Treatment with cystic fibrosis transmembrane conductance regulator (CFTR) modulators has greatly improved the prognosis of patients with cystic fibrosis (CF).1 One of these novel drugs is the combination of elexacaftor/tezacaftor/ivacaftor (ETI) for triple therapy, which is indicated in patients who carry the F508del change in at least one allele of the CFTR gene, although favourable outcomes have also been reported in studies in vitro and in patients with other class II changes (affecting CFTR protein processing).2–4 One of the potential effects of ETI therapy, although rare, is cholecystitis, which has been reported in small adult case series.5,6 We present the case of a boy with CF who started ETI therapy and complained a few days later of pain in the upper right region of the abdomen compatible with acute cholecystitis.
The patient was a boy aged 9 years with CF who carried the N1303K/R334W variants, without pancreatic insufficiency, with a history of chronic cough of 2 years’ duration and mild to moderate pulmonary exacerbations and detection of Staphylococcus aureus in throat swab specimens. He was managed with nebulised 3% hypertonic saline solution, oral azithromycin given 3 days a week and chest physiotherapy. The forced spirometry assessment was normal, with a forced expiratory volume in 1 second (FEV1) of 1.92 L (z score of −0.7 in relation to the reference group). The computed tomography of the lungs showed generalised cylindrical bronchiectasis, mucus plugging, involvement of small-calibre bronchi with mosaic attenuation and a Bhalla score of 15 (threshold of normal: 25). At the gastrointestinal level, the patient had adequate pancreatic function and growth (52nd percentile for weight and 83rd for height), but there was evidence of hepatobiliary involvement in the abdominal ultrasound (gallbladder sludge), managed with ursodeoxycholic acid. Due to progressive clinical and radiological pulmonary worsening in the last 3 years, the decision was made to initiate ETI therapy based on recently published articles that reported a favourable response in vitro and in patients carrying the N1303K variant, as did ours. The patient was given the adult dose for more than 30 kg of body weight (2 tablets containing 75 mg of ivacaftor, 50 mg of tezacaftor and 100 mg of elexacaftor in the morning and 1 tablet containing 150 mg de ivacaftor at night). Six days after starting treatment, the patient reported colicky abdominal pain in the right hypochondrium and epigastrium. The patient had no fever, choluria, vomiting or diarrhoea. In the physical examination, the skin colour was normal, and the patient experienced pain on palpation of the right hypochondrium with a positive Murphy sign. The abdominal ultrasound showed multiple hyperechoic spots suggestive of biliary sludge in the gallbladder; inflammatory changes and oedema of the gallbladder wall, with diffuse wall thickening and markedly increased blood flow on Doppler, along with inflammatory changes in the adjacent adipose tissue (Fig. 1), while all other organs, including the pancreas, had a normal appearance. Laboratory tests revealed levels of C-reactive protein, procalcitonin, white blood cells, pancreatic lipase, transaminases and bilirubin in the normal range. Given the findings compatible with acute cholecystitis, ETI was discontinued and analgesia provided to the patient, which achieved resolution of symptoms within 48 hours. Two months later, a follow-up abdominal ultrasound evinced resolution of the inflammatory process, and treatment with ETI was reintroduced in gradually increasing doses. Eventually, the indicated dose for the patient’s weight was reached and could be maintained without additional adverse events. Table 1 summarises the changes observed at 8 weeks of treatment, the most salient of which was a 24 mEq/L decrease in sweat chloride.
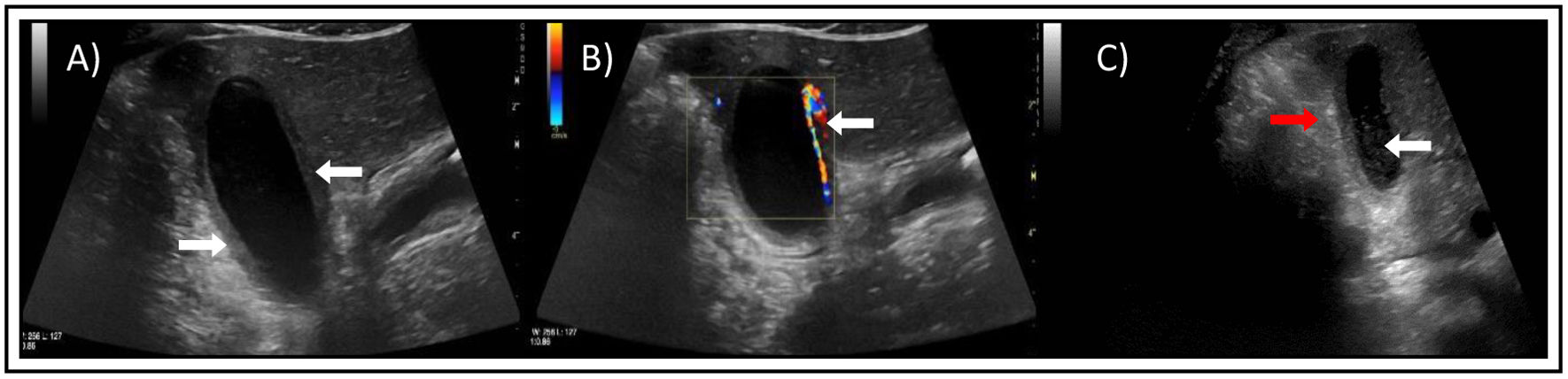
 Inflammatory-oedematous changes in gallbladder wall with diffuse wall thickening (white arrows). (B) Marked increase in blood flow on Doppler (white arrow). (C) Visualization of spots in the gallbladder compatible with biliary sludge (white arrow) and oedema of surrounding fat tissue (red arrow).")
Abdominal ultrasound. (A) Inflammatory-oedematous changes in gallbladder wall with diffuse wall thickening (white arrows). (B) Marked increase in blood flow on Doppler (white arrow). (C) Visualization of spots in the gallbladder compatible with biliary sludge (white arrow) and oedema of surrounding fat tissue (red arrow).
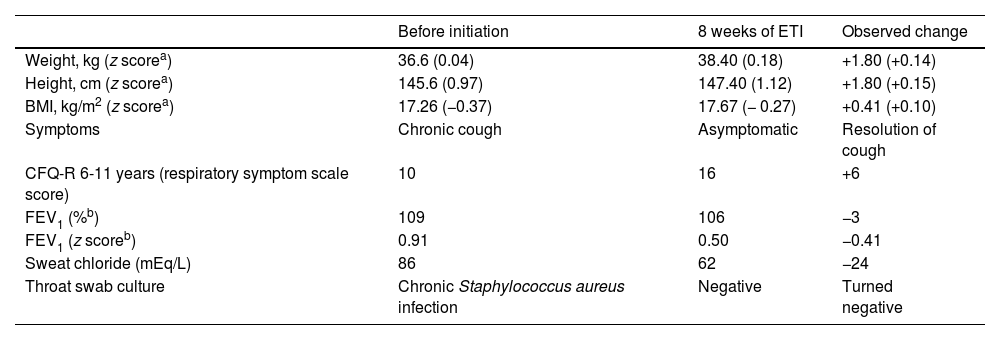
Changes observed at 8 weeks of treatment.
| Before initiation | 8 weeks of ETI | Observed change | |
|---|---|---|---|
| Weight, kg (z scorea) | 36.6 (0.04) | 38.40 (0.18) | +1.80 (+0.14) |
| Height, cm (z scorea) | 145.6 (0.97) | 147.40 (1.12) | +1.80 (+0.15) |
| BMI, kg/m2 (z scorea) | 17.26 (−0.37) | 17.67 (− 0.27) | +0.41 (+0.10) |
| Symptoms | Chronic cough | Asymptomatic | Resolution of cough |
| CFQ-R 6-11 years (respiratory symptom scale score) | 10 | 16 | +6 |
| FEV1 (%b) | 109 | 106 | −3 |
| FEV1 (z scoreb) | 0.91 | 0.50 | −0.41 |
| Sweat chloride (mEq/L) | 86 | 62 | −24 |
| Throat swab culture | Chronic Staphylococcus aureus infection | Negative | Turned negative |
CFQ-R, Cystic Fibrosis Questionnaire-Revised; ETI, elexacaftor/tezacaftor/ivacaftor.
Acute cholecystitis is a rare adverse reaction to ETI therapy of which only a few cases have been reported in some case series,5,6 and may be explained by the improvement in bile flow achieved with treatment, which would dislodge calculi or gallbladder sludge that would then obstruct the cystic duct. To our knowledge, this is the sole published case concerning a paediatric patient, and discontinuation of ETI sufficed to resolve it. In most reported adult cases, cholecystectomy was required, and none of the cases resulted in severe complications. Despite the occurrence of this adverse event, triple therapy was reintroduced gradually in all patients, without recurrence of similar complications.5,6
Although nonspecific abdominal pain is one of the most frequent adverse events after initiation of ETI or other modulators, when it develops it is important to rule out conditions such as acute pancreatitis or, as was the case of our patient, biliary colic or acute cholecystitis, so we consider that performance of an abdominal ultrasound scan and laboratory tests including measurement of transaminase, bilirubin and pancreatic enzyme levels is necessary in every case.

