



Medulloblastoma accounts for 20% of all paediatric brain tumours as the second most frequent type. It arises from the embryonic neuroectodermal cells of the cerebellum, and it is characterized by decreased speech, mutism, cerebellar dysfunctions, and apathy.1 Children with medulloblastoma can experience a broad range of functional problems due to the effects of the primary tumour and complications of treatment. There is a dearth of evidence on balance rehabilitation in children with medulloblastoma. Ospina et al. found no trials comparing the effects of physical therapy interventions focused on symptom relief and compensation of adverse effects of treatment in children and adolescents with cancer. Thus, there are no standardised rehabilitation exercise programmes for children with brain tumours.2 At present, approaches to rehabilitation are frequently attempted in children with brain tumours. The assessment of physical activity and performance in functional skills and activities daily living of children is useful in clinical practice. The correct implementation of rehabilitation therapy requires accurate and reliable evaluation. This paper focuses on the effect of the Nintendo Wii Fit Plus® (NWFP), which we have and use in our clinic as an intervention to improve balance in children with medulloblastoma.
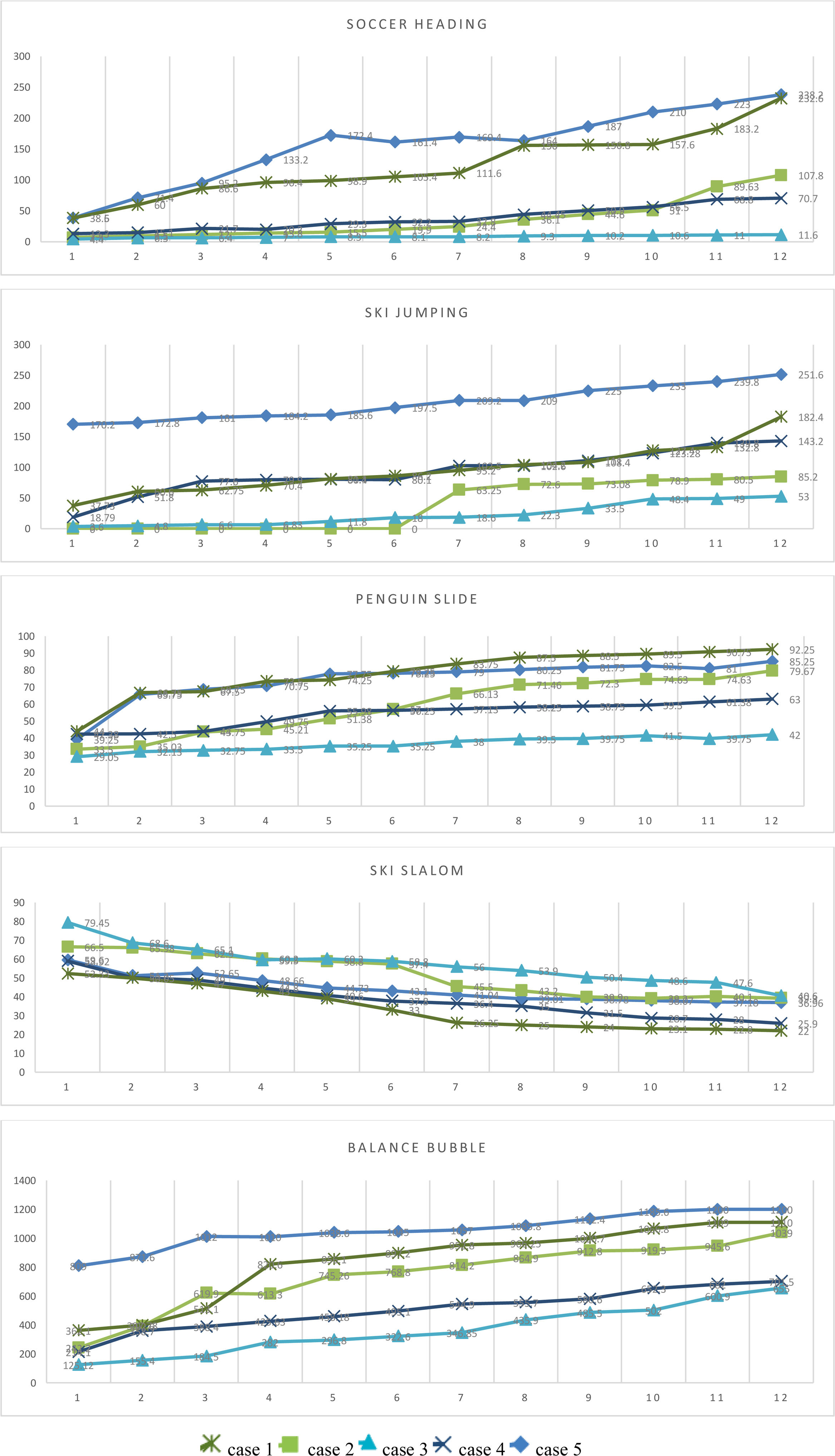
Case seriesThe study was approved by the ethics committee of the local university ethics committee. We obtained the signed informed consent and assent for participation from children and their parents. The evaluations and intervention were supervised by the same physical therapist in a sample of children with medulloblastoma treated with the same protocol and followed up in the department of paediatric haematology and oncology of our university hospital. We excluded children currently in treatment, treated with cranial irradiation, in relapse or with any impairment that could pose a barrier to performing the exercises. Table 1 summarises the demographic and clinical characteristics of the participants. Children were assessed with the body test included in the NWFP. The body test evaluated (1) centre of gravity (CoG), and (2) Fit Age. The CoG reflects the percentage of the weight placed on the right and left sides of the body to assess balance. We recorded the differences between the left and right sides of the body. In healthy subjects, the difference is zero (0%), with equal distribution in both sides. The Fit Age is a number obtained through the board of the NWFP balance test system. The fit age should be the same age as the chronological age. The difference between these ages shows a deviation from the normal range. Five children with medulloblastoma completed the intervention. Children participated in the NWFP intervention for 12 weeks, in 45-min sessions 2 days a week. The intervention included 5 different balance games under the supervision of an experienced physical therapist (Table 2). We made measurements before, during and after the intervention. The sample exhibited significant progressive improvement in game scores in each session (first week mean vs last week mean: soccer heading, 20.42 vs 132.18; ski jumping, 46.064 vs 143.08; penguin slide, 37.636 vs 72.434; ski slalom, 63.36 vs 32.952; balance bubble, 350.504 vs 941.1). Fig. 1 presents the mean weekly score for each game obtained by each participant.
Demographic and clinical characteristics of the patients.
| Sex | BMI | Age | Age at diagnosis | CTx | RTx | PT | Fit Age | CoG right-left Δ (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | After | Δ | Before | After | Δ | ||||||||
| Case 1 | Male | 21.33 | 14 | 12 | 8 | 35 | 12 | 25 | 24 | 1 | 7.6 | 3.4 | 4.2% |
| Case 2 | Female | 19.6 | 7 | 4 | 8 | 46 | 24 | 55 | 26 | 29 | 15.6 | 0.4 | 15.2% |
| Case 3 | Female | 31.55 | 14 | 11 | 8 | 35 | 24 | 50 | 36 | 14 | 47.2 | 0.9 | 46.1% |
| Case 4 | Male | 16.45 | 7 | 4 | 8 | 30 | 24 | 31 | 21 | 10 | 7.6 | 2 | 5.6% |
| Case 5 | Female | 16.16 | 10 | 9 | 8 | 35 | 16 | 30 | 22 | 8 | 12.6 | 2.2 | 10.4% |
BMI, body mass index; CoG, centre of gravity; CTx, chemotherapy; PT, physical therapy; RTx, radiotherapy.
Details of the games.
| Soccer heading | Ski jumping | Penguin slide | Ski slalom | Balance bubble | |
|---|---|---|---|---|---|
| General Description | Tilting the body towards the appropriate object to collect points | Standing up from the squatting position to jump forward | Shifting weight to collect items from the left and right to get points | Finishing the game making the least mistakes as fast as possible | Moving forward in the balloon without hitting the objects on the edges |
| Therapeutic Goals | Body control, transfer of weight to the right and left and proprioception, enhancing visual perception | Protection of squat position, standing and balance with lower extremity force transmission | Body control to improve transfer of weight to the right and left | Body control, transfer of weight to the right and left, maintaining hip-knee-ankle control | Improving body control, visual feedback, attention and coordination |
| Repetition | 5 times | 5 times | 4 times | 5 times | Once |
| Duration | 1 min per game | 1 min per game, each game has 2 jumps | 1.5 min per game | 1 min per game | Depends on the child |
| Scoring | High scores indicate better performance | High scores indicate better performance | High scores indicate better performance | Lower scores indicate better performance | High scores indicate better performance, and the maximum score is 1200. |
This work presents the effect of the NWFP intervention for management of balance impairment in children with medulloblastoma. Based on the findings in this case series, the NWFP intervention is beneficial for rehabilitation of balance impairment. The body test (CoG and Fit Age) and game scores in the NWFP system improved after the intervention in children with medulloblastoma. Thus, our analysis of the NWFP intervention in these children, with physical, physiological and cognitive improvements, reflects that the body can adapt to physical activities. The mean improvement after the intervention in children with medulloblastoma was 16.3% in the CoG and 12.4 years in the Fit Age. These improvements in balance and functional mobility, which would apply to activities of daily living, is important given that balance impairment has a significant impact in the performance of other activities that are part of everyday life, such as walking. Although this intervention does not focus primarily on training for activities like walking or running, these games train the body to improve balance and coordination, which support walking or running.
Children with medulloblastoma require rehabilitation to reduce symptoms, improve function and perform activities of daily living. Rehabilitation has a role not only in symptom management but also to continue to participate in daily activities. For example, increasing scores along with motor learning facilitates engaging in activities of daily living. Since the integration of games into functional activities is important, the treatment program should be planned considering the International Classification of Functioning, Disability and Health. Based on it, different rehabilitation approaches are necessary for children with brain tumours.3 Cognitive and affective barriers associated with medulloblastoma can negatively impact motivation and adherence to the intervention, and therefore can have an impact on the success of rehabilitation.4,5 We encouraged participation in virtual reality-based exercises for 12 weeks and reported verbally (mean 8.5/10) by children and their families. The adherence to the NWFP intervention was 83.3%. Customisation of virtual rehabilitation tools seems to have a positive impact on the motivation and effort of both paediatric and adult users.6
The NWFP intervention may be an effective home-based rehabilitation strategy, and is worth exploring in a larger trial. This intervention may be useful for providing balance training to children with medulloblastoma.
FundingWe did not receive any fees from Nintendo for the study or the Nintendo device used in it (owned by the principal investigator).
