
Physical activity (PA), screen time (ST), and sleep are modifiable lifestyle habits for health. The objectives of this study were: (a) to examine the association between PA, ST, and both, on sleep patterns; and (b) to determine the influence of PA and ST on sleep problems in Chilean girls.
Patients and methodsThe study involved 196 children (12.2 years). Patterns and sleep problems were assessed using the Spanish version of the Sleep Self-Report, and the PA through the Physical Activity Questionnaire for Adolescents (PAQ-A), both in Castilian. The ST was assessed using several questions about television, game console and computer use.
ResultsThe ST recommendation (<2h a day) was exceeded by 63.2% of the girls. In general, the most active girls (last quartile) that did not exceed the recommendations of ST reported higher sleep quality and total score values compared to those who did not meet both. The logistic regression analysis showed that girls who did not meet both habits were more likely to have sleep quality (odds ratio=17.8, P=0.018), and general sleep problems (odds ratio=7.85, P=0.025).
ConclusionsParents need to set limits on sedentary leisure time and encourage more active habits, as sleep is a parameter closely linked to a better health profile in youth.
La actividad física (AF), el tiempo de pantalla (TP) y el sueño son hábitos de vida modificables relacionados con la salud. Los objetivos de este estudio fueron: a) examinar la asociación entre la AF y el TP y ambos con los hábitos de sueño; b) determinar la influencia de los hábitos de AF y el TP sobre los problemas asociados al sueño en niñas chilenas.
Pacientes y métodosEl estudio involucró a 196 niñas (12,2 años). Los hábitos de sueño fueron evaluados con el cuestionario Self-report sleep y la AF con el Physical activity questionnaire for adolescents, ambos en castellano. El TP se evaluó a través de diversas preguntas sobre el tiempo de uso de la televisión, videoconsola y ordenador.
ResultadosEl 63,2% de las niñas excedieron el límite recomendado de 2h al día de TP. En general, las niñas más activas (último cuartil) que no excedían las recomendaciones de TP reportaban valores más altos de calidad del sueño y puntuación total respecto a las que no cumplían ambas. El análisis de regresión logística mostró que las niñas que no cumplían ambos hábitos tenían mayor probabilidad de presentar problemas asociados a su calidad del sueño (odds ratio=17,8; p=0,018) y sueño general (odds ratio=7,85; p=0,025).
ConclusionesParece necesario que los padres establezcan límites respecto a las horas de ocio sedentario y favorezcan un mayor hábito activo, puesto que el sueño es un parámetro íntimamente ligado a un mejor perfil saludable en niños.
Inadequate sleep in childhood has important consequences on health.1 It is also associated with attention difficulties, cognitive disorders, poor academic performance and mood disorders.2 In this regard, sleep deprivation and sleep disorders are common in young adults and adolescents worldwide.3 In recent years, sleep deprivation has also attracted interest as a potential contributor to the obesity epidemic in children and adolescents.4 Along with research on sleep duration, several studies have also investigated sleep quality.5,6
There is a wide range of lifestyle factors that influence sleep duration and quality in young individuals, among which are physical activity (PA) and health-related habits such as screen time (ST).7,8 The current literature on PA offers inconclusive and inconsistent findings.5,9–12 On the other hand, new technologies and the patterns of their use are changing rapidly and deserve more attention due to their impact on sleep and wellbeing.7 Studies on this subject suggest that more than two hours a day of ST may negatively impact children,13 as it is associated with delayed sleep onset, night wakings, sleep-related anxiety and shortened sleep duration.14,15
Although multiple studies have focused on physical exercise and ST separately, there is little evidence on the adherence to PA and ST recommendations and its relationship with sleep quality in youth. In this regard, girls seem to be an ideal target for the promotion of healthy habits, given their low levels of PA16 and poorer sleep habits (especially sleep-related anxiety)17 compared to their male peers. Thus, the objectives of this study were: (a) to study the association between PA, ST and both with sleep habits; (b) determine the influence of PA and ST habits on sleep problems in Chilean girls.
Patients and methodsPatientsWe conducted a cross-sectional descriptive study. We requested the participation of all the female students enrolled in the seventh year of primary school in seven schools in the region of Maule (Chile), and 196 (89%) accepted. The participants attended public, partially subsidised and private schools in rural areas. The study had a convenience sample. We excluded girls that had special education needs or any disorder that limited their ability to engage in physical activity. The study protocol was approved by the Ethics Committee of the Universidad Autónoma de Chile and later on by the principal of each school. After obtaining approval, we sent a letter to the parents of all children in seventh grade inviting them to a meeting where we informed them of the objectives of the study and obtained their written consent for the participation of their children in the study. Lastly, we collected all the signed forms and the researchers met with the physical education teacher to collect data in autumn of 2014 (March–June).
Anthropometric measurementsParticipants wearing light clothing were weighed twice using a digital scale accurate to 100g. Their height was measured twice with the patient barefoot using a wall stadiometer. The means of both measurements were used to calculate the body mass index (BMI) as the weight in kilograms divided by the square of the height in metres (kg/m2). Last of all, the children were classified as having normal weight or overweight/obesity based on the cut-off points established by the International Obesity Task Force.18
Physical activityThe instrument used to measure physical activity was the Spanish version of the Physical Activity Questionnaire for Adolescents (PAQ-A).19 Broadly speaking, the PAQ-A was designed to assess the levels of moderate and vigorous PA in youth. Physical activity was defined as “sports, exercise or dance that make you sweat or get tired, or games that that make you breathe heavily such as playing tag, skipping rope, running, climbing and others”. Participants were asked to quantify their levels of PA activity during their free time in the past seven days. The total PA score was obtained by averaging the nine items rated on a 5-point Likert scale (1–5; with higher scores corresponding to higher levels of PA).
Screen timeSelf-reported ST was measured by means of three questions that asked about the number of hours of free time a day spent watching television, playing computer or video games, and using the computer for anything other than games (emailing, chatting online, web browsing or homework). These questions were used in the Health Behaviour in School-Aged Children study.20 Lastly, the average daily ST was calculated using the sum of these three questions. Thus, ST was categorised as low-moderate if it was below two hours a day, and as high if it amounted to two or more hours a day, following the recommendations on the subject of the American Academy of Paediatrics.21
Sleep habits and problemsThe questionnaire used to assess sleep habits and problems was the Spanish version of the Sleep Self-Report (SSR).17 Each item is rated on a 3-point scale to indicate the frequency of each habit: usually (2=5–7 times a week), sometimes (1=2–4 times a week) and rarely (0=never or once a week). The questionnaire comprises 19 items (three of them gather additional information but are not scored in any subscale) grouped into four subscales: (a) sleep quality; (b) sleep anxiety; (c) bedtime resistance; and (d) sleep routines. The total score is calculated by adding the scores of the 16 items (total score variable). Higher scores indicate more sleep-related problems. We used the cut-off points to indicate sleep problems applying the criteria established by Orgilés, Owens, Espada, Piqueras, Carballo17: 7 for sleep quality, 6 for sleep-related anxiety, 4 for bedtime resistance, 3 for sleep routines and 16 for the total score.
Socioeconomic statusWe assessed socioeconomic status with a scale adapted from Graffar's method,22 and considering three categories based on the school under study (low, middle and high). These categories have been used recently in studies of Chilean children.23
Statistical analysisWe have expressed continuous variables as means and standard deviations, and categorical variables as frequency distributions. We used the Kolmogorov–Smirnoff test to assess the normality of the distributions. Analysis of variance was used to determine the differences in sleep habits (sleep quality, sleep-related anxiety, bedtime resistance, sleep routines and total score) by PA and ST categories (moderate-low vs high), adjusting for age, BMI, socioeconomic status, having a television set in the room and PA or ST depending on the independent variable included in the model. We calculated the effect size (ES) using the estimated marginal means, and subsequently classified it as small (0.20–0.50), moderate (0.51–0.80) or large (>0.80).24 Last of all, we used logistic regression models (odds ratio [OR] and 95% confidence interval [CI]) to determine the influence of adherence to PA and ST habits (independent variable=adheres to none, one, or both habits) on the probability of having sleep problems (dependent variable), adjusting for age, BMI, socioeconomic status and presence or absence of a television set in the room. We performed the statistical analysis with the SPSS software version 22 (SPSS Inc, Chicago, IL, USA).
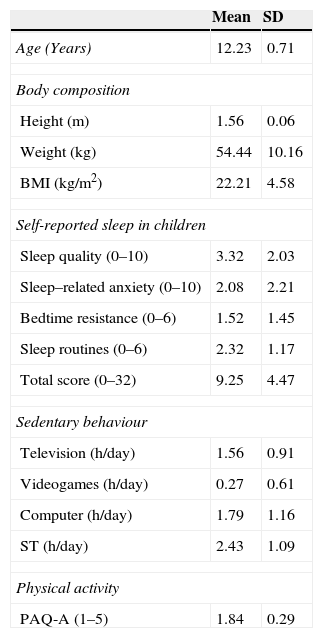
ResultsTable 1 shows the characteristics of the participating girls. Of all participants, 35.53% were classified as having overweight/obesity. The prevalence of sleep problems was 9.20% (total score). As for ST, 63.26% of the girls exceeded the recommended time (≥2h/day). Lastly, when the criteria for both PA (last quartile) and ST were combined, only 11.73% adhered to recommendations for both.
Characteristics of study participants.
| Mean | SD | |
|---|---|---|
| Age (Years) | 12.23 | 0.71 |
| Body composition | ||
| Height (m) | 1.56 | 0.06 |
| Weight (kg) | 54.44 | 10.16 |
| BMI (kg/m2) | 22.21 | 4.58 |
| Self-reported sleep in children | ||
| Sleep quality (0–10) | 3.32 | 2.03 |
| Sleep–related anxiety (0–10) | 2.08 | 2.21 |
| Bedtime resistance (0–6) | 1.52 | 1.45 |
| Sleep routines (0–6) | 2.32 | 1.17 |
| Total score (0–32) | 9.25 | 4.47 |
| Sedentary behaviour | ||
| Television (h/day) | 1.56 | 0.91 |
| Videogames (h/day) | 0.27 | 0.61 |
| Computer (h/day) | 1.79 | 1.16 |
| ST (h/day) | 2.43 | 1.09 |
| Physical activity | ||
| PAQ-A (1–5) | 1.84 | 0.29 |
| n | % | |
|---|---|---|
| Nutritional status | ||
| Overweight/obesity | 70 | 35.53 |
| Sleep problems | ||
| Sleep quality | 19 | 9.69 |
| Sleep-related anxiety | 23 | 11.73 |
| Bedtime resistance | 28 | 14.28 |
| Sleep routines | 57 | 29.08 |
| Total score | 18 | 9.2 |
| Sedentary behaviour | ||
| Television set in room | 107 | 54.59 |
| Exceeds recommended limita | 124 | 63.26 |
| Physical activity | ||
| High levelb | 40 | 20.41 |
| Healthy habits | ||
| PA+ST | 23 | 11.73 |
| Socioeconomic status | ||
| Low | 38 | 19.38 |
| Middle | 124 | 63.26 |
| High | 34 | 17.35 |
BMI, body mass index; PAQ-A, Physical Activity Questionnaire for adolescents20; ST, total screen time—sum of time spent using the television, videogames and computers.
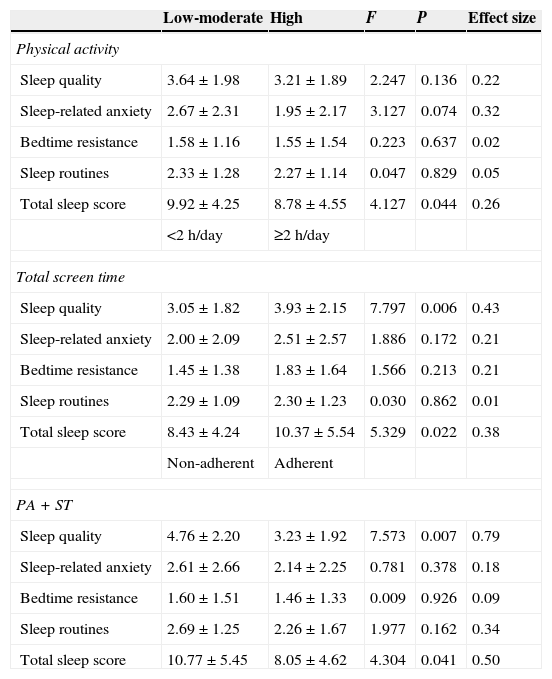
Table 2 shows the differences in the different sleep subscales by PA and ST categories, adjusted for age, BMI, socioeconomic status, having a television in the room and PA or ST depending on the independent variable included in the model. The results showed that less active girls had higher total scores, although the differences were small (9.92 vs 8.78; ES, 0.26). On the other hand, girls that exceeded the recommended ST (≥2h/day) showed a slightly poorer sleep quality (3.05 vs 3.93; ES, 0.43) and total score (8.43 vs 10.37; ES, 0.38). Lastly, analysing PA and ST in combination we found that girls that complied with recommendations for both had a better sleep quality (3.23 vs 4.76; ES, 0.79) and a better total score (10.77 vs 8.05; ES, 0.50), differences that were moderate.
| Low-moderate | High | F | P | Effect size | |
|---|---|---|---|---|---|
| Physical activity | |||||
| Sleep quality | 3.64±1.98 | 3.21±1.89 | 2.247 | 0.136 | 0.22 |
| Sleep-related anxiety | 2.67±2.31 | 1.95±2.17 | 3.127 | 0.074 | 0.32 |
| Bedtime resistance | 1.58±1.16 | 1.55±1.54 | 0.223 | 0.637 | 0.02 |
| Sleep routines | 2.33±1.28 | 2.27±1.14 | 0.047 | 0.829 | 0.05 |
| Total sleep score | 9.92±4.25 | 8.78±4.55 | 4.127 | 0.044 | 0.26 |
| <2h/day | ≥2h/day | ||||
| Total screen time | |||||
| Sleep quality | 3.05±1.82 | 3.93±2.15 | 7.797 | 0.006 | 0.43 |
| Sleep-related anxiety | 2.00±2.09 | 2.51±2.57 | 1.886 | 0.172 | 0.21 |
| Bedtime resistance | 1.45±1.38 | 1.83±1.64 | 1.566 | 0.213 | 0.21 |
| Sleep routines | 2.29±1.09 | 2.30±1.23 | 0.030 | 0.862 | 0.01 |
| Total sleep score | 8.43±4.24 | 10.37±5.54 | 5.329 | 0.022 | 0.38 |
| Non-adherent | Adherent | ||||
| PA+ST | |||||
| Sleep quality | 4.76±2.20 | 3.23±1.92 | 7.573 | 0.007 | 0.79 |
| Sleep-related anxiety | 2.61±2.66 | 2.14±2.25 | 0.781 | 0.378 | 0.18 |
| Bedtime resistance | 1.60±1.51 | 1.46±1.33 | 0.009 | 0.926 | 0.09 |
| Sleep routines | 2.69±1.25 | 2.26±1.67 | 1.977 | 0.162 | 0.34 |
| Total sleep score | 10.77±5.45 | 8.05±4.62 | 4.304 | 0.041 | 0.50 |
Values expressed as mean±SD. PA, physical activity; ST, screen time. Analysis adjusted for age, body mass index, socioeconomic status, television set in the room and physical activity or total screen time depending on the independent variable.
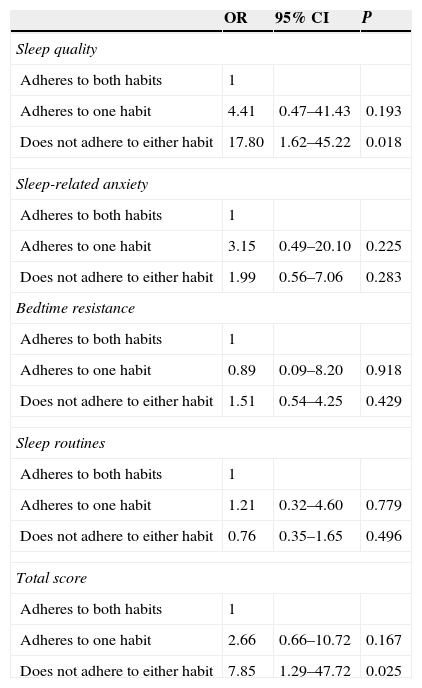
Last of all, the logistic regression model showed that girls that did not adhere to recommendations for either habit (≥1.97 for PA and <2h/day of ST) were more likely to have problems in sleep quality problems (OR, 17.80; P=0.018) or in sleep overall as assessed by the total score (OR, 7.85; P=0.025) (Table 3).
Logistic regression model for predicting sleep problems based on adherence to healthy habits.
| OR | 95% CI | P | |
|---|---|---|---|
| Sleep quality | |||
| Adheres to both habits | 1 | ||
| Adheres to one habit | 4.41 | 0.47–41.43 | 0.193 |
| Does not adhere to either habit | 17.80 | 1.62–45.22 | 0.018 |
| Sleep-related anxiety | |||
| Adheres to both habits | 1 | ||
| Adheres to one habit | 3.15 | 0.49–20.10 | 0.225 |
| Does not adhere to either habit | 1.99 | 0.56–7.06 | 0.283 |
| Bedtime resistance | |||
| Adheres to both habits | 1 | ||
| Adheres to one habit | 0.89 | 0.09–8.20 | 0.918 |
| Does not adhere to either habit | 1.51 | 0.54–4.25 | 0.429 |
| Sleep routines | |||
| Adheres to both habits | 1 | ||
| Adheres to one habit | 1.21 | 0.32–4.60 | 0.779 |
| Does not adhere to either habit | 0.76 | 0.35–1.65 | 0.496 |
| Total score | |||
| Adheres to both habits | 1 | ||
| Adheres to one habit | 2.66 | 0.66–10.72 | 0.167 |
| Does not adhere to either habit | 7.85 | 1.29–47.72 | 0.025 |
Analysis adjusted for age, body mass index, socioeconomic status and television in room.
This study shows that healthy PA and ST habits are associated with better sleep quality. Furthermore, girls that adhere to recommendations for both PA and ST habits seem to have better sleep quality and total sleep scores. Conversely, not adhering to either habit predicted problems in the sleep quality and in total score of participating girls. Compared to their male peers, girls show lower levels of PA (assessed by accelerometry),16 worse sleep habits (assessed by electroencephalography25 or questionnaires17) and similar ST habits (they play fewer videogames but use mobile phones more).26 Thus, it seems that we should study this young population thoroughly and promote healthy habits in it. Our cross-sectional study suggests that girls should be advised to limit or decrease their ST, especially before or during sleep hours in order to minimise its negative impact on sleep and wellbeing, and to promote an active lifestyle.
The assumption that PA promotes better sleep is based on several hypotheses about energy conservation, tissue repair or temperature down-regulation in the individual.27 Recent studies have analysed this association by means of accelerometry. Accelerometers estimate the PA performed by the child over several days (usually one week), and at night they record the actual times the child falls asleep (sleep onset) and wakes up (end of sleep), calculating total sleep duration and night wakings. In this regard, a recent study reported that more active children have poorer sleep quality (more night wakings).11 Its authors noted that higher levels of moderate to vigorous physical activity (MVPA) were associated with more fragmented sleep, although going to bed earlier was associated with less time spent in sedentary behaviour the following day. Conversely, several studies have shown a positive correlation with several sleep-quality parameters. Thus, MVPA has been associated with increased sleep efficiency (percentage of sleep per time in bed)10 and fewer night wakings,5 with some studies assessing sleep by means of electroencephalography.28 It also appears that children that go to bed and get out of bed earlier are more active during the day.9 In our study, the results of the self-administered questionnaire corroborated these findings, showing that girls that were more active achieved better total scores than their less-active peers (ES, 0.26). At the same time, compared to other populations assessed by means of this questionnaire,19,29 the girls in our sample showed a higher level of inactivity, so it would be necessary to establish whether a higher level of PA leads to better sleep10 or the other way around.11
Several studies have demonstrated the negative impact of digital media on the sleep of young individuals, especially on sleep duration30 and delayed bedtimes.31 However, their effects and the specific mechanisms involved remain unclear.7,8 Our study showed that girls with higher STs had poorer sleep quality (for example, waking at night due to some kind of pain) (ES, 0.43) and a worse total score compared to their peers with lesser STs (ES, 0.38). Some of the mechanisms that could explain this fact are greater physiological arousal, which would make it harder for girls to relax before bed, and a suppression of melatonin secretion due to exposure to the bright light of displays, which would promote delays in the circadian rhythm.32 Similarly, higher STs at bedtime could be due to an increase in educational computer use or that this age (13 years) is the minimum required to register in various popular social networks.
When it comes to both habits, we only found one study on the subject that analysed adherence to the recommendations concerning PA (>60min/day of MVPA) and ST (>2h/day) in relation to sleep quality in children.9 These authors noted that going to bed and getting up late are associated with a lesser degree of adherence to PA and ST recommendations, and thus with worse health, regardless of sleep duration. Our study supports these findings, as it suggests that the most important factor associated with poorer sleep quality (ES=0.79) and total score (ES=0.50) is non-adherence with recommendations for both of these habits. Furthermore, non-adherence seems to predict sleep quality problems and sleep problems in general (total score). This fact may be due to girls devoting more time to digital media and consequently reducing the time spent sleeping or in other activities related to good sleep hygiene (for example, PA). Thus, we would expect a perception of decreased sleep and poorer sleep quality.17
LimitationsThere are limitations to the study that ought to be considered: (a) it is a cross-sectional study, and thus the results cannot be used to establish causality; (b) self-reported data may be biased and do not provide the direct measurements of sleep that can otherwise be obtained by electroencephalography or accelerometry; (c) the answers to the sleep questionnaire are based on the past week, which may make detection of sleep problems difficult, as it requires a longer assessment period,17 and the questionnaire does not differentiate between weekdays and weekends; (d) the data obtained on the levels of PA and ST (sedentary habits) cannot provide a precise representation of the variables under study; and last of all (e) we did not take into account the pubertal development of the girls, an aspect that could influence their anthropometric measurements and possibly their sleep quality.33
ConclusionsThe findings of this study point to the need to analyse the impact of PA and ST habits in combination for the prevention of sleep-related disorders and associated health parameters, including obesity. However, the discrepancies found between questionnaires and objective measures suggest that further research is needed that uses objective measurements (accelerometry) to establish conclusive results on the matter, as well as randomised controlled interventions that promote both habits.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Aguilar MM, Vergara FA, Velásquez EJA, García-Hermoso A. Actividad física, tiempo de pantalla y patrones de sueño en niñas chilenas. An Pediatr (Barc). 2015;83:304–310.
