
Enterovirus D68 (EV-D68) is a virus that belongs to the D species of the Enterovirus genus in the family Picornaviridae. It was first described in 1962 in California as rhinovirus 87 as an agent involved in paediatric respiratory infections.1 In 2014 a significant outbreak of respiratory infections caused by EV-D68 was reported in the United States that affected more than one thousand patients.2 Due to this circumstance, several countries started assessing for the presence of this virus in cases of upper and lower respiratory tract infections in children and adults. Infection by this virus has been reported in France, Italy, Netherlands and Germany, among other European countries.2,3
In Spain, there have been a few reports of isolated acute respiratory infection (ARI) associated with EV-D68, both in adults and in children, and in the community and in the hospital.4–6 We think that there is still little information on this type of infections, and thus believed it would be interesting to analyse the ARIs caused by EV-D68 over a period of eight months.
We analysed the presence of enterovirus and other respiratory viruses in respiratory samples (nasopharyngeal aspirate or throat swab) obtained between July 2015 and March 2016 in paediatric patients (age<15 years) with suspected ARI.
Viral detection was performed by means of a commercially available real-time RT-PCR gene amplification technique that simultaneously detects and distinguishes 16 different viruses (Allplex® Respiratory Full Panel Assay; Seegene, South Korea). This assay can differentiate between enterovirus and rhinovirus, but cannot be used to serotype enteroviruses. Samples that tested positive for enterovirus were submitted to the National Microbiology Centre (Centro Nacional de Microbiología, Madrid), where the final serotyping was performed.
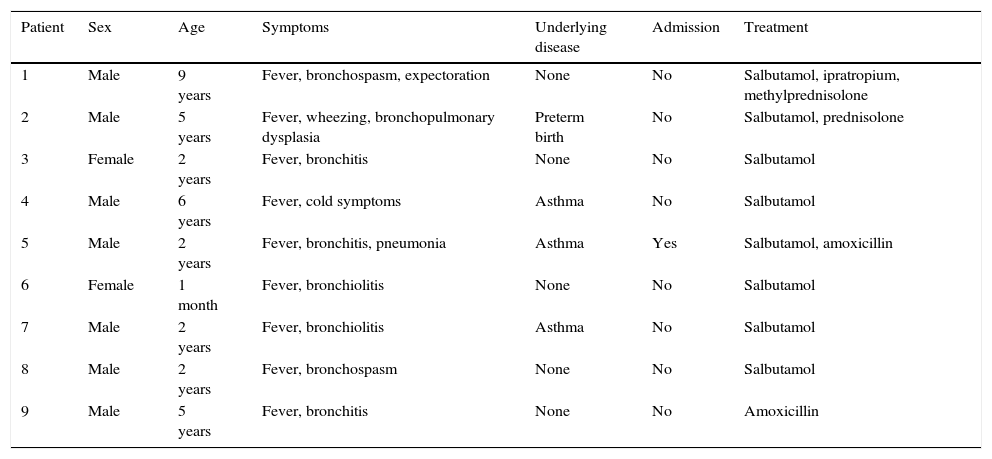
We analysed 2827 respiratory samples collected in the period under study, of which 1646 (58.2%) tested positive (some virus was detected). Of the positive samples, 88 (5.3%) corresponded to enterovirus, and only 78 strains could be serotyped (88.6%), with identification of EV-D68 in nine patients (11.5%). The nine cases of EV-D68 infection amounted to 0.5% of all positive samples and 0.3% of the total samples analysed. Other enteroviruses detected in the sample included coxsackievirus A13 (16.6%), coxsackievirus A6 (76%) and coxsackievirus B4 (7.6%). Table 1 presents the main clinical characteristics of these infections. All were community-acquired infections that occurred in isolation, and all patients had positive outcomes, including the one that required admission to the hospital.
Main characteristics of patients with acute respiratory infections caused by EV-D68.
| Patient | Sex | Age | Symptoms | Underlying disease | Admission | Treatment |
|---|---|---|---|---|---|---|
| 1 | Male | 9 years | Fever, bronchospasm, expectoration | None | No | Salbutamol, ipratropium, methylprednisolone |
| 2 | Male | 5 years | Fever, wheezing, bronchopulmonary dysplasia | Preterm birth | No | Salbutamol, prednisolone |
| 3 | Female | 2 years | Fever, bronchitis | None | No | Salbutamol |
| 4 | Male | 6 years | Fever, cold symptoms | Asthma | No | Salbutamol |
| 5 | Male | 2 years | Fever, bronchitis, pneumonia | Asthma | Yes | Salbutamol, amoxicillin |
| 6 | Female | 1 month | Fever, bronchiolitis | None | No | Salbutamol |
| 7 | Male | 2 years | Fever, bronchiolitis | Asthma | No | Salbutamol |
| 8 | Male | 2 years | Fever, bronchospasm | None | No | Salbutamol |
| 9 | Male | 5 years | Fever, bronchitis | None | No | Amoxicillin |
Although there are many studies devoted to most types of enterovirus infection, this is not the case regarding their involvement in ARIs. Historical studies seem to suggest that enteroviruses are the main aetiological agents in ARIs in the summer months, possibly accounting for 23–27% of all viruses detected during this season of the year.2,3 Although when its involvement is analysed over the course of an entire year, it declines to 4–6%.3 The incidence of ARIs caused by EV-D68 in Spain corresponds to between 0.94% and 2% of analysed samples4,5; in our study, the percentage found was somewhat lower, of 0.5%, but it appears that its incidence may change based on the season under study (peaking in the summer).2,3
In Spain, twenty cases have been described to present in patients aged 1 month to 5 years4–6; our patients were slightly older, with ages ranging between 1 month and 9 years. The mean age reported in the North American outbreak was 5 years, although the range was 15 days to 15 years.2
Despite the severity of the ARIs caused by EV-D68 reported in relation to the American outbreaks, the cases described in Europe seemed to be less severe.2 Our patients only presented with fever and mild to moderate respiratory symptoms that did not require hospital admission. Only one patient (11%) developed pneumonia requiring three days of hospitalisation; however, in the study by Calvo et al.,4 83% of patients had to be admitted. In the United States outbreak, 59% of patients were admitted to paediatric intensive care units due to the severity of their respiratory disease.2 In opposition, only 6.8% required admission to intensive care in a study conducted in Canada.2
Some studies have demonstrated that the presence of underlying disease, especially respiratory, could facilitate infection by EV-D68.2 In our study, four patients (44.4%) had this type of disease.
The evidence from this pilot study suggests that ARIs caused by EV-D68 in Europe are not associated with the clinical severity that has been observed in the outbreaks in North America, although patient comorbidity could be a determinant of its pathogenicity.
Please cite this article as: Reina J, Cabrerizo M, Ferrés F. Infecciones respiratorias agudas comunitarias causadas por enterovirus D68 (EV-D68). An Pediatr (Barc). 2017;86:158–159.
