




Autoimmune enteropathy (AIE) is a rare cause of severe diarrhoea associated with immune dysregulation and characterised by the presence of antibodies and autoimmune disorders.
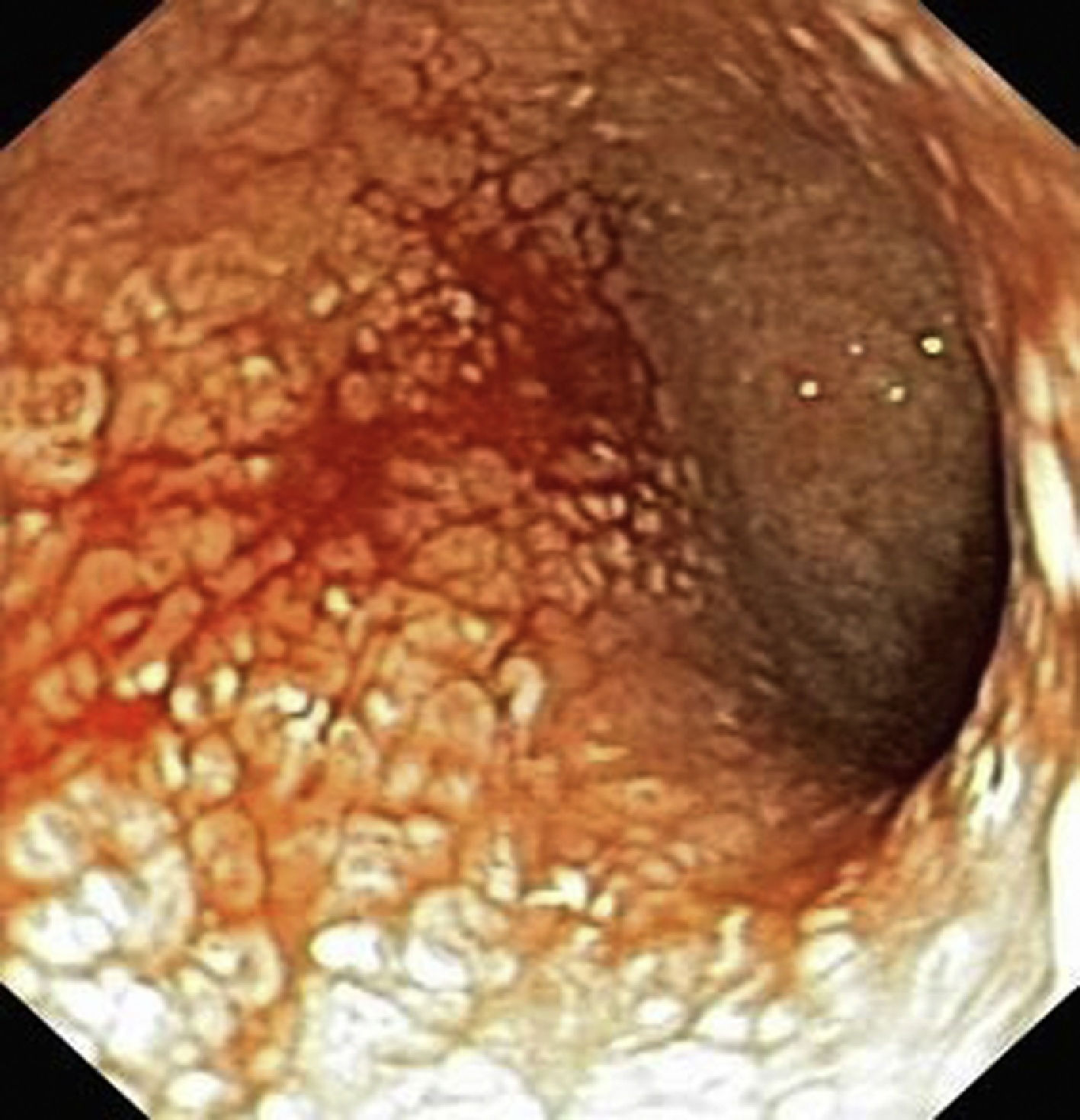
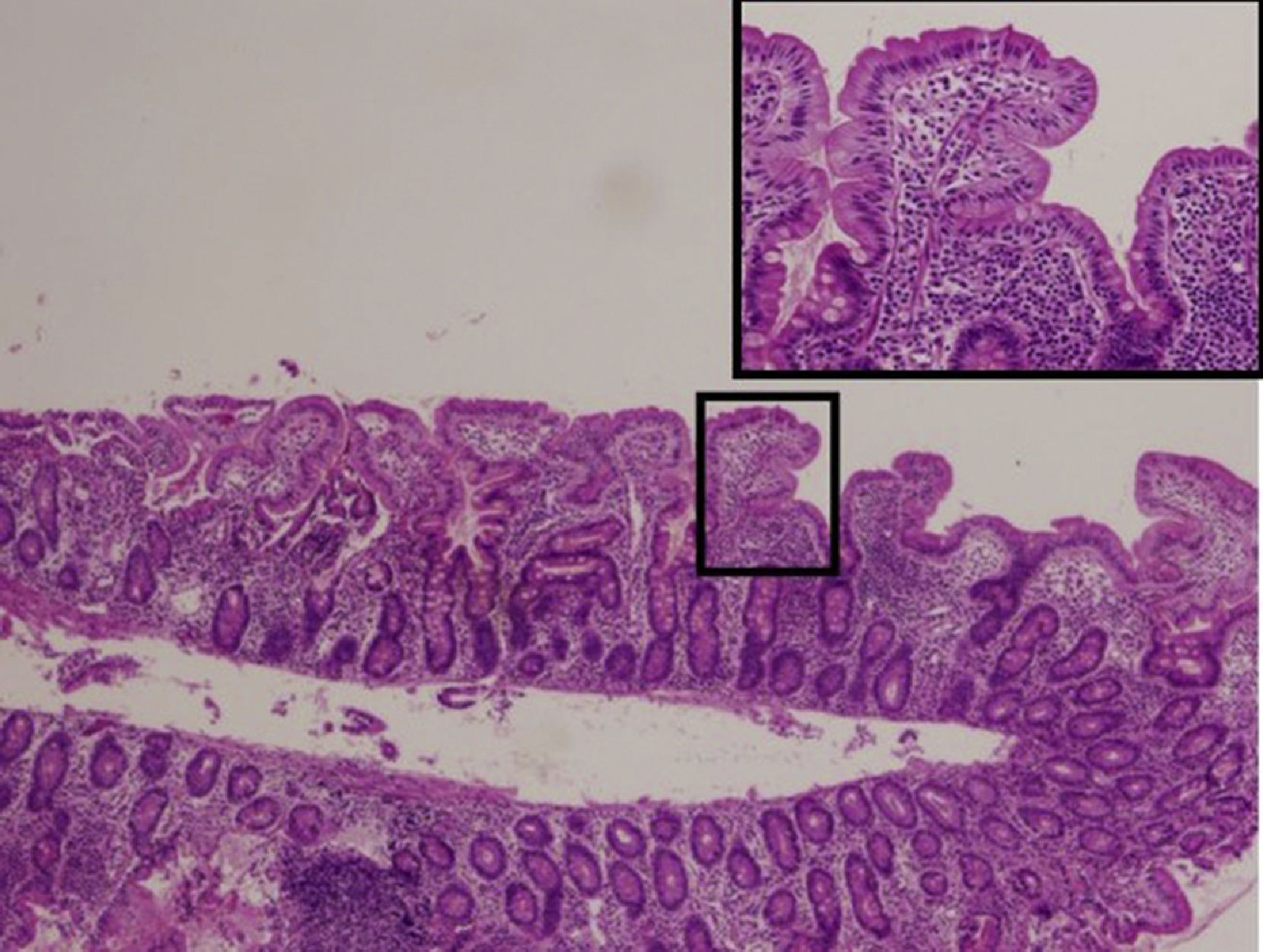
We performed a retrospective review of the cases of AIE diagnosed in our hospital between 1975 and 2015. A total of 8 patients received the diagnosis during this period. Seventy-five percent were male. The age of onset was less than 3 months in five patients (62.5%), 15 months in one (12.5%), 2 years in one (12.5%) and 7 years in one (12.5%). The most frequent symptoms were severe mixed-type diarrhoea (exudative/secretory), with bloody stools in 4 patients, weight faltering, found in 100% of the patients, and vomiting, present in 5 (62.5%). Serum albumin levels were elevated in all patients, and faecal calprotectin in every patient in whom it was measured (62.5%). Four patients had decreased levels of IgG and one had selective IgA deficiency. Three patients tested positive for anti-enterocyte antibodies. The endoscopic examination revealed an atrophic gastric mucosa with erosions in 75%, granularity and friability of the duodenal mucosa in 100% (Fig. 1), and a friable colonic mucosa with loss of the normal vascular pattern in 62.5%. The histological examination revealed atrophic gastritis, villous atrophy of variable severity with crypt hyperplasia and mononuclear cell infiltration in the duodenum (Fig. 2), and ulcerations in the colon.
Three patients had mutations in the FOXP3 gene (IPEX syndrome), and one in the CTLA4 and caspase 10 genes (autoimmune lymphoproliferative syndrome). The autoimmune comorbidities found in these patients were: nephropathy in 2, hepatitis in 1, thyroiditis in 2, cytopaenia in 1 and type 1 diabetes mellitus in 1. All patients received steroid therapy, with a partial and transient response. This led to the use of alternative agents: azathioprine, tacrolimus, sirolimus, infliximab, adalimumab, cyclosporine, cyclophosphamide, thymoglobulin and mercaptopurine. At the time of this writing, 5 patients remained in remission under immunosuppressive therapy, 2 had transitioned to adult care, and 1 had died of septic shock.
Autoimmune enteropathy is a rare disease that may have onset in childhood and is characterised by intractable diarrhoea and immune dysregulation syndrome. It was first described as a distinct entity in 1982 by Walker-Smith et al. in a boy aged 9 years, although McCarthy et al. had already described the clinical picture in a boy with IgA deficiency in 1978. It manifests with chronic and intractable diarrhoea in infants following an uncomplicated gestation and neonatal period. Cases with onset in adolescence and adulthood have also been described.1 It is generally believed to predominantly affect males, but Singhi et al. found a similar prevalence in both sexes in a large case series that was published recently.2 The differential diagnosis must include diarrhoea of infectious or allergic aetiology and other, less frequent diseases such as microvillus inclusion disease or intestinal epithelial dysplasia.
The pathogenesis of AIE is unknown. It has been hypothesised that it involves changes in T cell activation, but larger studies are required to elucidate the exact underlying mechanisms.3
The presence of anti-enterocyte antibodies is not a specific finding, as they are also detected in other conditions such as inflammatory bowel disease, HIV infection and allergic enteropathy.4 Furthermore, the antibody titre is not correlated to the degree of mucosal damage. An association with other autoimmune disorders of the endocrine system, lung, liver, blood or other systems is frequently found in these patients, as was the case in our series.
Immunodysregulation polyendocrinopathy enteropathy X-linked (IPEX) syndrome, caused by a mutation in the FOXP3 gene, and autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) syndrome, caused by mutations in the AIRE gene, frequently cause AIE.
Autoimmune enteropathy usually involves the small intestine, although gastric and colonic involvement are not rare. In our series, we found gastric atrophy in most patients, and colonic involvement in 3. The histological examination revealed villous atrophy with crypt hyperplasia and a marked T cell infiltrate in the intestinal mucosa. Crypt apoptosis is characteristic of AIE.5
The management of AIE in children is based on providing the necessary nutritional support to ensure adequate growth. These patients also require immunosuppressive therapy, with corticosteroids being the first-line treatment, although steroid resistance is frequent. In cases where steroid therapy fails, alternative immunosuppressive agents are used, such as cyclosporine, tacrolimus, sirolimus or mycophenolate, with variable results. In addition, some authors have proposed the use of biologic agents after observing good outcomes in clinical practice.6
To conclude, AIE is a rare cause of severe mixed-type diarrhoea with protein-losing enteropathy. It can involve the entire gastrointestinal tract and is frequently associated with other autoimmune diseases. Further research is required to elucidate the underlying mechanisms of the disease and improve its management.
Please cite this article as: Lázaro de Lucas C, Rodríguez LT, García LN, Martínez-Ojinaga Nodal E, Boluda ER. Diarrea grave por enteropatía autoinmune: tratamiento y evolución. An Pediatr (Barc). 2018;88:350–351.
