





A boy aged 3 years presented with intermittent abdominal pain of 72hours duration, fever of 3hours duration and self-limited vomiting associated with episodes of crying, drawing legs to chest and diaphoresis. There was diffuse tenderness in the abdomen and the physical examination was difficult. The ultrasound was not very useful due to poor cooperation, as it was not possible to identify the appendix or assess for inflammatory signs. Blood tests revealed leukocytosis (20500/mm3) with a procalcitonin (PCT) level of 0.5ng/mL and a C-reactive protein (CRP) level of 61mg/L. Given the abdominal pain of undetermined aetiology and the inability to rule out a condition requiring surgery, the patient was admitted for observation. Since the symptoms persisted, the tests were repeated at 14hours, evincing a decrease in the white blood cell count (19100) and the level of PCT (0.3), albeit mild, and further elevation of CPR (69). A new ultrasound scan evinced an appendix measuring up to 11mm (Fig. 1), and surgery evinced the presence of a nonpurulent appendiceal phlegmon with torsion of the appendix, which was removed. Fig. 2 shows the surgical specimen and Fig. 3 an illustration of its examination. The postoperative outcome was favourable and the patient was discharged 5 days after the procedure.


Video-assisted transumbilical laparoscopic approach with visualization of scant serous fluid and a nonpurulent appendiceal phlegmon adhered to the anterior abdominal wall and containing the vermiform appendix. Upon exteriorizing the organ, the 360° clockwise torsion of the appendix 3cm from the base could be observed that gave rise to an area of different calibre and hue (arrow). Distal to the torsion site, the appendix had a purplish gangrenous appearance, felt taut and exhibited significant venous ingurgitation, although without purulence or macroscopic perforation. However, proximal to the torsion site, the appearance of the appendix and mesentery was normal. The pathological examination found gangrenous appendicitis with areas of haemorrhage.
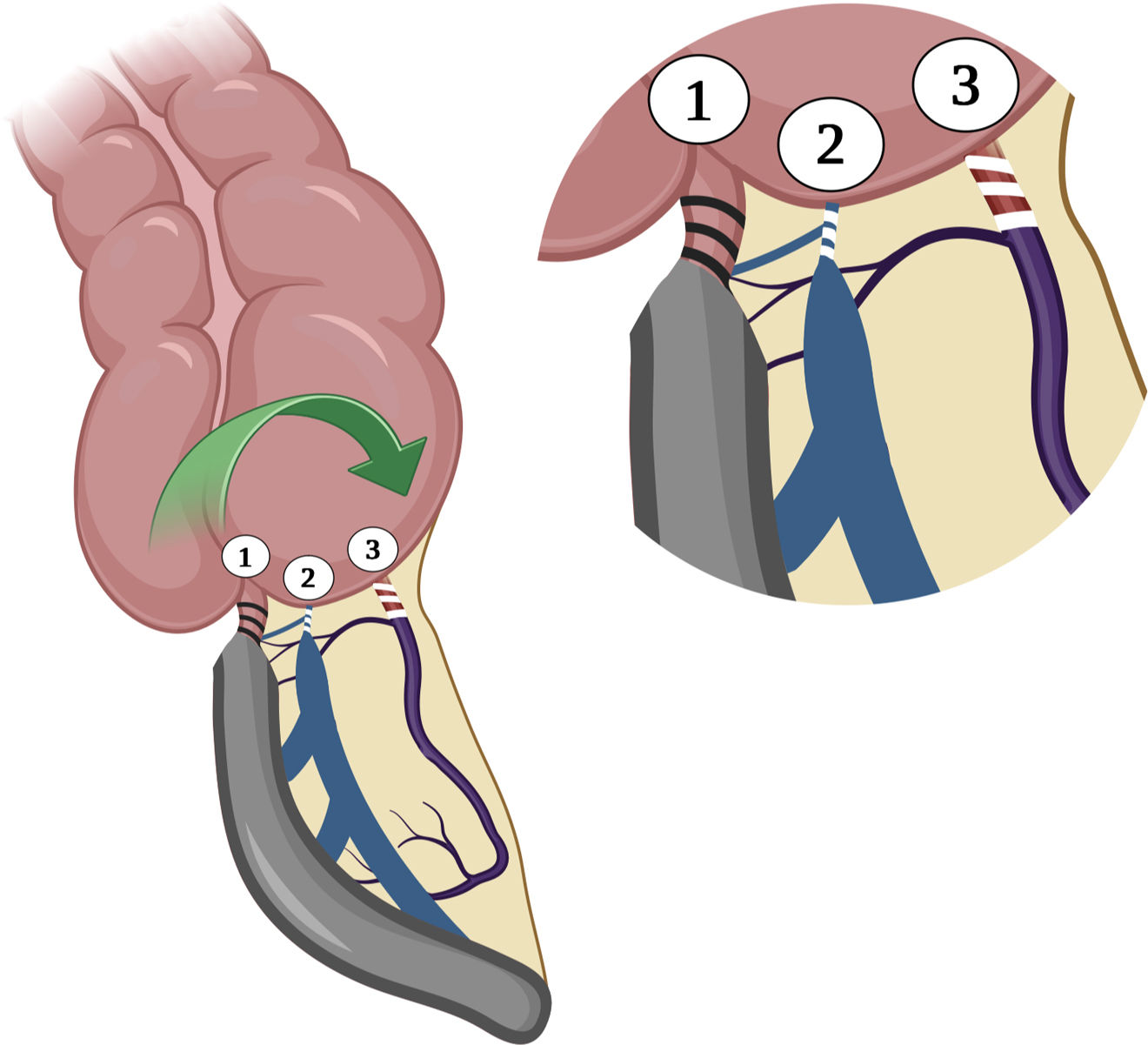
Illustration depicting the point of axial torsion of the vermiform appendix and its vessels, resulting in strangulation of (1) the appendiceal lumen, (2) the veins, with significant vascular ingurgitation, and (3) the appendicular artery with absence of blood flow, blanching due to ischaemia and, as a result, necrosis.
The twisting of the appendix around its long axis resulting in vascular and luminal obstruction is known as volvulus or torsion of the appendix.1 Its incidence is unknown, and fewer than 80 cases have been reported.2 It is not possible to distinguish it from classic appendicitis based on the clinical presentation, although absence of signs of infection could support the suspicion of torsion, which is an ischaemic rather than a septic condition.3 This case illustrates the diversity of appendiceal disease and contributes a description of a rare presentation of appendicitis to the literature.
FundingNone to declare.
