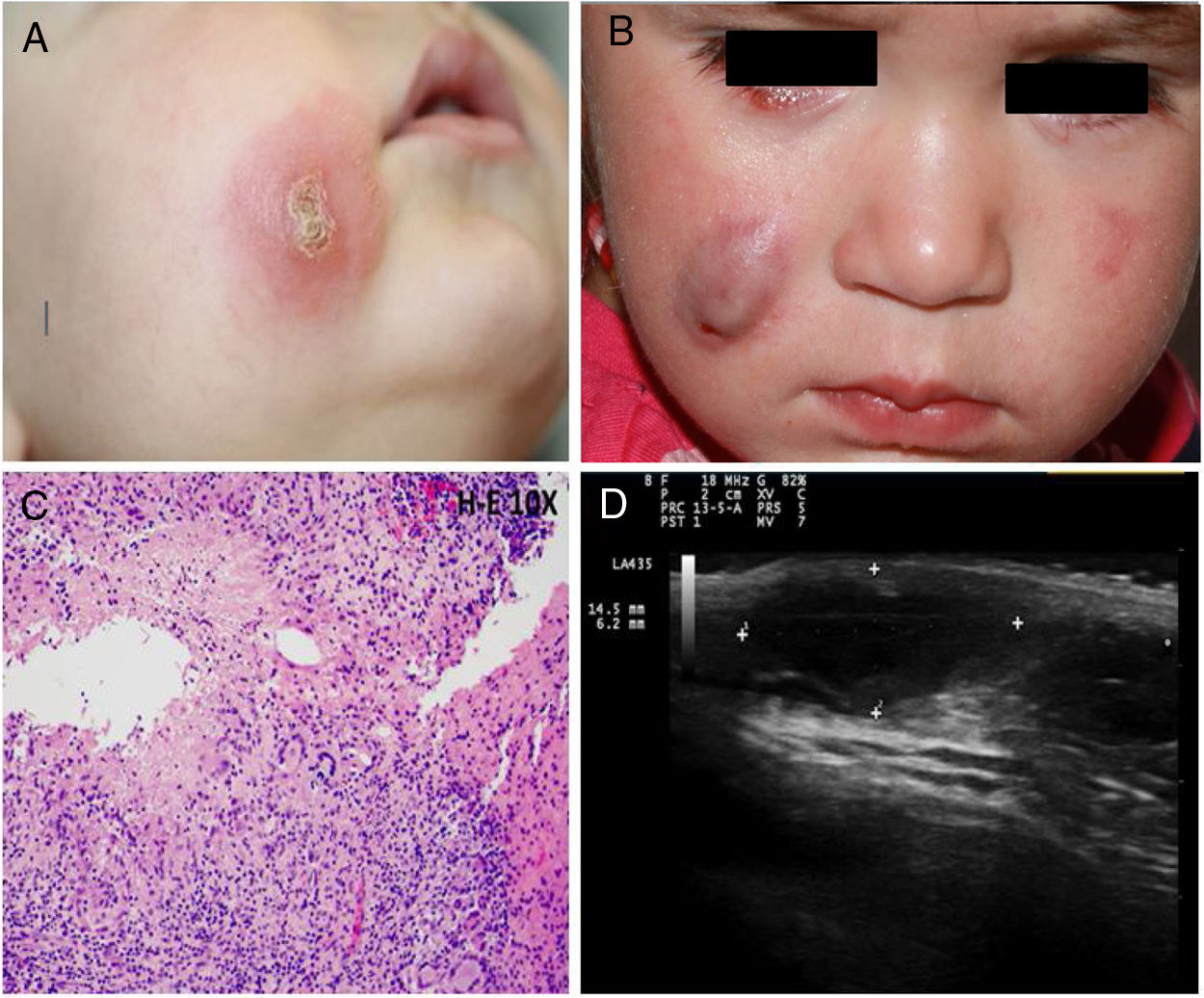
(A) Clinical image of case 2. (B) Clinical image of case 6 showing a chalazion in the right lower eyelid. (C) Histological examination of the lesion in the right cheek of case 6, showing a cutaneous infiltrate of lymphocytes and plasma cells with granulomas composed of histocytes and multinucleate giant cells. (D) Ultrasound of lesion in the right cheek (case 6) showing a hypoechoic structure with a rolled posterior edge.
The ultrasound scan revealed hypoechoic oval structures in the dermis with the longest diameter parallel to the skin surface. There were no calcium deposits. The posterior edge was even except in 1 case in which it exhibited mildly rolled edges (Fig. 1D). The posterior hypodermis was hyperechoic. The presence of peripheral fluid was variable, and there was no fluid within the lesion in any case.
Idiopathic facial aseptic granuloma is characterised by the development of a painless, hard red or purple nodule in the cheek.2 It has a characteristic location: in 2/3 of cases, it is located within a triangle with vertices at the earlobe, the external corner of the eye and the mouth corner. There is usually a single lesion, although some patients may have more than 1. It tends to regress spontaneously in a mean of 11 months.2 All patients in our case series fit these clinical characteristics and course of disease.
The mean age at onset is 46 months, with a range of 8 months to 13 years.1,2 It is more frequent in female patients, although this was not the case in our series.
The pathogenesis of IFAG has yet to be determined. One of the current hypotheses is that it could belong in the spectrum of granulomatous rosacea in children.3 The concomitant presence of chalazions (commonly associated with rosacea), described in up to 2/3 of patients at the time of diagnosis of IFAG, the subsequent development of rosacea lesions in a large number of patients, the detection of perifollicular histocyte infiltration in the histological examination, typical of granulomatous rosacea, or the response to antibiotic agents used for treatment of rosacea are some of the features that suggest an association with granulomatous rosacea.3–5 In our case series, one patient developed perioral rosacea papules and another patient had a chalazion.
The possibility of an infectious aetiology seems to have been excluded, at least when it comes to known pathogens.2
A third hypothesis suggests the development of a granulomatous reaction in response to an embryonal remnant.2 This possibility is supported by a case where the histological examination revealed remnants of an epidermoid cyst,2 which we also found in one of our patients.
Lastly, other proposed aetiologies include a persisting reaction to an insect bite or traumatic injury.
The histological presentation of IFAG is characterised by a cutaneous inflammatory granulomatous infiltrate composed mainly of lymphocytes, histocytes, neutrophils and multinucleated foreign body giant cells in the absence of calcification or ghost cells.2
The ultrasound examination of skin lesions reveals hypoechoic oval structures in the dermis with posterior hyperechogenicity with no calcification.2,4 Patients with acute inflammation present with perilesional fluid, which disappears as the lesion resolves. In most cases of IFAG, there is no fluid within the lesion.6
When it comes to treatment, the previous literature describes improvement with long courses (2–3 months) of oral clarithromycin or doxycycline and topical metronidazole or ivermectin.3,5 Amoxicillin–clavulanic acid, azithromycin, erythromycin and cefalexin have proven ineffective.
The aim of this study was to bring attention to a disease that is probably underdiagnosed. Since this disease resolves spontaneously and is located in an area that has an aesthetic impact, the use of invasive diagnostic tests must be justified, and ultrasonography is an important non-invasive tool in its differential diagnosis. In the future, additional descriptions of IFAG cases will probably help elucidate the aetiology and optimal management of this disease.
Please cite this article as: Docampo Simón A, Sánchez-Pujol MJ, Schneller-Pavelescu L, Berbegal L, Betlloch Mas I. Granuloma aséptico facial idiopático: características clinicopatológicas y ecográficas. An Pediatr (Barc). 2020;92:297–9.
