




The term malnutrition includes malnutrition due to excess or obesity, underweight as well as stunted growth. Its prevalence in a population can be estimated using anthropometric variables. The aim of this study is to estimate the prevalence of malnutrition in Galician schoolchildren aged 6–15 years in the school year 2013–2014.
MethodsA cross-sectional study was conducted on a representative sample by gender and age of the Galician population of 6–15 years old. The prevalence of obesity, underweight, and short stature was estimated by age and gender using the reference standards proposed by the World Health Organisation.
Results7438 schoolchildren weighed and measured 16,4% presented malnutrition. The prevalence of obesity was 14.8%, underweight was 0.7%, and short stature for age was estimated at 1%. Obesity was more prevalent among boys. As regards underweight and short stature, when there were differences, prevalence was higher among girls.
ConclusionsIn Galicia, 16 out of every 100 schoolchildren aged 6–15 years had malnutrition, with that due to excess or obesity being the most frequent. Prevalence of underweight and short stature did not exceed 1%. This data shows that primary prevention measures should be promoted at an early age to reduce malnutrition due to excess or adiposity, in particular.
Bajo el término malnutrición se agrupa la malnutrición por exceso, por defecto y por retraso en el crecimiento. Su prevalencia, a nivel poblacional, se puede estimar mediante variables antropométricas. El objetivo de este trabajo es estimar la prevalencia de malnutrición en los escolares gallegos de 6 a 15 años en el curso escolar 2013–2014.
MétodosEstudio transversal sobre una muestra representativa por sexo y edad de la población gallega de 6 a 15 años. Se estimó la prevalencia de obesidad, bajo peso y baja estatura en función del sexo y la edad utilizando los criterios de referencia propuestos por la Organización Mundial de la Salud.
ResultadosSe pesaron y midieron 7.438 escolares. En global, el 16,4% de los escolares presentaban malnutrición. La prevalencia de obesidad fue del 14,8%, la de bajo peso, del 0,7%, y la de baja estatura para la edad, del 1%. La obesidad fue más prevalente entre los niños; respecto al bajo peso o baja estatura cuando aparecieron diferencias, las prevalencias fueron más altas entre las niñas.
ConclusionesEn Galicia, 16 de cada 100 escolares de 6 a 15años presentaban malnutrición, siendo la malnutrición por exceso u obesidad la manifestación más frecuente. La prevalencia de bajo peso y baja estatura no superaron el 1%. Estos datos ponen de manifiesto que se deben promover medidas de prevención primaria a edades tempranas encaminadas a disminuir la malnutrición, especialmente por exceso o adiposidad.
Malnutrition is a term that may refer to a negative energy balance (undernutrition, or underweight) or to a positive energy balance (overnutrition, or obesity). At the population level, while the approach has some limitations, the prevalence of malnutrition can be estimated using anthropometrics.1 Thus, weight and height are the indicators used most frequently to assess nutritional status in children at the population level.
There is evidence that in developed countries, socioeconomic differences are associated with malnutrition in children and adolescents, with the risk of malnutrition increasing with decreasing socioeconomic status.2,3 In Spain, there was an inflection point in employment trends in 2007, after which the level of unemployment increased.4 As mean household incomes dropped, poverty increased and private consumption decreased. The economic crisis led to an increase in the number of households living below the poverty threshold,5 and in these households, the scarcity of resources may be associated with a decrease in the availability or quality of foods and an increase in the risk of malnutrition,6 which is associated with significant nutritional deficiencies. This is a very important aspect to consider in relation to vulnerable groups, such as children.7
In 2013, UNICEF published a report that ranked Spain among the European countries with percentages of children at risk of child poverty greater than the European average (29.8% vs 27.1%).8 In 2014, the at-risk-of-poverty rate in Spain based on data from the Encuesta de Condiciones de Vida (Survey of Living Conditions) was 22.2%, and the corresponding rate for children was 30.1%.5 Based on the same survey, the at-risk-of poverty rate in Galicia was among the lowest in Spain at 15.4%. Nevertheless, these data indicated that 420000 inhabitants were at risk in Galicia. Malnutrition does not occur in the entire population at risk of poverty. The data of the survey of living conditions revealed that in 2014, 3.3% of the Spanish population could not afford a meal with red meat, chicken or fish at least every 2 days, a percentage that rose to 4.2% in individuals aged less than 16 years. In Galicia, the percentage of the population that suffered material deprivation related to nutrition was 1.8%, and this was the autonomous community with the lowest percentage following Aragon and the Basque Country.5
The prevalence of child malnutrition at the population level in Galicia has not been determined to date. The aim of our study was to establish the prevalence of malnutrition in Galician schoolchildren aged 6–15 years during the 2013–2014 school year using objective anthropometric measures based on weight and height.
MethodsIn order to estimate the prevalence of malnutrition in Galician children and adolescents, we designed a cross-sectional study among schoolchildren aged 6–15 years enrolled in any of the 6 years of Primary Education (PE) or the 4 years of Compulsory Secondary Education (Educación Secundaria Obligatoria [ESO]) in public or private schools in Galicia during the 2013–2014 school year. We selected participants by stratified two-stage cluster sampling. In the first stage, we selected schools offering PE and/or ESO, and in the second stage, we selected 3 classrooms of PE and/or 2 of ESO in each of the previously selected schools. We included in the study all students of the selected classes aged 6–15 years. We calculated the sample size separately for each school year under simple random sampling assumption. In all sample calculations, we assumed that 22000 children were enrolled in each school year in Galicia and a prevalence of obesity of 10%, and we made the calculation for a 95% confidence interval, a precision of 2.8% and a design effect of 1.5. We increased the estimated sample sizes by 10% for PE students and 15% for ESO students to compensate for potential missing data due to refusal to participate. The final target sample sizes were 4500 PE students and 3200 ESO students. Based on these targets, we determined that we needed to select 417 classrooms and 137 schools.
After requesting the informed consent of parents, 9 teams, each composed of 2 previously trained members, visited the sites during school hours. The schoolchildren were weighed wearing light clothing and with bare feet with a Seca scale accurate to 0.1kg, and their heights measured with the head in the Frankfort plane using a portable Tanita stadiometer with a fixed base plate accurate to 0.1cm. The fieldwork was conducted in October and November 2013.
We estimated malnutrition using the obtained anthropometric measurements and applying the cut-off points proposed by the World Health Organisation (WHO): short stature (weight for age and sex <−2 SD) and underweight (body mass index [BMI] for age and sex <−2 SD). We estimated malnutrition by excess based on the prevalence of obesity (BMI for age and sex ≥+2 SD).9
We present the calculated prevalence values with their 95% confidence intervals (CIs). We compared proportions by means of the Pearson chi square test weighted to adjust for the sampling design. We performed the statistical analysis with the software STATA 12. We have presented the estimates by sex, age, and age group (6–11 years; 12–15 years).
ResultsWe obtained data for 7438 students, of whom 4434 were aged 6–11 years, the age range corresponding to PE, and 3004 were aged 12–15 years, the range corresponding to ESO. The proportion of students that accepted to participate in the study was 91.4%.
Overall, 16.4% (15.2–17.5) of Galician schoolchildren had obesity, underweight or stunted growth. The prevalence was higher in male students (19.2% [17.8–20.7%] vs 13.3% [11.9–14.8%]) and children aged 6–11 years (18.5% [16.9–20.0%] vs 13.1% [11.6–14.4%]).
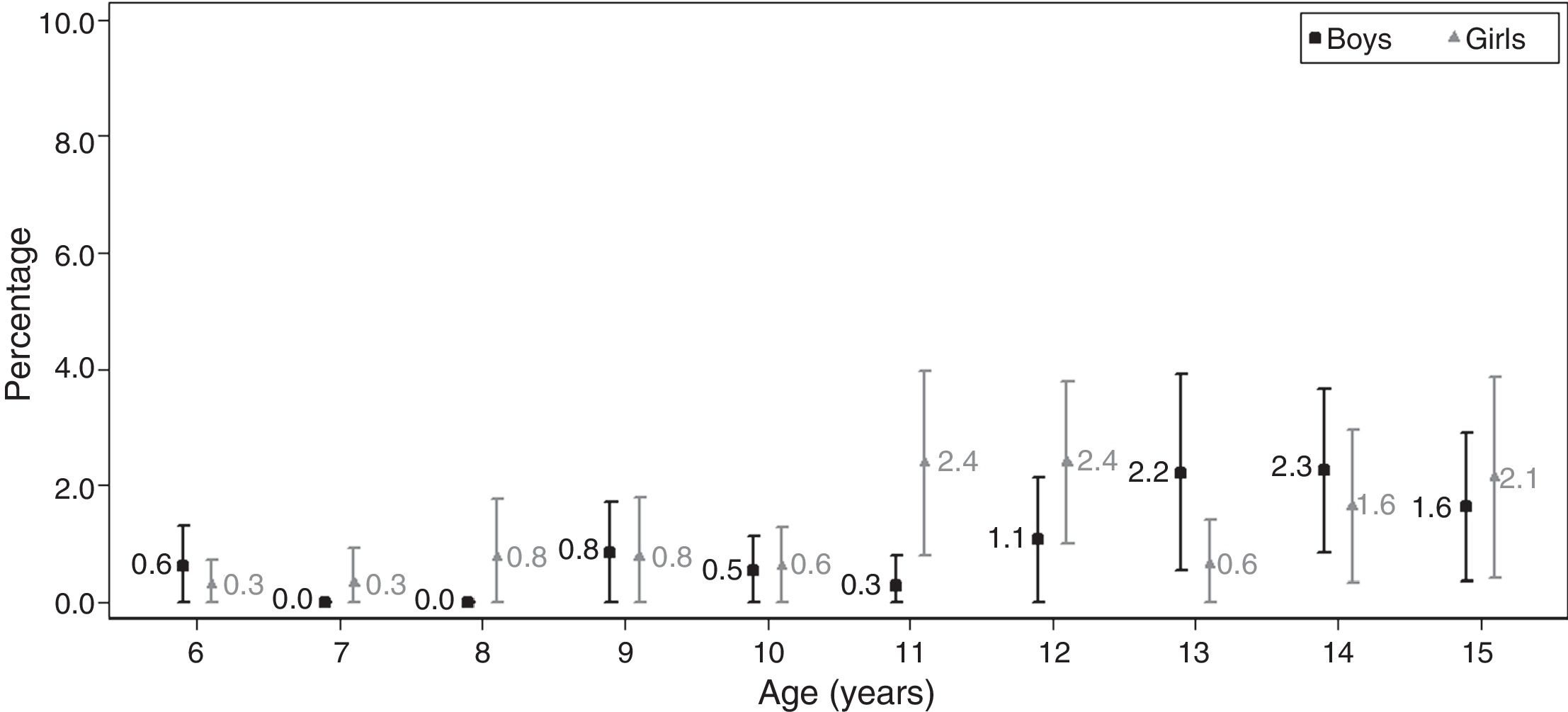
Short stature for age was present in 1.0% (0.8–1.3%) of Galician students aged 6–15 years, and we found no difference between sexes (P≥.05). When it came to age, we found that short stature was less frequent in schoolchildren aged 6–11 years (0.6% vs 1.7%). We found differences between the sexes in the 6–11 years age group, with a higher prevalence in girls (Table 1). Taking age into account, we found that the prevalence of short stature in boys peaked at 13–14 years of age, while in girls it peaked at 11–12 years of age (Fig. 1).
Prevalence of malnutrition (underweight, obesity or short stature) by age group, overall and by sex. Cut-off points: WHO, 2007.
| Total | Boys | Girls | P* | ||||
|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | ||
| 6–11 years | |||||||
| Underweight (BMI<−2 SD) | 0.5 | 0.3–0.7 | 0.3 | 0.1–0.5 | 0.8 | 0.4–1.2 | .014 |
| Obesity (BMI≥2 SD) | 17.4 | 16–18.9 | 21.0 | 19.1–22.8 | 13.7 | 11.7–15.6 | .000 |
| Height-for-age<−2 SD | 0.6 | 0.4–0.8 | 0.4 | 0.2–0.6 | 0.8 | 0.5–1.2 | .033 |
| 12–15 years | |||||||
| Underweight (BMI<−2 SD) | 0.9 | 0.5–1.3 | 0.6 | 0.2–1.1 | 1.2 | 0.6–1.8 | .135 |
| Obesity (BMI≥2 SD) | 10.5 | 9.3–11.8 | 13.3 | 11.4–15.2 | 7.6 | 5.9–9.3 | .000 |
| Height-for-age<−2 SD | 1.7 | 1.2–2.2 | 1.8 | 1.1–2.5 | 1.7 | 1–2.4 | .883 |
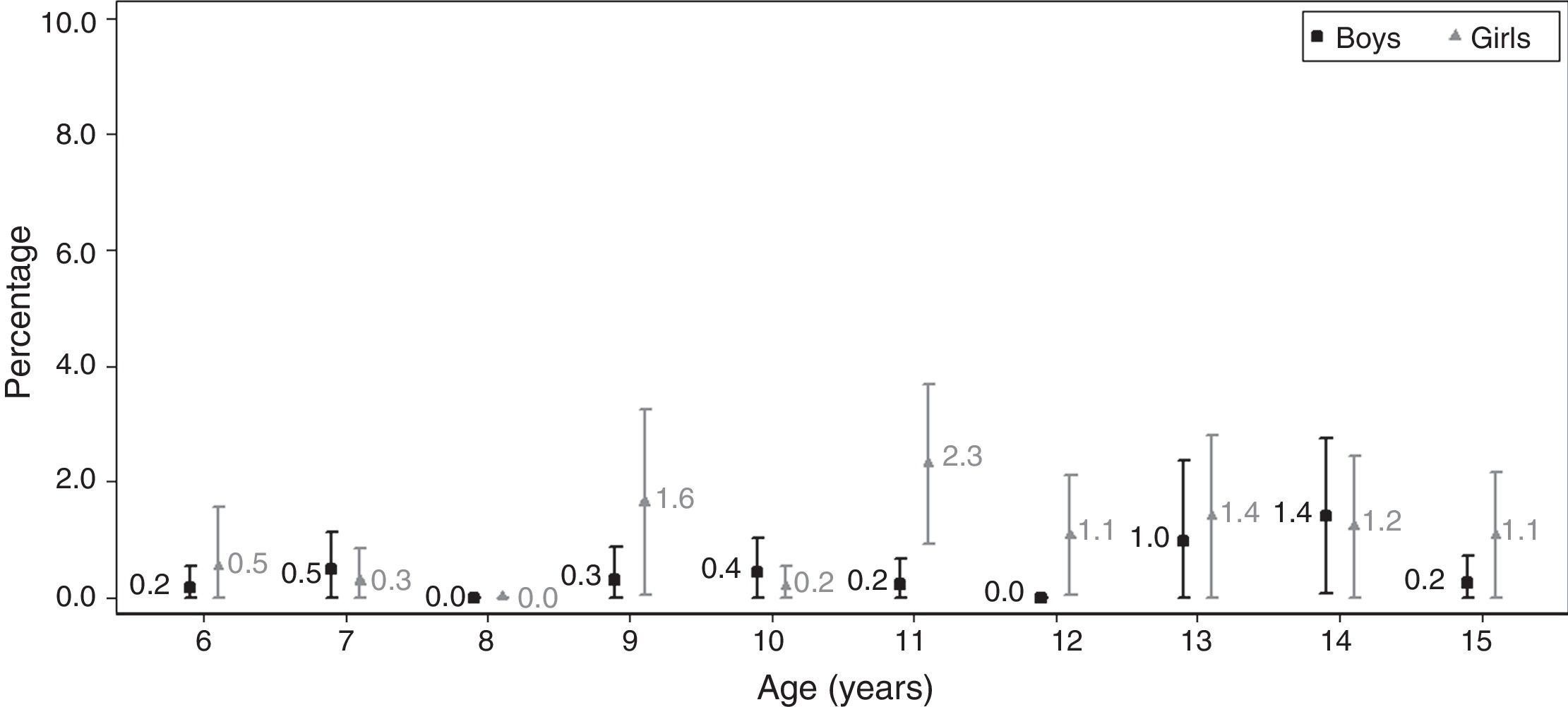
Underweight was detected in 0.7% (0.5–0.9%) of Galician schoolchildren aged 6–15 years. The prevalence was higher in girls (0.4% [0.2–0.6%] vs 1% [0.6–1.3%]). By age group, the prevalence was higher in students aged 12–15 years, with no difference between the sexes (P≥.05); in the 6–11 years age group, the prevalence was higher in girls (P<.05) (Table 1). Taking sex into account showed that the prevalence peaked at age 11 years in girls and at age 13–14 years in boys (Fig. 2).
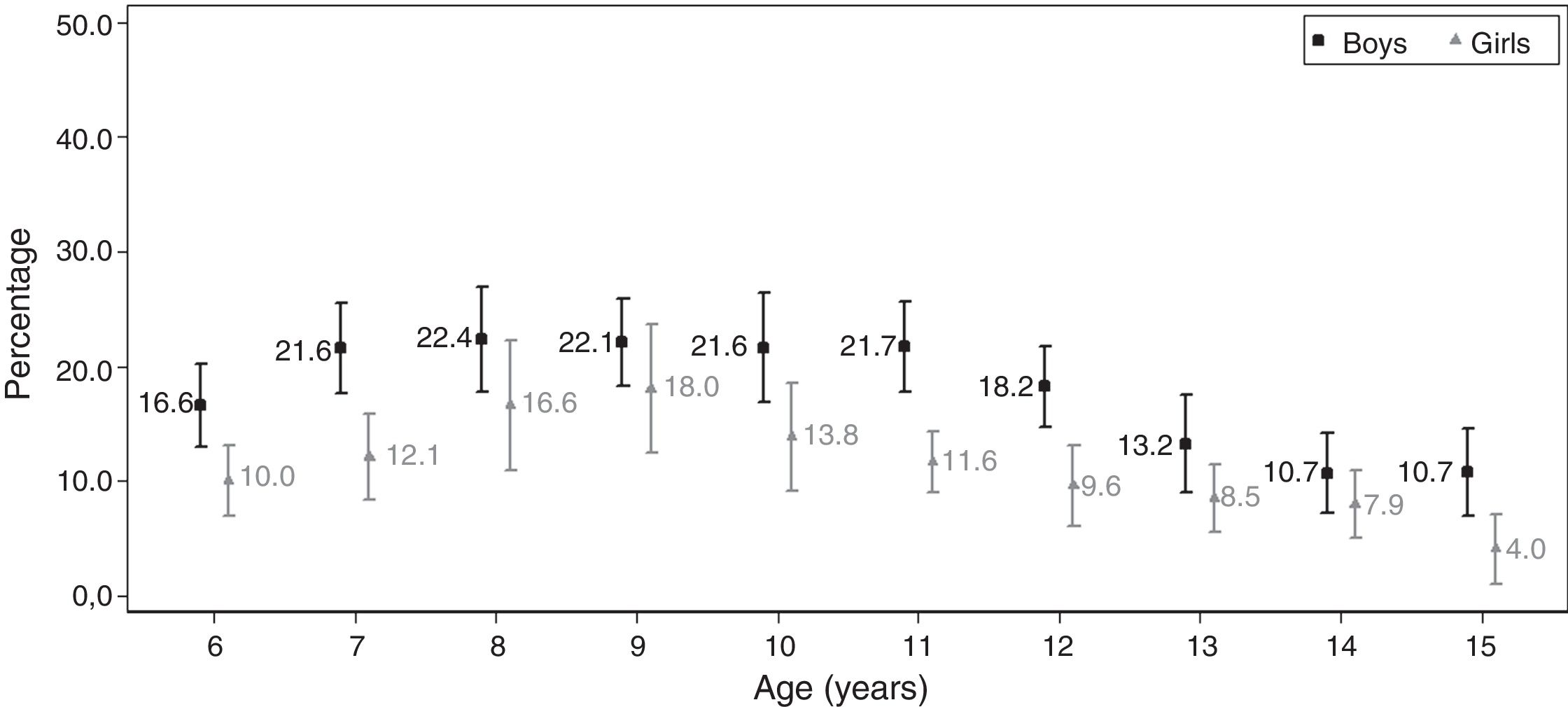
We found obesity in 14.8% (13.7–15.9%) of Galician schoolchildren aged 6–15 years, and the prevalence was higher in boys (18.0% [16.6–19.5%] vs 11.4% [9.9–12.8%]; P<.05), regardless of age group. The prevalence of obesity was 66% higher (P<.05) in schoolchildren aged 6–11 year (Table 1). By age, we found that the prevalence of obesity peaked between ages 7 and 11 years in boys, and ages 8 and 9 years in girls (Fig. 3).
We found no differences in the prevalence of malnutrition based on the type of school (public vs private) or between provinces (data not shown).
DiscussionWe estimate that 16 out of 100 schoolchildren aged 6–15 years in Galicia had malnutrition (manifesting as obesity, underweight or stunted growth). Although the prevalence of short stature and underweight did not exceed 1% at any age, based on the 2013 population census data, we estimate that 1683 (1262–2104) schoolchildren aged 6–15 years had short stature and 1266 (871–1660) were underweight for their age. When it came to overnutrition, our estimates were cause for concern, as the prevalence of obesity was 15% using the cut-off point recommended by the WHO, which means that 29040 (25934–32147) schoolchildren in Galicia aged 6–15 years would have been obese.
Height gain, whose assessment is essential in paediatric checkups, is an indicator influenced by multiple factors, such as chronic or metabolic disease and environmental factors, which include social factors with an impact on the child, such as emotional or economic deprivation. It is also important to consider constitutional growth delay. Deficiencies in the intake of micronutrients could also play a role in height gain, although a lesser one, so their inclusion as indicators of malnutrition in developed countries may be questionable. Most published studies on short stature for age have been conducted in children aged 0–5 years or in developing countries,10 which makes it difficult to compare their findings with ours. A cross-sectional study published in 2003 analysed the weight and height measurements reported by parents of schoolchildren aged 11 years and older in 9 European countries.11 This study identified Spain—represented by 745 Spanish schoolchildren—as the country with the highest prevalence of short stature for age following Portugal. The study estimated that 5.1% (3.1–7.8%) of girls and 3.4% (1.8–5.7%) of boys in Spain had short stature at age 11 years. The overall prevalence in the included European countries was 2.8% in girls and 1.4% in boys. When we estimated the prevalence of short stature in Galicia 12 years later using the same cut-off points12 and in children aged 11 years (789 schoolchildren in our sample), the prevalence of short stature was lower than the prevalence estimated in the study by Yngve et al.11 for Spain overall, and similar to the overall prevalence in the studied European countries (3.8% [1.6–5.9%] in girls and 1.4% [0.1–2.6%] in boys).
The prevalence of underweight in Galician schoolchildren increased with age, although it only exceeded 2% in girls aged 11 years (2.3%). The values we obtained were similar to those estimated in populations of similar age in other developed countries,13,14 although making comparisons is difficult, as the definition of underweight varies between studies. Thus, in a study conducted in France in 2000,13 the estimated prevalence of underweight, using the 5th percentile of the CDC tables as the threshold,12 was 4.3% in girls and 4% in boys at age 7 years; in our study in Galicia, if we were to apply the same cut-off point, the prevalence 13 years later would be lower (1.3% in boys and 2.5% in girls). The study in France found that the prevalence of underweight increased with age, reaching 7.7% in girls and 7.9% in boys at age 9 years. In our study in Galicia, the prevalence also increased with age in girls, reaching 2.3% at age 9 years; however, boys exhibited a decreasing trend, with the prevalence dropping to 2.1% at this age.
In recent years, the prevalence of obesity in children and adolescents has increased in developed countries,15 and several studies have evinced the considerable impact of social inequalities on obesity.16 Obesity, considered to reflect overnutrition, constitutes the manifestation of the most frequent type of malnutrition in developed countries both in adults and children. In Galicia, obesity affects approximately 15 out of 100 schoolchildren. When we compared our results with those of other studies that applied the same cut-off points, we found that the percentages were similar to those calculated for Spain in 2012 (12.6% in children aged 8–17 years),17 for Catalonia for the 2010–2012 period (15.4% in children aged 2–14 years)18 and those in the United States for the 2011–2012 period (with a prevalence of obesity of 17.3% in individuals aged 2–19 years).19 Previous studies in Galicia have estimated the prevalence of obesity, although they were conducted in specific age groups,20 specific geographical areas21 or provided data that need to be updated.22
Some authors question the approach of estimating the prevalence of malnutrition in developed countries based on height- or BMI-for-age, as the resulting estimates are not robust. Using a combination of indicators is one possible way of increasing accuracy.23 If undernutrition were defined as a combination of short stature and low weight for age, the prevalence would be near 0; in our study, for instance, only 2 children met both criteria. If we considered short stature and obesity for age and sex, the prevalence in our study would be 0.1%, with 7 children fulfilling both criteria.
There are various limitations to this study. Our results are based on a cross-sectional study with a single measurement per child, and we do not have follow-up data to assess weight and height gains, which could reveal changes or reductions in individual growth rates. Our results are estimates of various parameters in different age groups, although we have presented our findings as if they corresponded to a cohort. Furthermore, we must underscore that the indicators analysed cannot be used to identify the cause of malnutrition, which in some cases could be associated to an underlying disease. Another important limitation is that the cut-off points to assess differences in anthropometric measurements in the paediatric age group are not universal, so that reported prevalences vary according to the standard applied. For instance, we showed estimates calculated with the reference standards provided by the CDC earlier in this discussion. The prevalences obtained with these standards were 3.8% (1.6–5.9%) in girls and 1.4% (0.1–2.6%) in boys at age 11 years, compared to 2.4% (0.8–4.0%) in girls and 0.3% (0–0.8%) in boys using the WHO cut-off points, which were the reference used in our study. Another limitation is the potential for selection bias due to differential participation, as schoolchildren that deviate from average in weight or height may be less likely to participate. In our study, 91.4% of children agreed to participate, and we verified that the impact of non-participation on the estimation of prevalence was low.24 Given the cross-sectional design of our study and the lack of previous data, we were unable to determine whether the economic crisis had an impact on the estimated prevalences, although we would expect it to be so, as several studies have found increases in the prevalence of malnutrition, especially in terms of an increase in adiposity in individuals of low socioeconomic level.2,3
There are several strengths to our study. The sample size is one of them, as we calculated it to guarantee accurate estimates by school year and therefore by age. The age distribution of the final sample matched our expectations, with a mean sample size per year of 744 schoolchildren, a minimum of 592 at age 8 years and a maximum of 909 at age 6 years. This guarantees that the sample is representative for both sexes and for every age included in the estimates. Our estimates were calculated using objective measurements obtained by previously trained individuals, which guaranteed the quality of the data and low intra- and inter-rater variability. The sampling frame consisted of the schools in Galicia, which gave us access to the study universe, the population aged 6–15 years, as schooling is legally mandated in this age group.
Determining the prevalence of malnutrition at the population level in developed countries poses challenges, but it should nevertheless be attempted. The prevalence of malnutrition in a population should be assessed by specific studies conducted in the clinical setting. Despite its intrinsic limitations, anthropometry is the only approach that allows us to obtain estimates at the population level, and collecting anthropometric data is of vital importance, as it can inform the development of health promotion and disease prevention programmes and identify vulnerable groups. In this regard, schools play a key role both in the detection of cases and in their management,25 so we need to raise awareness in educators about malnutrition and engage them in the early detection and management of this health problem.
Conflict of interestThe authors have no conflicts of interest to declare.
We thank Dr Mercedes de Onís for her significant contributions to the manuscript.
Please cite this article as: Pérez-Ríos M, Santiago-Pérez MI, Leis R, Malvar A, Suanzes J, Hervada X. Prevalencia de malnutrición en escolares españoles. An Pediatr (Barc). 2018;89:44–49.
