



A girl aged 12 years presented to a hospital emergency department with a possible dislocation of the left wrist that would have taken place 3 days prior when the patient was playing and doing acrobatics. From that time, she experienced discomfort moving the wrist.
The examination of the left wrist evinced a prominent ulnar head compared to the contralateral wrist. Bilateral hyperlaxity, full range of flexion and extension, painless pronation against resistance and mild discomfort on forced supination.
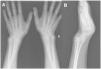
The wrist radiograph (Fig. 1) showed what seemed like a deviation of the distal epiphysis of the radius and a V-shaped carpus, with no differences between the two wrists. A watchful waiting approach was taken, with provision of conservative treatment with an elastic brace and analgesics and follow-up in the outpatient trauma clinic once Madelung deformity was confirmed with a CT scan (Fig. 2).

Madelung deformity is a rare congenital anomaly of the wrist involving a radial deformity with inclination of the radial physis toward the ulnar physis due to an abnormal Vikers ligament or asymmetric growth at the physis. It is more frequent in de girls with bilateral involvement and onset between ages 8 and 12 years.1 The diagnosis is made by means of plain radiography, which allows visualization of an increased distal radius volar tilt, subluxation of the ulnar head and a V-shaped carpus,2 although computed tomography or magnetic resonance imaging can be used to obtain higher-resolution images. The treatment depends on the level of pain and functional impairment, and conservative treatment with wrist splinting is usually sufficient.1
