

Supraventricular tachycardia (SVT) is the most common arrhythmia in the neonatal period, but its association with other triggering processes is not well established. The aim of the study was to analyse the possible relationship between neonatal SVT and gastroesophageal reflux disease (GERD), a condition which was recently linked to atrial arrhythmias.
Material and methodsA retrospective longitudinal descriptive study was conducted over a period of 5 years on newborns who were diagnosed with SVT in a level III neonatal unit, assessing morphological aspects, associated symptoms, and treatments received. Its association with GERD and the impact of this on SVT was studied.
ResultsEighteen patients (1.2 per 1000 newborns) were diagnosed with SVT. Fifty percent of them were combined with clinically significant GERD (P=.01), and all of them received drug treatment. The average time of control of SVT without GERD since diagnosis was 6 days (95% CI: 2.16–9.84, with a median of 3) and 7.6 days when both pathologies were present (95% CI: 4.14–10.9, with a median of 7) (P=.024).
ConclusionsPatients with SVT in the neonatal period frequently have GERD, and this combination leads to more difficulty in controlling the tachycardia. The reflux could act as a trigger or perpetuator of arrhythmia, therefore it is important to find and treat GERD in infants with SVT.
La taquicardia supraventricular (TSV) es la arritmia más común en el periodo neonatal, sin embargo, su asociación con otros procesos desencadenantes no está bien establecida. El objetivo de este estudio es analizar la posible relación entre TSV neonatal y el reflujo gastroesofágico (RGE), por ser una dolencia relacionada recientemente con las arritmias auriculares.
Material y métodosSe realizó un estudio descriptivo longitudinal retrospectivo de recién nacidos que fueron diagnosticados de TSV en una unidad neonatal de nivel III, durante un período de 5años, valorando los aspectos morfológicos, la sintomatología asociada y los tratamientos recibidos. Se estudió su asociación con el RGE y la repercusión de este sobre la TSV.
ResultadosDieciocho pacientes (1,2 de cada 1.000 recién nacidos) fueron diagnosticados de TSV. El 50% asociaban RGE con repercusión clínica (p=0,01) y todos ellos recibieron tratamiento farmacológico. El tiempo medio de control de la TSV sin RGE desde el diagnóstico fue de 6 días (IC 95%: 2,16–9,84, con una mediana de 3) y de 7,6 días cuando estuvieron las 2dolencias asociadas (IC 95%: 4,14–10,9, mediana de 7) (valor p=0,024).
ConclusionesLos pacientes con TSV en el período neonatal tienen frecuentemente RGE, y esta asociación genera una mayor dificultad para el control de la taquicardia. El reflujo podría actuar como desencadenante o perpetuante de la arritmia, por eso es importante buscar y tratar el RGE en los recién nacidos con TSV.
Neonatal tachycardia is defined as a resting heart rate (HR) of 182 beats per minute (bpm) when the baby is not crying.1,2 Supraventricular tachycardia (SVT) is the most common tachyarrhythmia in the neonatal period and usually presents with a HR of more than 200bpm and with a narrow QRS complex. In 80% of patients, it originates through a mechanism of retrograde conduction via an accessory pathway between the ventricle and the atrium, with an abrupt onset and termination. In 15% of patients it results from atrial ectopic beats, while 5% of cases correspond to re-entrant nodal tachycardias.3,4 Approximately half of these patients present with heart failure, with suspicion of sepsis in some cases. The tachycardia may be detected in the foetal period, most frequently between weeks 28 and 33 of gestation, possibly manifesting with hydrops.5
The key element in the management of haemodynamically unstable patients with tachycardia is electric cardioversion. However, in stable patients, SVT is generally managed with a stepwise approach, starting with vagal manoeuvres and, should the patient not respond, initiation of pharmacological treatment with adenosine (0.03–0.25mg/kg) or ATP (0.05–0.1mg/kg), which cause a transient block in the atrioventricular node.6,7 If the patient does not respond to these drugs, treatment may continue with the administration of amiodarone, beta-blockers or digoxin. Flecainide and sotalol have proven effective in the management of refractory SVT.8,9 Supraventricular tachycardia frequently recurs after acute therapy (80%). Maintenance of antiarrhythmic prophylaxis is recommended in children aged less than 1 year because recurrent SVT may be difficult to detect in newborns and infants. Most patients are asymptomatic and require no further treatment by age 1 year.9,10
Gastro-oesophageal reflux is usually a physiologic process in newborns,11,12 although some cases may require pharmacological treatment for adequate control.13,14 Although there is no published evidence of an association between SVT and gastro-oesophageal reflux disease (GERD), the oesophagus is located immediately posterior to the left atrium, and the two structures share some innervations. In recent years, evidence has emerged of a potential association between the development of atrial fibrillation and GERD.15 Atrial fibrillation is the most common sustained arrhythmia in adults, and SVT is the most frequent one in children; their pathophysiology is nearly the same from a structural standpoint. Atrial fibrillation may result from vagal nerve overstimulation.16,17 Thus, it would be logical to hypothesise that the presence of acid in the oesophagus could trigger tachycardia.
The aim of this study was to assess whether the presence of GERD in the neonatal period may trigger SVT, and the impact of GERD on its adequate control.
Patients and methodsPatientsWe conducted a longitudinal retrospective study between January 2011 and December 2015 of children born in the Hospital Clínico Universitario of Santiago de Compostela (CHUS), a tertiary level hospital, who received a diagnosis of SVT based on the criteria of the International Classification of Diseases (ICD-10; http://www.who.int/classifications/icd/icdonlineversions/en/). We registered the study with the Research Ethics Committee of Galicia (2016/361).
We set the following inclusion criteria: infant born to term with a diagnosis of sustained tachycardia (resting HR without crying>182bpm). We excluded patients with a diagnosis of sinus tachycardia and infants born preterm.
We analysed the presence or absence of GERD. We retrieved data from the health records of patients and their mothers. We adhered to the protocols established by the hospital for access to health records. We collected data pertaining to the maternal and foetal history: preeclampsia, oligohydramnios or polyhydramnios, risk of preterm birth, disease or infection in the mother, gestational diabetes, maternal obesity, multiple pregnancy, maternal pharmacological treatment, smoking or alcohol use, and foetal tachyarrhythmia. We also analysed the perinatal history: gestational age, birth weight, sex of the newborn, neonatal respiratory depression and multiple birth. We also analysed the reason for admission to the neonatal unit, the mechanism of tachyarrhythmia and the heart rate at onset, the presence or absence of underlying structural malformations of the heart and, if present, whether they were accompanied by clinical manifestations. We analysed the drugs used to manage SVT and the time elapsed from diagnosis to control of tachycardia. We also documented the number of drugs needed to treat GERD in addition to postural therapy.
MethodsThe diagnosis of SVT was based on the features of electrocardiogram (ECG) displays viewed in a Philips Intellivue MP70 neonatal monitor (Netherlands), and confirmed by interpretation of paper printouts of 12-lead ECGs (Hewlett Packard PageWriter 300pi). Ultrasound examinations were performed by a paediatric cardiologist using a General Electrics ultrasound system.
Continuous 24-h intra-oesophageal pH monitoring was performed with 2 probes placed in the oesophagus and stomach (Digitrapper MKIII, Synectics Medical, Sweden). Reflux was diagnosed based on clinical manifestations and the results of intra-oesophageal pH monitoring, expressed by means of Vandenplas’ criteria18: reflux index (percentage of the monitoring time that acid was detected in the oesophagus); number of reflux episodes; number of reflux episodes lasting more than 5 minutes, and duration of longest episode. We applied the standards established for this age group to interpret test results.19
Statistical analysisWe performed the statistical analysis with SPSS version 20.0 (SPSS Inc; Chicago, IL, USA). We have expressed clinical and epidemiological variables as percentages or means and standard deviations. We checked the normality assumption by means of the Shapiro–Wilk test. We compared quantitative variables that did not follow a normal distribution with the nonparametric Mann–Whitney U test, and qualitative variables by means of the chi square test.
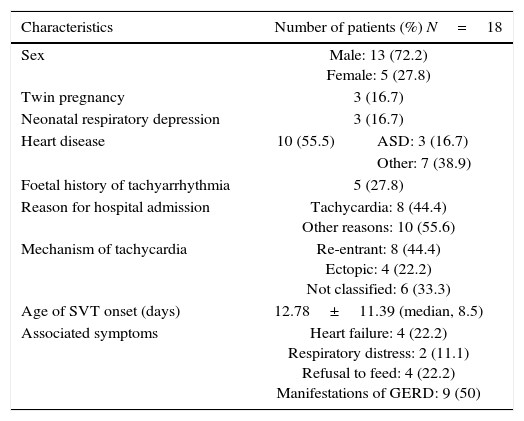
ResultsOf the total of 14,387 newborns delivered in our hospital in the 5-year period, 44 received a diagnosis of sustained tachycardia (3/1000). Eighteen of these tachycardia cases (41%; 1.2/1000) were classified as SVT (Table 1).
Characteristics of patients with supraventricular tachycardia.
| Characteristics | Number of patients (%) N=18 | |
|---|---|---|
| Sex | Male: 13 (72.2) Female: 5 (27.8) | |
| Twin pregnancy | 3 (16.7) | |
| Neonatal respiratory depression | 3 (16.7) | |
| Heart disease | 10 (55.5) | ASD: 3 (16.7) |
| Other: 7 (38.9) | ||
| Foetal history of tachyarrhythmia | 5 (27.8) | |
| Reason for hospital admission | Tachycardia: 8 (44.4) Other reasons: 10 (55.6) | |
| Mechanism of tachycardia | Re-entrant: 8 (44.4) Ectopic: 4 (22.2) Not classified: 6 (33.3) | |
| Age of SVT onset (days) | 12.78±11.39 (median, 8.5) | |
| Associated symptoms | Heart failure: 4 (22.2) Respiratory distress: 2 (11.1) Refusal to feed: 4 (22.2) Manifestations of GERD: 9 (50) | |
ASD, atrial septal defect; GERD, gastro-oesophageal reflux disease; SVT, supraventricular tachycardia.
We found some type of heart comorbidity in 55.6% of the patients with SVT. The most frequent cardiac comorbidities were atrial septal defects. Re-entry was the most frequent mechanism of tachycardia. The mean HR was 259bpm, and SVT presented as heart failure in only 22% of the patients. In 50%, the onset of tachycardia occurred when the patient had already been admitted, usually for reasons other than arrhythmia (low weight, neonatal respiratory depression, etc.). Different drugs were used to manage SVT. Adenosine was used as the first-line drug in 100% of patients, with or without previous performance of vagal manoeuvres (performed in 52.9%). The drugs used to control arrhythmia included flecainide (61.1%), propranolol (50%), digoxin (38.9%) and esmolol (33.3%). In our study, 71.4% of patients required 2 or more drugs to control the tachycardia.
Association with gastroesophageal refluxWe found records of fussiness during feedings, regurgitation and vomiting in 9 newborns (50% of cases) associated with GERD, which was confirmed by means of pH monitoring (P=.01). Gastrointestinal reflux was treated with prokinetic agents (domperidone), proton pump inhibitors (omeprazole) and antacids (almagate). A single drug was used for the symptomatic treatment of GERD in 33.3% (3/9) of cases, and with 2 drugs in 55.6% (5/9); only one patient required more than 2 drugs for control. The mean time elapsed from the diagnosis to the control of tachycardia in patients without GERD was 6 days (95% CI, 2.16–9.84), and the median was 3 days. However, the mean time elapsed in patients with associated GERD was 7.6 days (95% CI, 4.14–10.9), with a median of 7 days (P=.024) (Fig. 1).
Discussion
In this study, we investigated newborns with SVT to assess the association of this condition with GERD. The proportion of patients with SVT in the neonatal period that also had GERD was 50%, and this comorbidity was associated with an increased difficulty in controlling the tachycardia.
The prevalence of supraventricular tachycardia is low in the neonatal period, when its onset may go undetected, the symptoms are often nonspecific, and control is difficult to achieve, although the intermediate- to long-term prognosis is very good, as a high percentage of these patients are asymptomatic without treatment by age 1 year.20 In our study, we found a high incidence of heart disease (more than 50% of the patients had some type of structural anomaly) compared to other studies that reported percentages of structural heart disease between 7% and 19.7%.21,22 However, these diseases were not severe, and none of the patients died. In fact, heart failure was only documented in 4 (22.2%), in contrast to the 48% reported in other studies.21
The approach to the management of tachycardia did not differ from the clinical guidelines published by the American College of Cardiology, American Heart Association and European Society of Cardiology in either the acute phase or the maintenance phase.8 The management was fundamentally based on the condition of the patient. Adenosine was the first drug administered to every patient, as they were all haemodynamically stable. As regards maintenance treatment, the most recent recommendations support the use of flecainide as one of the most effective drugs for long-term control of neonatal SVTs, since it is very effective in preventing recurrence and has few side effects in patients with healthy hearts. In our patients, the most frequent pharmacological treatment was flecainide in combination with a beta blocker, and it was highly effective in controlling arrhythmia. Up to 71.4% of patients require 2 or more drugs for tachycardia control. Following the appropriate adjustments in the selection of drugs and their dosage, patients usually remain asymptomatic until treatment can be discontinued. Etheridge and Judd reported that 76% of the patients they followed up until age 1 year no longer needed medication and were free from SVT.20
We found a significant association between GERD and SVT in newborns (P=.01). This may be explained by the anatomical relationship of the oesophagus and the heart, as the thoracic portion of the oesophagus is right behind the left atrium, and the potential stimulus of acid at this level could act as a trigger or perpetuator of SVT. A current study published on behalf of the European Society of Cardiology discusses potential atrial arrhythmogenic mechanisms in patients with GERD, such as inflammation, impaired autonomic stimulation or mechanical irritation due to anatomical proximity.23 Furthermore, there is evidence that failure to diagnose GERD could hinder the management of SVT. The time elapsed to the control of tachycardia in patients with GERD is longer compared to patients without GERD, which suggests that it is more difficult to control arrhythmia when it is associated with reflux.
This study is the first to demonstrate a causal link between GERD and SVT in newborns. Although the sample was small, it is important to take this risk factor into account in order to optimise treatment and improve outcomes. Prospective multicentric studies are needed to confirm our results and determine the degree of causality or strength of the association of GERD in the development of SVT during the neonatal period.
ConclusionsOur study found an association between GERD and SVT in the neonatal period, and that this association resulted in an increased difficulty in controlling tachycardia with pharmacological treatment. Thus, it is important to consider the potential presence and appropriate treatment of GERD in newborns with SVT to reduce the duration of arrhythmia and prevent potential complications.
Conflict of interestThe authors have no conflict of interests to declare.
Please cite this article as: Fuertes Á, Alshweki A, Pérez-Muñuzuri A, Couce M-L. Taquicardia supraventricular en recién nacidos y su asociación con reflujo gastroesofágico. An Pediatr (Barc). 2017;87:206–210.
