



Transverse myelitis (TM) is a focal inflammation of the entire thickness of the spinal cord.1 Its incidence rate is 1–8/1000000inhabitants/year.2 It is typically present in patients aged 0–2 and 5–7 years with symmetric pain, progressive weakness, sensory disturbances, and bowel or bladder dysfunction.2,3
It is caused by an altered immune response and viral infection of the spinal cord that extends to the nerve fibres, leading to hypoxaemia, ischaemia, inflammation, and demyelinisation.2
The differential diagnosis must rule out a compressive myelopathy by means of magnetic resonance imaging (MRI). After ruling out a compressive aetiology, a lumbar puncture is indicated to assess for noninflammatory causes in the absence of leukocytosis.2
A full recovery occurs in one-third of the patients, usually spontaneously, and factors for a poor prognosis include older age, acute onset, a protracted course, presence of supraspinal symptoms, severe denervation, normal cerebrospinal fluid, and delayed onset of recovery.3
This paper presents a singular case of delayed-onset post-chickenpox TM, as well as an update on the few existing publications on the subject.
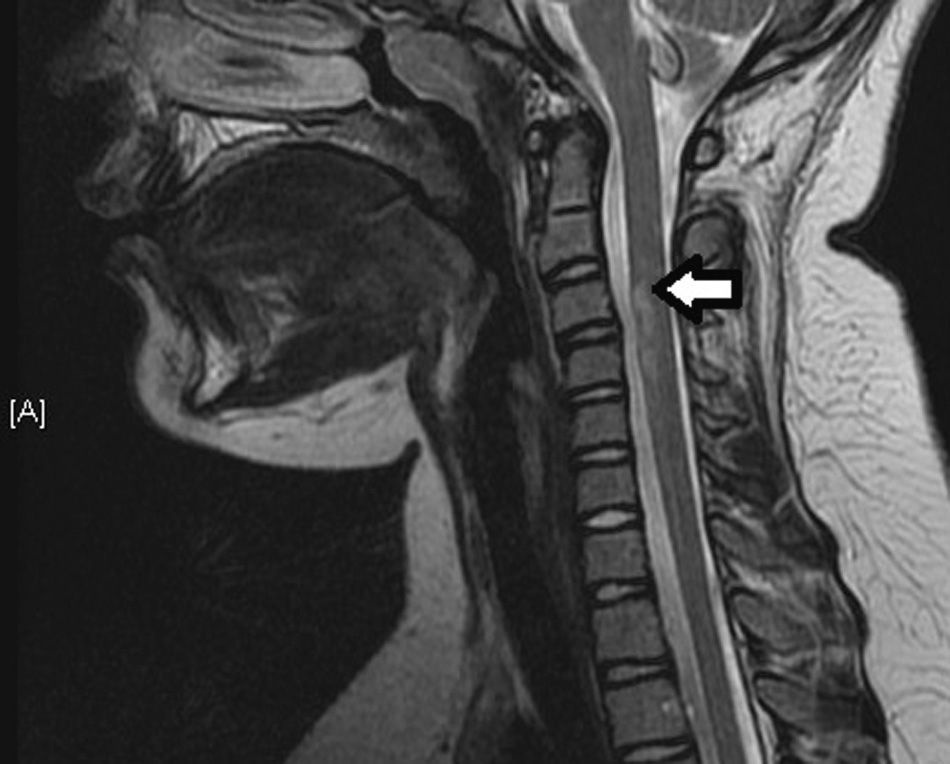
The patient was a 10-year-old girl presenting with a fever of 39°C, paresthesias, pain in the right shoulder, cervicalgia, and loss of power and weakness in the upper limbs (ULs) lasting 24h. The examination found proximal weakness of the pectoral girdle, with the left side (1/5) weaker than the right (2/5), preserved distal strength (4/5), and urinary retention requiring catheterisation for bladder drainage. Blood and urine cultures, serology tests, immunology testing, and the cytochemical study and oligoclonal bands of the CSF were all negative, except for positive tests for IgM and IgG antibodies to VZV. The latter was evidence of a previous latent infection, and the mother reported that the patient had had chickenpox a month and a half earlier, while PCR did not detect VZV in the CSF. A T2-weighted MRI scan without contrast ruled out a brain abnormality and revealed a thickening of the spinal cord and a hyperechoic fusiform lesion in the anterior and peripheral portion of the cord between C3 and C4, findings compatible with a varicella aetiology (Fig. 1).
The patient was treated with bolus steroids (1g/day/5 days) and immunoglobulins (2g/kg/day/4 days), with progressive recovery of strength in the ULs (right, 4/5; left 2/5). After discharge, at home the patient completed pharmacological treatment by tapering off steroids and started rehabilitation sessions, progressing favourably.
Transverse myelitis presents with abrupt onset of progressive weakness and sensory disturbance, usually in the lower limbs,2,4 contrary to what happened in our case, with weakness in the ULs. Another atypical feature in our patient was the presence of fever. A recent history of vaccination or infection is frequent in children, although VZV is not a common cause of TM in immunocompetent children (0.01–0.3%).1
The diagnosis of post-chickenpox myelitis is made by means of serological tests, CSF analysis with VZV PCR, and MRI, which typically shows inflammation of the spinal cord with fusiform-like hyperintensities on T2-weighted images with heterogeneous enhancement, and involvement of several vertebral levels, as observed in our patient.2,5
We based our diagnosis on the recent history of infection by VZV and the compatible clinical features and serology and MRI findings.
As for the interval between the onset of TM and chickenpox, the literature describes that they occur simultaneously or that TM manifests 1–2 weeks after the appearance of the papulomacular rash,1 while our patient developed TM 6 weeks later, probably due to a delayed-type hypersensitivity cell-mediated immune response.
There is no established treatment regime for post-chickenpox TM, but the literature shows that patients evolve favourably with acyclovir and steroids.1,4,5 Acyclovir was not used in our patient because the previous infectious history was unknown, as the mother had not reported it during the anamnesis. Physical therapy following the acute episode can diminish neurologic deficits in these patients.2 Thus, early initiation of these therapies is important in reducing sequelae. Recovery usually starts after 10 weeks, and can take as long as 12–24 months.1,4
It is worth noting that a history of vaccination against varicella was absent, so we must underscore the need to vaccinate against this virus in order to reduce the incidence of chickenpox and its complications.6
In conclusion, post-chickenpox TM is an uncommon complication in immunocompetent children and must be considered in the differential diagnosis of patients with a history of varicella infection in the six weeks preceding the onset of symptoms. Magnetic resonance imaging of the spinal cord and serological tests and PCR for VZV are useful tools for diagnosing this disease. Pharmacological treatment and rehabilitation therapy must be initiated as soon as possible to reduce the sequelae.
Please cite this article as: Ariza Jiménez AB, Martínez Antón J, Urda Cardona A. Mielitis transversa focal posvaricelosa tardía: a propósito de un caso. Revisión y puesta al día. An Pediatr (Barc). 2015;82:41–42.
