





To describe the temporal trend and distribution of chromosomal congenital abnormalities (CA) in the Valencia Region, in less than one year olds, during the period 2007–2011.
MethodologyLive births, still births and termination of pregnancy due to foetal anomaly between 2007 and 2011 with chromosomal CA (Q90-Q99.9 codes of the 10th International Classification of Diseases –British Paediatric Association) were selected from the CA population-based Registry of Valencia Region. The prevalence per 10000 births for the chromosomal CA and for the different types of chromosomal syndromes with 95% confidence intervals was calculated. The analysis was performed by calculating prevalences and data were compared using Pearson Chi-squared test.
ResultsA total of 895 cases were found, representing a prevalence of 33.5 per 10000 births (95% CI: 31.0–35.9), highlighting five syndromes: Down's, Edward's, Patau, Turner and Klinefelter. The prevalence of chromosomal CA and Down's syndrome were stable over the period, except in 2010. Down's was the most frequent chromosomal CA (67% of the cases), and the most frequent termination of pregnancy type was for foetal anomaly (69%). Cardiac heart defects represented 70.3% of the associated congenital anomalies. Mothers of children with chromosomal CA were mainly Spanish (73.3%). The age group of mothers over 39 years had a higher prevalence (133.0 per 10000 births). The province of Castellón had the highest prevalence, 39.1 per 10000 births.
ConclusionsThe prevalence has remained stable over the five years, excluding the significant decline in 2010, for chromosomal CA detected and two of the major syndromes. Chromosomal CA are an important public health problem as they represent 15% of all CA identified in the Valencia Region, and agrees with the European data.
Describir la tendencia y la distribución de las anomalías congénitas (AC) cromosómicas en la Comunitat Valenciana, en menores de un año, durante el periodo 2007-2011.
MetodologíaSe seleccionó a los nacidos vivos y muertos e interrupciones voluntarias del embarazo por AC entre 2007 y 2011 del Registro Poblacional de AC de la Comunitat Valenciana con AC cromosómica (códigos Q90-Q99.9 de la 10.ª Clasificación Internacional de Enfermedades-British Pediatric Asociation). Se calcularon la prevalencia por 10.000 nacidos y sus intervalos de confianza (IC) al 95% para el conjunto de AC cromosómica y algunos síndromes cromosómicos. El análisis se realizó mediante el cálculo de prevalencia y se compararon los datos utilizando la prueba de la chi al cuadrado de Pearson.
ResultadosSe identificaron 895 casos de AC cromosómicas, lo que supuso una prevalencia de 33,5 por 10.000 nacimientos (IC del 95%, 31,0-35,9), siendo los síndromes más frecuentes: Down, Edwards, Patau, Turner y Klinefelter. Las prevalencias de las AC cromosómicas y síndrome de Down fueron estables en el periodo, excepto en 2010. El Down fue la AC cromosómica más frecuente (67%) y las interrupciones voluntarias del embarazo por AC, el tipo de finalización del embarazo mayoritario (69%). Entre las AC asociadas, las cardiopatías congénitas representaban un 70,3%. La mayoría de las madres de niños con AC cromosómicas eran españolas (73,3%) y en el grupo de edad de madres mayores de 39 años se identificó la prevalencia más elevada (133,0 por 10.000 nacimientos). La provincia de Castellón presentó la prevalencia más elevada, 39,1 por 10.000 nacimientos.
ConclusionesLa prevalencia se ha mantenido estable durante el quinquenio, exceptuando el descenso significativo del año 2010, detectado para AC cromosómicas y 2 de los principales síndromes. Las AC cromosómicas son un importante problema de salud pública, ya que representan el 15% de todas las AC identificadas en la Comunitat Valenciana, coincidiendo con los valores de Europa.
The term chromosomal congenital anomaly (CA) refers to any morphological, structural, functional or molecular developmental anomaly affecting the number or structure of chromosomes. Chromosomal CAs represent approximately 15% of the major CAs diagnosed before one year of age in Europe and are associated with 25% of perinatal deaths due to CA.1 The most common chromosomal CAs are trisomy 21, 18 and 13.2
Chromosomal CAs contribute to high perinatal and infant mortality and can provoke miscarriage. Moreover, many cases do not reach birth due to voluntary termination of pregnancy for CA (VTP-CA). The physical and/or mental disabilities they cause tend to be severe, in most cases, affecting the patient for life, and this entails a high healthcare, social and emotional cost due to the chronic nature of these diseases.3–6 Management of chromosomal CAs requires a multidisciplinary approach to the ongoing assessment and followup of the associated CAs and acquired disorders, since knowledge of these associated conditions is important for healthcare professionals treating these patients.
Early diagnosis is therefore important in order to establish the best strategy designed to minimise the risks to the children's health, because increased mortality represents a serious and major problem in these patients.7
It is also important to develop information systems, since they are the basis for monitoring and for clinical and epidemiological investigation of CAs. Such systems have been evolving to cover a range of issues related to epidemiology, such as aetiological investigation and assessment of healthcare services.6
In this context, the Population-Based Congenital Anomalies Register was established in the Comunidad Valenciana (Valencian Community: VC) in 2009, as an integral part of the Rare Diseases Information System, following the methodology, criteria and quality controls of the European Network of Population-Based Registers for the Epidemiological Surveillance of Congenital Anomalies (EUROCAT),8 making it possible to compare the data with other registers, both Spanish and European, and thereby progress in research on CAs.
This enables us to describe the trend and distribution of chromosomal CAs in infants less than one year old born in the VC during the period from 2007 to 2011, which is the purpose of this article.
Material and methodsWe conducted a cross-sectional epidemiological study of chromosomal CAs using data obtained from the Population-Based Congenital Anomalies Register of the Valencian Community (PCAR-VC).
We identified cases by searching the Conjunto Mínimo Básico de Datos (Basic Minimum Data Set), the Perinatal Mortality Register9 of the VC and the Register of Voluntary Terminations of Pregnancy in the VC. In addition, we used the Metabolic Disorders Register of the VC as a supplementary source for obtaining data on deliveries, newborns and mothers. On the basis of these sources we reviewed the clinical documentation, enabling us to confirm the patients with CAs and collect the clinical and epidemiological information. Once the cases were confirmed they were incorporated into the PCAR-VC.
For this study we selected the live births (LB), stillbirths (SB) and VTP-CAs during the period 2007–2011 with at least one chromosomal CA (codes Q90-Q99.9 in the 10th Revision of the International Classification of Diseases-British Paediatric Association) whose mothers were resident in the VC. Cases are included in this register following the protocol formulated and agreed upon by the member registers of EUROCAT.8 Therefore major CAs (life-threatening malformations requiring surgery or involving severe sequelae) are registered, and minor CAs (those that are not associated with significant sequelae or changes in quality of life or life expectancy) are registered only if they are associated with a major CA.
The case variables included in the analysis were year of birth or of VTP-CA, type of chromosomal CA, type of end of pregnancy and associated CAs. The variables analysed pertaining to the mothers were province of residence at the time of birth or of VTP-CA, age at delivery or VTP-CA and country of birth.
We calculated the overall and annual prevalences of chromosomal CAs, and also their 95% confidence intervals (95% CIs). We studied the time trend for the period 2007–2011. The prevalences of chromosomal CAs and their 95% CIs were also obtained for the variables being analysed and the data were compared using Pearson's chi-square test.
In addition, the type of end of pregnancy (LB, SB or VTP-CA) that occurred with the chromosomal CAs was described and the trend in VTP-CAs over the five-year period was analysed.
The most common CAs associated with chromosomal CAs were identified and grouped by body systems to obtain the frequency of each, and the group with most cases was analysed in order to establish the specific CAs with the largest presence.
An analysis by province was conducted to describe the geographical variability of chromosomal CAs in the VC, which enabled us to study the distribution in the 3 provinces and calculate their prevalences and 95% CIs, using births in each province of the VC for the whole period from 2007 to 2011 as a reference.
Finally, to analyse the association of maternal age and country of birth and the risk of chromosomal CAs, we established maternal age subgroups by five-year intervals, on the one hand, to observe the distribution of cases of chromosomal CAs, and the percentages and their 95% CIs were calculated. On the other hand, the percentages of cases according to the mother's country of birth were obtained and the prevalences and their 95% CIs were calculated, using births in the VC by maternal nationality (Spanish or foreign) as a reference, and Pearson's chi-square test was performed to determine significant differences.
ResultsA total of 895 cases of infants under one year old with at least one chromosomal CA were recorded in the VC in the period 2007–2011, representing a prevalence of 33.5 per 10000 births (95% CI, 31.0–35.9).
Table 1 shows the distribution of cases of chromosomal CAs by syndrome type. Down syndrome (DS) was the most frequent among the cases of chromosomal CAs, accounting for 9.8% of total CAs in the VC, with a prevalence of 22.4 per 10000 births (95% CI, 20.5–24.4).
Total number of cases, proportion and prevalence of chromosomal syndromes, Valencian Community, 2007–2011.
| Syndrome | Total cases | Percentage | Prevalence per 10000 births |
|---|---|---|---|
| Down | 600 | 67.04 | 22.4 (95% CI, 20.5–24.4) |
| Edward | 104 | 11.62 | 3.8 (95% CI, 3.1–4.7) |
| Patau | 41 | 4.58 | 1.5 (95% CI, 1.0–2.0) |
| Turner | 41 | 4.58 | 1.5 (95% CI, 1.0–2.0) |
| Klinefelter | 25 | 2.79 | 0.9 (95% CI, 0.5–1.3) |
| Others | 84 | 9.38 | 3.1 (95% CI, 2.4–3.9) |
| ChrCAs | 895 | 100 | 33.4 (95% CI, 31–35.9) |
ChrCAs: chromosomal congenital anomalies.
In the time trend it was observed that the prevalences over the period remained stable, except in 2010, when there was a statistically significant reduction. This phenomenon occurred both at the level of chromosomal CAs as a whole, whose prevalence in 2010 was 27.5 per 10000 births (95% CI: 25.3–29.7), and particularly for DS and Patau, whose prevalences showed a significant decrease compared with the preceding and following years (Fig. 1).

No statistically significant differences were found with respect to birth year when DS was compared with the other syndromes (P>.47).
Most of the recorded cases were VTP-CAs, followed by LBs and SBs. When each type of syndrome was observed individually, Turner syndrome showed the highest proportion of VTP-CAs, with 87.8% of the 41 cases, and DS had the lowest, with 69.0% of 600 cases. As for LBs, the highest proportion was observed for DS, with 30.3%, and the lowest for Turner. Edwards syndrome showed the largest number of SBs, with a proportion of 7.7% of all cases (Table 2).
Cases and percentages of chromosomal syndromes by type of end of pregnancy, Valencian Community, 2007–2011.
| Syndrome | Live birth | Stillbirth | VTP-CA | Total cases | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Down | 182 | 85.9 | 4 | 28.6 | 414 | 70.8 | 600 |
| Edward | 14 | 6.6 | 8 | 57.1 | 82 | 14.0 | 104 |
| Patau | 7 | 3.3 | 1 | 7.1 | 33 | 5.6 | 41 |
| Turner | 5 | 2.4 | 0 | 0 | 36 | 6.2 | 41 |
| Klinefelter | 4 | 1.9 | 1 | 7.1 | 20 | 3.4 | 25 |
| Total | 212 | 100 | 14 | 100 | 585 | 100 | 811 |
VTP-CA: voluntary termination of pregnancy for congenital anomaly.
During the study period, a pattern of stability was observed in the proportion of VTP-CAs, which remained at around 70% of cases, except in 2010, for which the figure was 64.8%.
Statistically significant differences between DS and Edwards and Turner syndromes were found with respect to the distribution of categories for the type of end of pregnancy variable (LB, SB and VTP-CA) (P=0.038).
There was a total of 518 CAs associated with the principal syndromes (regardless of whether they were major or minor CAs) (Table 3). It should be noted that a case of chromosomal CA could have more than one CA associated with it; a total of 220 patients with chromosomal CAs that also had another CA were identified. Of these patients, 58.6% had more than one associated CA. The most frequent CAs were cardiac CAs, which represented 70.3% of the associated CAs identified, followed by musculoskeletal and urinary malformations, the proportions of which were 5.8% in both cases. Within the category of cardiac CAs atrial and ventricular septal defects were the most frequent, with proportions of 27.9% and 20.0% respectively.
Distribution of associated congenital anomalies identified in cases of chromosomal congenital anomalies, by congenital anomaly groups, Valencian Community, 2007–2011.
| Congenital anomaly group | Associated congenital anomaly (n) | Percentage |
|---|---|---|
| Circulatory system | 364 | 70.3 |
| Urinary system | 30 | 5.8 |
| Musculoskeletal system | 30 | 5.8 |
| Digestive system | 19 | 3.7 |
| Nervous system | 18 | 3.5 |
| Genital organs | 14 | 2.7 |
| Eye, ear, face, neck | 13 | 2.5 |
| Respiratory system | 9 | 1.7 |
| Other congenital anomalies | 9 | 1.7 |
| Chromosomal congenital anomalies | 7 | 1.4 |
| Others unspecified | 5 | 1 |
| Total | 518 | 100 |
In geographical terms it was established that half the cases (48.4%) occurred in the province of Valencia, followed by Alicante (36.9%) and Castellón, with 14.4% of the cases of chromosomal CAs. It was observed that the prevalence of chromosomal CAs in the province of Castellón was higher than in the other provinces, standing at 39.1 chromosomal CAs per 10000 births (95% CI, 36.5–41.7), whereas the figures for Alicante and Valencia were 35.3 (95% CI, 32.8–37.8) and 31.2 per 10000 births (95% CI, 28.9–33.5) respectively.
The mother's country of birth was not recorded in 9.4% of cases. Of the mothers included in the study 17.3% were foreign, with Morocco and Romania being the most frequent countries of origin. The prevalence of chromosomal CAs in Spanish mothers with children affected by chromosomal CAs in the VC for the period was 33.1 per 10000 births (95% CI, 30.6–35.5) and in foreign mothers it was 23.94 per 10000 births (95% CI, 21.9–26.0); thus statistically significant differences were identified (P=.0004).
In particular, a significant increase occurred between 2007 and 2008 in the prevalence for foreign mothers, which went from 17.6 (95% CI, 15.8–19.4) to 29.32 (95% CI, 27.1–31.6) per 10000 births. However, a significant decrease was identified from 2010 to 2011, when the figure went from 28.1 (95% CI, 25.8–30.3) to 17.8 (95% CI, 16.1–19.6) per 10000 births. A similar situation was observed in the prevalence in Spanish mothers, since it went from 38.2 per 10000 births (95% CI, 35.6–40.8) in 2009 to 24.9 (95% CI, 22.8–27.0) in 2010. Moreover, 2010 was the only year in which foreign mothers showed a higher prevalence than Spanish mothers.
The mean age of the mother was 35 years (95% CI, 24–45) and the range was 14–50 years. It was observed that mothers aged between 35 and 39 were those with the highest proportion of cases of chromosomal CAs (38.5%) and a prevalence of 58.0 per 10000 births (95% CI, 54.8–61.2), followed by the 30 to 34-year-old group with 28.4% of cases (25.0 per 10000 births; 95% CI, 22.9–27.1) and by the group aged over 39, with almost 17.9% (133.0 per 10000 births; 95% CI, 128.2–137.8). The group of mothers aged over 39 years had the highest prevalence in every year. It was observed that the 30- to 34-year-old group showed the largest decrease of all the age groups in 2010 (Fig. 2).

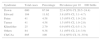
On comparing the various chromosomal syndromes with the age groups, it can be seen that from the age of 30 there was a considerable increase in the number of cases and that the group of mothers aged over 39 years had the highest prevalence for nearly all syndromes. No cases of Klinefelter and Patau syndromes were found in mothers aged <25 years (Table 4).
Prevalence per 10000 births of chromosomal syndromes by maternal age groups, Valencian Community, 2007–2011.
| Maternal age group (years) | Down S. | Edwards S. | Patau S. | Turner S. | Klinefelter S. |
|---|---|---|---|---|---|
| <20 | |||||
| n | 8 | 0 | 0 | 1 | 0 |
| Prevalence | 11.8 | 0 | 0 | 1.48 | 0 |
| 95% CI | 10.4–13.4 | 0 | 0 | 1.0–2.0 | 0 |
| 20–24 | |||||
| n | 21 | 5 | 0 | 1 | 0 |
| Prevalence | 8.96 | 2.13 | 0 | 0.42 | 0 |
| 95% CI | 7.7–10.2 | 1.5–2.7 | 0 | 0.1–0.7 | 0 |
| 25–29 | |||||
| n | 50 | 10 | 1 | 11 | 2 |
| Prevalence | 8.72 | 1.74 | 0.17 | 1.92 | 0.34 |
| 95% CI | 7.5–10.0 | 1.2–2.3 | 0.0–0.3 | 1.3–2.5 | 0.1–0.6 |
| 30–34 | |||||
| n | 162 | 25 | 16 | 12 | 8 |
| Prevalence | 15.95 | 2.46 | 1.57 | 1.18 | 0.79 |
| 95% CI | 14.3–17.6 | 1.8–3.1 | 1.0–2.1 | 0.7–1.6 | 0.4–1.2 |
| 35–39 | |||||
| n | 240 | 38 | 14 | 14 | 10 |
| Prevalence | 40.5 | 6.41 | 2.36 | 2.36 | 1.69 |
| 95% CI | 37.8–43.2 | 5.3–7.5 | 1.7–3.0 | 1.7–3.0 | 1.1–2.2 |
| >39 | |||||
| n | 112 | 25 | 10 | 2 | 5 |
| Prevalence | 92.49 | 20.65 | 8.26 | 1.65 | 4.13 |
| 95% CI | 88.5–96.5 | 18.7–22.6 | 7.1–9.5 | 1.1–2.2 | 3.3–5.0 |
95% CI, 95% confidence interval.
The only significant differences with respect to the distribution of maternal age groups (under 20, 20–24, 25–29, 30–34, 35–39, over 39 years) were detected when comparing DS and Klinefelter syndrome (P=.004).
DiscussionThe prevalence of CAs in the VC in the period 2007–2011 was similar to that described by the various European countries belonging to the EUROCAT network.10 However, the prevalence of chromosomal CAs (33.5 per 10000 births in the CV) varies widely. Countries such as Portugal, Ireland and Ukraine show lower prevalences, whereas the registers in France, Germany, Switzerland and the Basque Country11 (35.8 per 10000 births) reach higher values.
The prevalence of DS in the VC shows intermediate values, similar to those obtained in other registers, such as those of Italy and Belgium.
In the VC chromosomal CAs were the second most prevalent subgroup of CAs, a striking feature being the notable differences among the various syndromes. In Europe the most frequent are trisomy 21, 18 and 13,2 coinciding with the results obtained in the VC.
The statistically significant decrease in the prevalence of chromosomal CAs in 2010 can be explained, at least in part, by the following: (a) the number of Spanish mothers fell sharply, from 151 in 2009 to 97 in 2010 (coinciding with the differences identified in relation to the mother's country of birth in a previous study,12 although in that case the higher risk was identified in foreign mothers); (b) in 2010 there was an increase in the proportion of cases in mothers aged between 35 and 39 years, showing the highest figure for this group in the five-year period, followed by mothers aged 30–34 years and by those over 39, identifying the mother's age as an important factor and confirming what had already been established in previous studies,13–15 and (c) the number of VTP-CAs performed that same year fell to a value below 65.0%.16 This may be due to the fact that in 2010 the Ley de Salud Sexual y Reproductiva (Sexual and Reproductive Health Act)17 came into force in Spain and a decrease in the total number of VTP-CAs was observed in the VC. This Act allows women to interrupt pregnancy at their own request, with no requirement for justification and/or prenatal examination, before the 14th week, regardless of their age. There could therefore be a loss of information due to under-reporting of such cases, and the quality of the information could be affected, always bearing in mind what is involved in introducing a new application or information system. Nevertheless, a decrease had already been identified in 2009, even greater than that observed in 2010.
For chromosomal CAs in general, VTP-CAs remained stable, except for the decrease in 2010. A total of 54867 VTPs were notified for all causes in the VC during the study period, DS being the main anomaly for which they were performed (223 VTP-CAs in 2008 and 249 in 2011), followed by cardiac CAs, CAs of the nervous system and Edwards syndrome.16,18
The increase in prenatal detection of CAs, with foetal karyotyping as the most reliable way of identifying anomalies, has made it possible to ascertain the prognosis of these babies and has given rise to a higher rate of VTP-CA, which has raised the proportion of children born with normal phenotypes and without abnormalities,1 thereby minimising the risks to foetuses and expectant mothers. In addition, advances in detection techniques are enabling us to discover ever smaller and more specific chromosomal abnormalities, as well as nongenetic factors of an environmental kind.19
On the other hand, geographical analyses make it possible to identify regional variations in the prevalence of chromosomal CAs in different areas.20 In our study geographical differences were identified between the provinces of the VC: a higher prevalence of chromosomal CAs was observed in Castellón, which could be due to the higher frequency of cardiac CAs in that province (because of their association with chromosomal CAs), already described in previous studies.21 However, studies need to be conducted to enable possible environmental risk factors to be identified, also taking sociocultural and demographic factors into account, since some areas of Castellón are notable for being predominantly industrial, and this could be related to the higher prevalence values and affect the association between chromosomal CAs and cardiac CAs.
Despite the fact that association of CAs with syndromes is unusual,22,23 we found 220 cases of chromosomal CAs with a total of 518 associated CAs. Of these associations, 70% were of cardiac origin, consistent with the results obtained in other Spanish and European studies, since cardiac CAs are the most common malformations. Ventricular and atrial septal defects together with patent ductus arteriosus were already identified as the anomalies with the highest prevalence in the VC in the period 1999–2008,21 and the same increase was observed in other studies in England and Turkey.24,25
A significant difference was identified in the risk of chromosomal CAs according to the maternal country of birth, as has previously been emphasised.12 The mother's age is very important, since it is the only well-established risk factor for DS. The most prominent finding is that the risk increases from 35 years of age; but it is less established as a risk factor for nonchromosomal CAs.13-15 We find the opposite case in younger mothers, who have a lower risk of chromosomal CAs but in whom an increase in nonchromosomal anomalies has been described, particularly congenital abdominal defects.26,27
With regard to the limitations of the study, it should be mentioned that variables pertaining to the mother, such as comorbidity and medication taken during pregnancy, were not included, but those responsible for the PCAR-VC are working to improve the information gathered and thereby broaden the study of anomalies. Moreover, the Conjunto Mínimo Básico de Datos Hospitalarios (Basic Minimum Hospital Data Set) was previously the only source of information for these studies (it had high specificity, high predictive values and low sensitivity28,29), but the use of the PCAR-VC has led to improvement and progress in the analysis of these diseases, as it uses multiple sources of information, thus expanding the data and making it possible to calculate incidence and prevalence.30 The PCAR-VC is therefore currently the best option for monitoring CAs and studying their epidemiological aspects.6,31
In conclusion, the prevalence of chromosomal CAs in the VC during 2007–2011 remained stable over the five-year period, apart from the statistically significant decrease detected in 2010 for chromosomal CAs as a whole and for two of the main syndromes. Furthermore, chromosomal CAs stand out as an important public health problem, since they represent approximately 15% of all the CAs identified in the VC, coinciding with the proportion this group occupies in the EUROCAT database, which includes the cases in the European population-based CA registers.
FundingThis research study was made possible by a grant from the Fondo de Investigaciones Sanitarias (Healthcare Research Fund) (FIS PI10/01676) and by the SpainRDR Project (PR11/122).
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Gimeno-Martos S, Cavero-Carbonell C, López-Maside A, Bosch-Sánchez S, Martos-Jiménez C, Zurriaga O. Anomalías cromosómicas: la experiencia del Registro de Anomalías Congénitas de la Comunitat Valenciana. An Pediatr (Barc). 2016;84:203–210.
Previous presentations: I Jornadas de Investigación Integral en Ciencias Ómicas y Estilos de Vida; 11–13 June 2014; Valencia, Spain. XXXII Reunión Científica de la Sociedad Española de Epidemiología; 3–5 September 2014; Alicante, Spain. I Congreso de Biomedicina PreDocs Valencia; 27 and 28 November 2014; Valencia, Spain.

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals