



Spontaneous retropharyngeal emphysema (SRE) is characterised by the presence of ectopic air at the retropharyngeal level without a clear underlying aetiology. It is a diagnosis of exclusion and considered very infrequent, with few isolated cases reported in the scientific literature. To date, cases in the paediatric population have been exceptional.1–5
We present the case of a boy aged 8 years with an unremarkable medical history assessed in the emergency department for chest pain radiating to the neck with sudden onset while playing football. The patient reported worsening pain when lying down or eating. He reported no recent trauma or foreign body ingestion. The physical examination revealed that the patient was in good health with haemodynamic and respiratory stability. The patient had no fever at any point. There was no evidence of bone abnormalities, although subcutaneous crepitus was detected in the cervical region. The tonsillar pillars were not swollen and the uvula was not deviated. Blood tests showed leucocytosis and neutrophilia without elevation of acute phase reactants. A lateral cervical radiograph was taken, revealing the presence of air in the retropharyngeal space, without an increase in the size of the space (Fig. 1, left). The nasolaryngoscopic exam was normal. A barium swallow was not performed. The patient was hospitalised for 24 hours, receiving intravenous analgesia and fluids, but not supplemental oxygen, and his symptoms resolved. A radiograph performed on an outpatient basis 15 days later evinced near-full resolution of the abnormalities (Fig. 1, right).
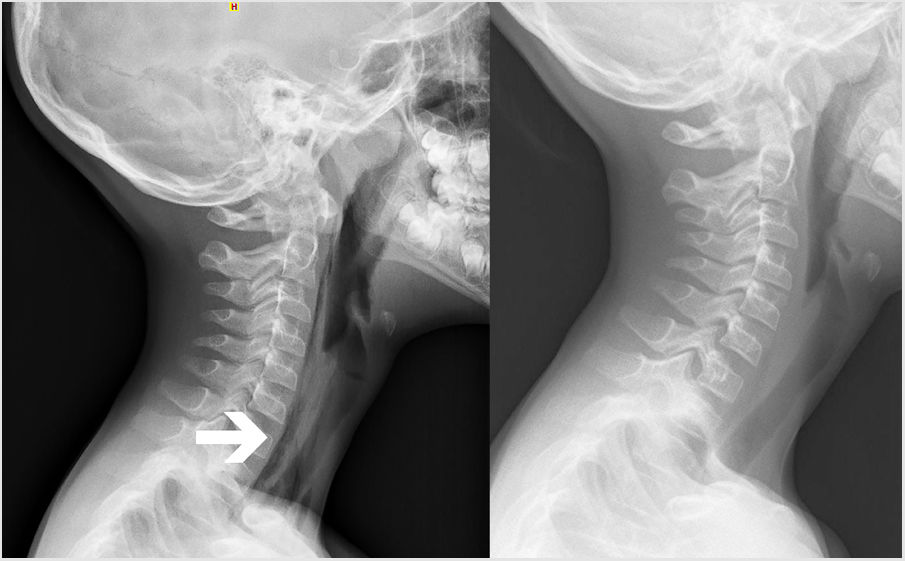
Table 1 details the cases of paediatric SRE published to date. It can be seen that the majority occurred in female adolescents and that in many cases there was an identifiable trigger (cough or sports). Two of the patients experienced voice changes. Most had onset with sudden chest or neck pain. The presence of fever or low-grade fever was documented in 3 cases, and leucocytosis and neutrophilia in 1. The nasolaryngoscopic exam only revealed a slight protrusion of the posterior pharyngeal wall in 1 patient, and was normal in all others. Three patients underwent a CT scan. All cases were managed conservatively and had a favourable outcome.
Cases of spontaneous retropharyngeal emphysema reported in the paediatric population and its clinical characteristics.
| Autor(es) | Relevant history | Sociodemographic characteristics | Trigger | Clinical presentation | Clinical or laboratory abnormalities | NLC | CT | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Marín Garrido et al. (2003)4 | None | Male. 13 years | Sports | Sudden chest and neck pain. Voice changes | Low-grade fever (37.5 °C). BT not reported | Mild protrusion of posterior pharyngeal wall | Yes | Rest. Intravenous antibiotherapy | Favourable (radiological resolution in 48 hours) |
| Lee et al. (2005)5 | Asthma | Female. 12 years | None | Respiratory distress. Chest pain. Voice changes | Desaturation, tachypnoea, fever (38.2 °C) | Normal | No | Rest. Oxygen. Antibiotics. Bronchodilators | Favourable (resolution of symptoms in 7 days) |
| Haro et al. (2014)2 | None | Female. 14 years | Coughs | Sudden cervical pain | Fever (39 °C). Normal BT | Normal | No | Rest. Analgesia. Supplemental oxygen | Favourable |
| Cho et al. (2016)3 | None | Female. 14 years | Coughs | Odynophagia | Afebrile. BT not reported | Normal | Yes | Rest. Nil per os. Supplemental oxygen. Intravenous antibiotherapy | Favourable (3 day hospitalization) |
| Chi et al. (2018)1 | None | Female. 13 years | None | Cervical pain | Afebrile. Leucocytosis. Neutrophilia | Normal | Yes | Analgesia. Monitoring. Nil per os | Favourable (resolution of symptoms in 7 days) |
| Arredondo Montero et al. (2022) | None | Male. 8 years | Sports | Sudden cervical pain | Afebrile. Leucocytosis. Neutrophilia | Normal | No | Analgesia. Monitoring. Nil per os | Favourable (24 hours hospitalization, radiological resolution in 15 days) |
BT, blood test; CT, computed tomography; NLC, nasolaryngoscopy.
In the case reported by Lee et al.,5 a female patient with asthma, the presentation was atypical, with increased work of breathing, desaturation and pneumomediastinum. We suppose that this patient probably presented with pneumomediastinum secondary to asthma that eventually extended to the cervical region, and therefore we do not consider this a true case of SRE.
The literature on the aetiology, pathogenesis and pathophysiology of SRE is scarce. Macklin et al.6 published an article in which they proposed that the aetiology could involve the formation of pulmonary interstitial emphysema secondary to an overdistension of marginal alveoli and decrease in calibre of perialveolar vessels, generating a pressure gradient between both structures that would cause alveolar rupture at the basal level and leaking of air into the interstitial space. The air would spread along the path of least resistance through the perivascular sheaths, chiefly to the mediastinum (as seen in the cases described by Cho et al.3 and Lee et al.5) and potentially reaching the cervical region.
As regards the overdistension of marginal alveoli, the coughing physical activity described in the cases included in the series could have contributed to triggering this pathophysiological mechanism. Similarly, this mechanism could be involved in the case of pneumomediastinum associated with asthma described by Lee et al.5
In conclusion, SRE seems to be a distinct albeit infrequent entity predominantly found in female adolescents. Its management includes nil per os, intravenous fluids, analgesia and rest, and supplemental oxygen may be an additional option. Although it is a benign disease, it is imperative to remember that it is a diagnosis of exclusion and that all potential causes of ectopic air in the retropharyngeal space need to be ruled out, especially those that require urgent treatment, such as oesophageal perforation. Surgical intervention should be considered in the event of complications like mediastinitis or airway obstruction.
