






The aim of this study is to evaluate the effectiveness of a disaster preparedness training programme in a Paediatric Emergency Department (PED).
MethodsA quasi-experimental study was conducted using an anonymous questionnaire that was distributed to health care providers of a PED in a tertiary paediatric hospital. The questions concerned the disaster plan (DP), including theoretical and practical aspects. Questionnaires were distributed and completed in January 2014 (period 1) and November 2014 (period 2). The disaster training programme includes theoretical and practical sessions.
ResultsA total of 110 questionnaires were collected in period 1, and 80 in period 2. Almost three-quarters (71.3%) of PED staff attended the theoretical sessions, and 43.8% attended the practical sessions. The application of this training programme significantly improved knowledge about the DP, but no improvement was observed in the practical questions. PED staff felt more prepared to face a disaster after the training programme (15.5% vs. 41.8%, P<.001).
ConclusionsThe training programme improved some knowledge about the disaster plan, but it has not improved responses in practical situations, which may be due to the low attendance at practical sessions and the time between the training programme and the questionnaires.
Analizar la eficacia de un programa formativo sobre catástrofes en un Servicio de Urgencias Pediátricas (SUP).
MetodologíaEstudio cuasiexperimental mediante encuestas dirigidas al personal sanitario del SUP de un hospital pediátrico de tercer nivel. Se evalúan aspectos teóricos y prácticos del plan de catástrofes (PC). Las encuestas son cumplimentadas en 2 periodos (periodo 1, enero del 2014, y periodo 2, noviembre del 2014), entre los cuales se realiza una formación con sesiones teóricas y situaciones clínicas.
ResultadosSe recogen 110 encuestas en el periodo 1 y 80 en el periodo 2. El 71,3% del personal asiste a las sesiones teóricas y el 43,8% a las prácticas. Tras la formación, aumenta significativamente la proporción del personal que conoce el PC y el «kit» de catástrofes. En cuanto a los aspectos prácticos, no se observa mejoría en las respuestas a las situaciones clínicas planteadas. El personal se siente más preparado para afrontar una catástrofe después del programa formativo (15,5% vs. 41,8%, p<0,001).
ConclusionesLa aplicación de una formación sobre catástrofes ha mejorado algunos conocimientos del personal, pero no ha mejorado las respuestas en las situaciones clínicas planteadas, posiblemente influenciado por la baja asistencia a las sesiones prácticas y el tiempo transcurrido entre la formación y la encuesta.
A disaster is any situation or event that overwhelms local response resources, and usually produces severe damage, destruction and human suffering.1–3 The impact of disasters is particularly severe in the field of paediatric emergency medicine, as children are more vulnerable and at greater risk of experiencing dehydration, infection and multiple trauma.1,4
Therefore, it is essential that paediatric emergency departments (PEDs) and their personnel be properly prepared to manage these situations, which, while infrequent, can result in substantial morbidity and mortality in the population. Such preparedness involves a broad range of elements: availability of materials, reorganisation of health care delivery, training of health care staff…
Training in disaster preparedness is a must for all health care workers, especially for those in emergency settings, and should be incorporated in educational curricula, as has been recommended by the American Medical College.2,4 A lack of specific training in disaster preparedness poses risks to the health of the general population and also to that of patient care providers.5 There are different educational strategies and a wide variety of training programmes, ranging from the Advanced Pediatric Life Support (APLS) to self-directed courses, day-long workshops or training sessions that use simulation.3,4,6,7.
Several studies, most of them conducted outside of Spain, warn of a lack of disaster preparedness.4,6,8,9 In Spain, many PEDs do have disaster plans in place, but they are usually not up to date and are not generally known by the staff.10
The aim of this study was to analyse the efficacy of a disaster preparedness training programme in a PED.
MethodsWe conducted a quasi-experimental pre-post intervention study by means of a survey of health care workers in which the training programme was the intervention. The study took place in a tertiary paediatric hospital that receives approximately 100,000 visits a year and is the reference hospital for patients with multiple trauma. The hospital has a disaster plan (DP) that was updated in 2013 and the PED is equipped with a disaster kit to be opened by the staff in case the DP is activated.
The target population of our study was the collective of health care workers that regularly staffs the PED (125 individuals), including nursing staff (nurse assistants and registered nurses [RNs]) and doctors in the specialties of paediatric emergency medicine, surgery and traumatology (adjunct, fellow and resident doctors).
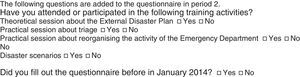
We conducted the study over two time periods (period 1, before training, in January 2014, and period 2, after training, in November 2014) and the training programme took place between the two (April 2014). Between the two periods, the researchers asked the health care staff to fill out the paper-based questionnaire anonymously, and no reward was offered for participating.
The training programme consisted of one theoretical session that explained the hospital's DP and two three-hour-long practical sessions in which various disaster-related clinical scenarios were discussed in small groups to put the DP into practice (victim triage, reorganisation of PED activity and space, duties of the shift manager).
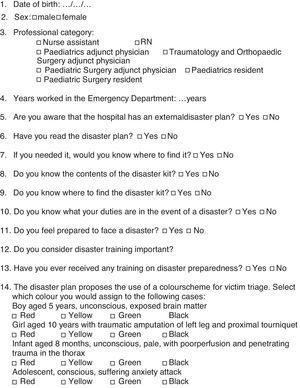
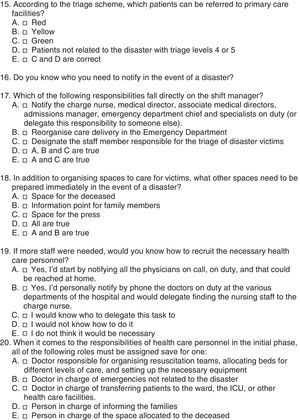
The questionnaire was written in Spanish and based on the published literature,11 and comprised 20 multiple-answer questions (Appendix 1). It included:
- –
Demographic data of the health care worker (sex, age, professional category, years worked in the emergency department).
- –
Five theoretical questions about the external disaster plan, the disaster kit, and the duties of the shift manager.
- –
Ten practical questions that presented clinical situations in disaster scenarios requiring the application of the DP and that assessed aspects such as victim triage, the reorganisation of space in the PED, staff duties and recruitment.
- –
Two personal questions that asked about the perceived importance of the training and whether the respondent felt prepared to respond to a disaster.
To score the answers for the ten practical questions, each correct answer was graded with one point and each incorrect answer with zero points, which were added up to obtain the total score for practical knowledge (minimum score, 0; maximum score, 10).
ResultsWe collected 110 questionnaires in period 1 (88% response rate) and 80 in period 2 (64% response rate). Table 1 shows the demographic data of the respondents.
Demographic data of study participants.
| Period 1 Pre training | Period 2 Post training | P | |
|---|---|---|---|
| Female sex | 96 (87.3%) | 67 (85.8%) | NS |
| Age | Median 33 years (IQR, 28–42) | Median 34 years (IQR, 28–43) | NS |
| Years worked in Emergency dept | Median 4 years (IQR, 2–10) | Median 7 years (IQR, 3–13) | NS |
| Professional category | |||
| Adjunct physician | 23 (21.3%) | 21 (26.3%) | NS |
| Resident physician | 34 (31.5%) | 21 (26.3%) | NS |
| Registered nurse | 34 (31.5%) | 23 (28.7%) | NS |
| Nurse assistant | 17 (15.7%) | 15 (18.7%) | NS |
IQR, interquartile range; NS, not significant.
Sixty percent of the staff that filled out the questionnaire in period 1 had never undergone disaster training of any kind. Eighty percent of respondents in period 2 had completed the questionnaire in period 1. Of all period 2 respondents, 71.3% had attended the theoretical session and 43.8% had participated in the practical sessions. Thirty percent of respondents in period 2 had completed the full training.
Following the training programme, we observed significant differences in the awareness of the existence of a DP (77.1% vs. 95%, P=.001), having read the DP (24.5% vs. 67.5%; P<.001), and knowing where to find the DP (52.77% vs. 73.8%; P=.003).
Concerning the disaster kit, we also observed a significant increase in the number of staff that were aware of its existence (53.6% vs. 72.5%; P=.008) and that knew where to find it in the PED (33.6% vs. 72.7%; P<.001) after the training.
When it came to the responsibilities of the shift manager, 33.6% of the health care workers knew them in period 1, compared to 72.7% in period 2 (P<.001).
We did not observe a significant improvement in the mean score obtained in the practical questions from period 1 to period 2 (5.8/10 vs. 6.1/10). We also did not find a statistically significant difference between the answers given in each period for any of the 10 practical questions when we analysed each of them separately.
The staff felt better prepared to face a disaster after participating in the training programme (15.5% vs. 41.8%; P<.001) and 98.8% stated that training on this subject is important.
DiscussionBased on the results of the study, the training programme succeeded in improving certain knowledge areas in the staff, mostly concerning theoretical aspects of the DP. However, the application of this theoretical knowledge to the proposed clinical scenarios did not improve, so the results we obtained were not entirely satisfactory.
This may be due to various factors. On the one hand, the time elapsed between training and the survey was six months, so participants may have forgotten some of what they had learned; on the other hand, less than half of the staff attended the practical sessions and those that did not were unable to put the DP into practice; last of all, the training programme did not include simulation exercises, such as drills in the PED or virtual simulations.
Although the studies published to date have yet to identify the most effective training strategy, most disaster readiness courses recommend the performance of practical sessions with drills.7,9,12 Such drills should be performed on a regular basis, as on one hand they consolidate the knowledge of the staff, and on the other help identify areas for improvement in the DP of the facility.3,7,9
The health care workers in our sample stated that training in disaster preparedness is important, which was consistent with the findings of other authors.4,6,9 Health care staff usually have limited experience in disasters due to the low frequency of such occurrences, and usually want a combination of didactic and experiential training that includes simulations or drills.4,9 In fact, the recommended coursework in paediatric disaster medicine in the United States comprises five components and includes experiential learning: preparedness, knowledge of the response system, triage, treatment, mental health needs of victims and local training.2,3
In addition to the limitations inherent in any survey-based study, our assessment of the outcomes of the training programme may be biased for lack of a control group consisting of individuals with no training. We also were unable to compare the performance of the staff that participated in the training programme with that of staff that did not participate, as the surveys were filled out anonymously. Furthermore, the survey has not been validated, so its results must be interpreted with caution. Last of all, the high dropout rate between the two periods may be a significant source of bias, as the interest in disaster training of respondents in period 2 is probably greater.
To conclude, the implementation of a specific training programme on disaster preparedness improved some of the knowledge of health care workers, but was not associated with an improvement in answers given to hypothetical clinical situations they were presented with. Therefore, training needs to be improved, incorporating simulations or drills, and giving incentives for staff participation.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Parra Cotanda C, Rebordosa Martínez M, Trenchs Sainz de la Maza V, Luaces Cubells C. Impacto de un programa de formación de catástrofes en el personal sanitario. An Pediatr (Barc). 2016;85:149–154.
Previous presentations: This study was presented as an oral communication at the XX Reunión Anual de la Sociedad Española de Urgencias de Pediatría; April 16–18, 2015; Bilbao, Spain. It has not been published before and it is not under consideration by any other editorial board.

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals