





We present the case of a male neonate born preterm at 34 weeks with gastroschisis that could not tolerate the primary closure of the bowel that had bulged out during birth. Compared to the use of a silo1 to delay the reduction of the prolapsed organs, we describe the use of the Alexis® wound retractor, which consists of 2 flexible rings joined by a flexible polymer sleeve that fits and seals the inner surface of the abdominal wall and keeps the bowel protected without requiring suturing or any form of surgery for its fixation (Fig. 1).

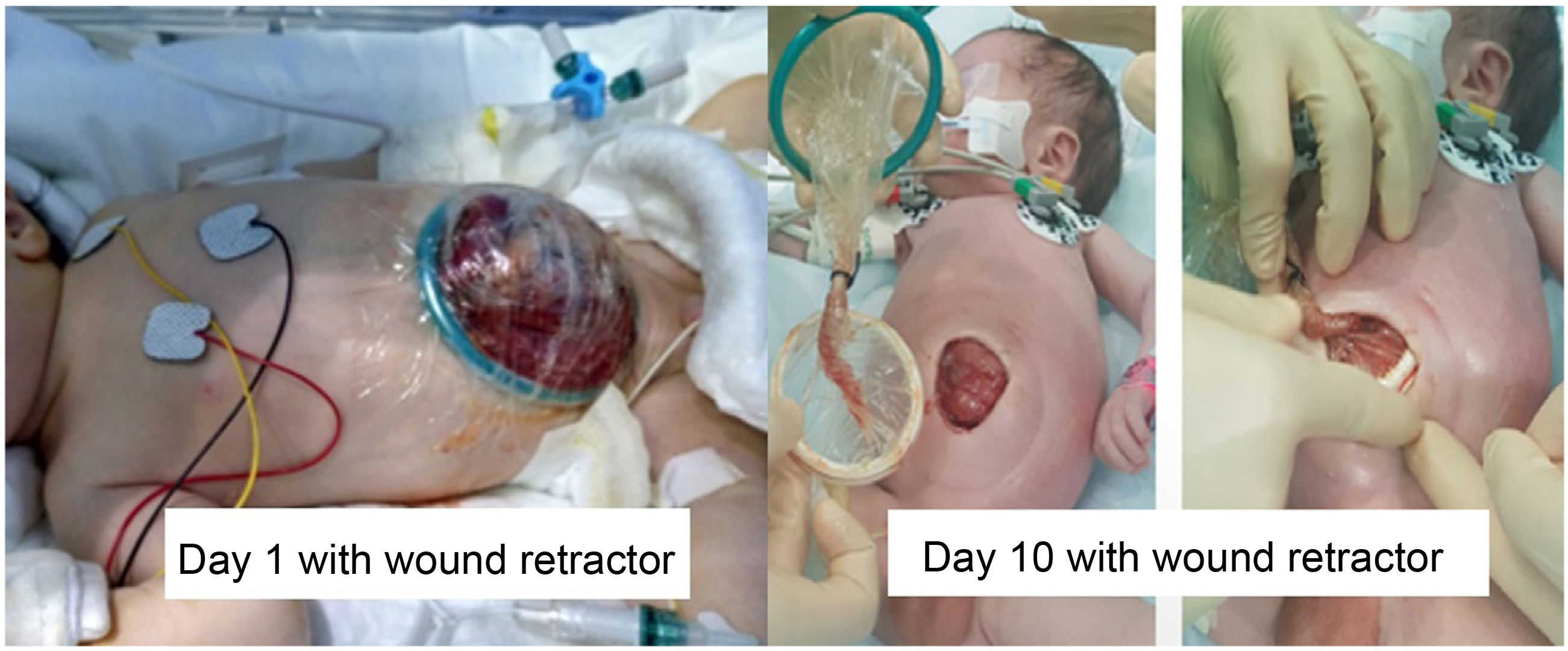
In the first day of life, after ruling out the presence of associated malformations, the device was placed in the operating room, using size S (2.5–6cm), because the patient could not tolerate the complete reduction of the prolapsed viscera. Later, staged closure was achieved in the intensive care unit with progressive reduction of the bowel day by day and delayed surgery for complete closure on day 10 post birth (Fig. 2).
Thus, we conclude that the use of the wound retractor allows delaying the closure of the abdominal wall defect following the progressive reduction of the bowel in patients who could not tolerate primary closure. This method is less invasive than the traditional silo, and offers further advantages, as it requires less handling, medication and ventilatory support, which translates to a decrease in morbidity and easier management2,3 (Fig. 3).

