



Lung ultrasound has been integrated in neonatal care units as an essential tool in the evaluation of neonatal respiratory distress due to its quickness, harmlessness and high sensitivity and specificity.1 However, there are some images that pose a challenge.
We present the case of a term newborn infant that underwent a bedside ultrasound examination of the chest due to respiratory distress. Transverse-plane scanning with a linear probe can be used to rule out pneumothorax,2 and in this patient it revealed several well-demarcated hyperechoic lesions up to 2 cm in diameter confined to the myocardium (Fig. 1, Appendix B, supplemental material). The lung parenchyma presented an interstitial pattern in a gradient with a thin pleural line and lung sliding, compatible with transient tachypnoea (respiratory support for 48 h). The echocardiogram confirmed the presence of cardiac tubers, and a brain magnetic resonance evidenced subependymal tubers and nodules (major criteria), radial migration lines, subependymal nodules and cysts in the white matter (Fig. 2) which, combined with the results of genetic testing, led to the diagnosis of tuberous sclerosis type 2 (Bourneville syndrome, pathogenic TSC2 gene variant).
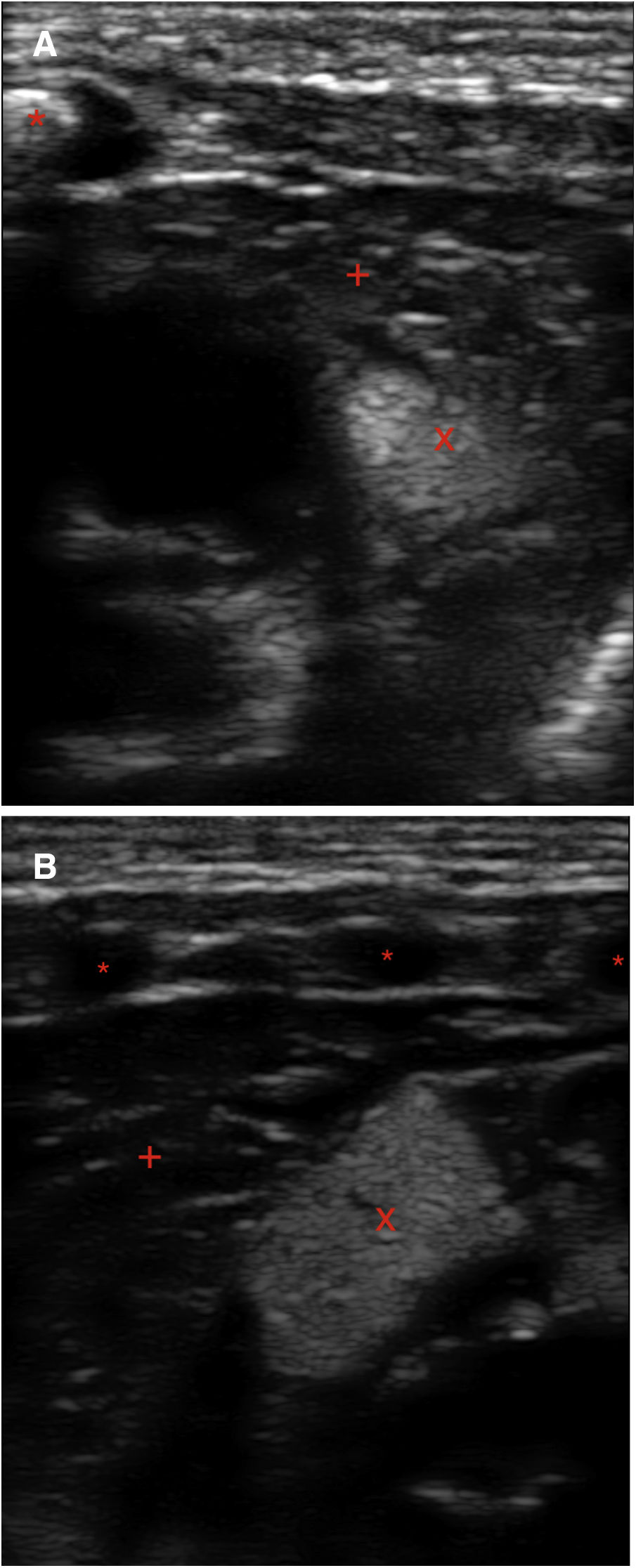
Point-of-care ultrasound of the chest. Linear probe. (A) Transverse plane at the level of the intermammary line. Visualization of sternum (*) and the masses (tubers) in the myocardium (homogeneous, hyperechoic, X). This contrasted with the decreased echogenicity of the myocardium (+). B) Left longitudinal plane: anterior arc of ribs (*), tubers (X), mediastinum (+). gr1.
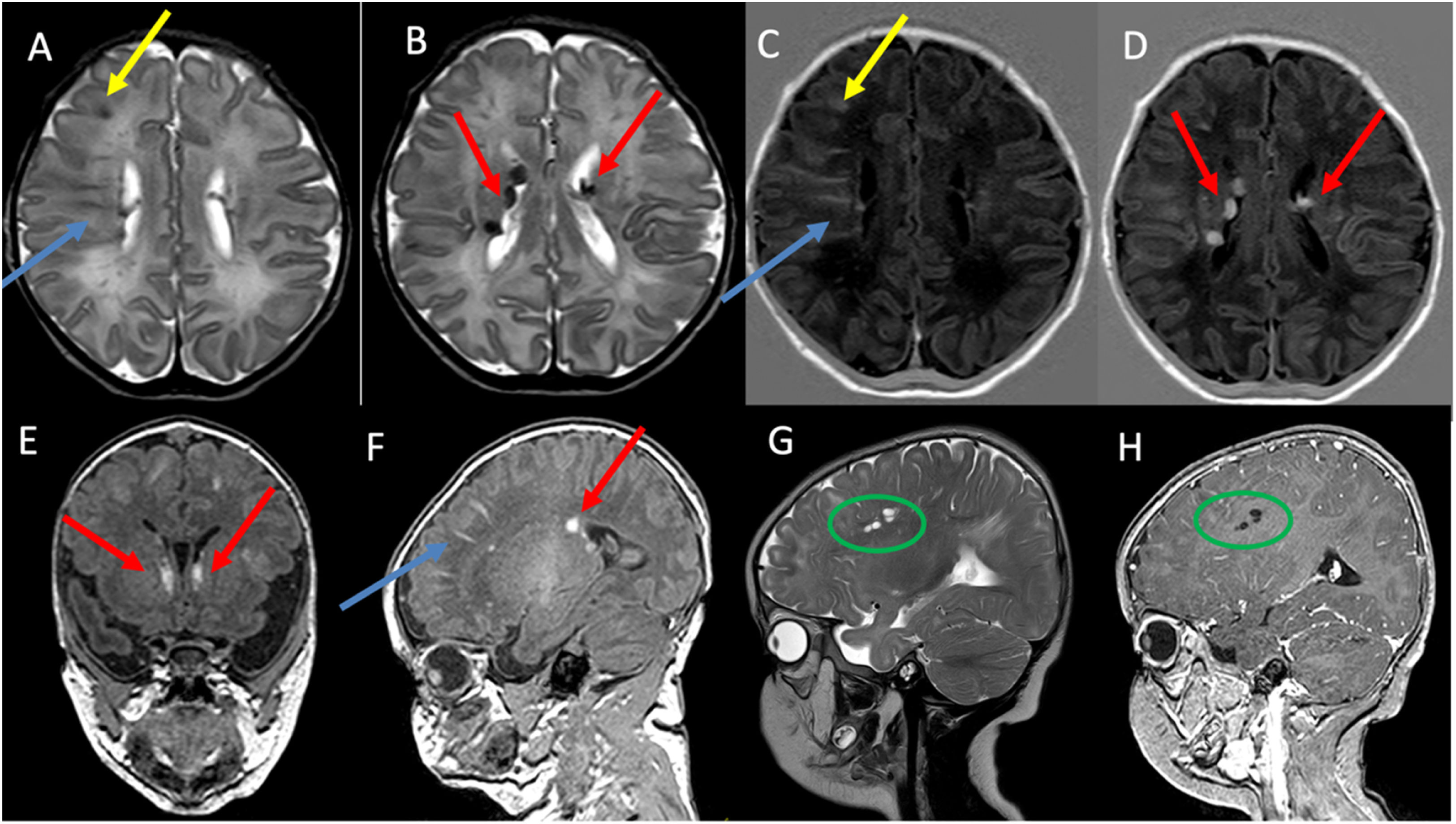
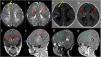
Magnetic resonance imaging of the head at 6 days post birth. Axial turbo spin echo (TSE) sequence T2-weighted images (A and B), axial T1 inversion recovery (T1IR) sequence image (C and D) Coronal T1-weigthed 3D image (E), sagittal T1-weighted 3D image (F), sagittal TSE T2-weighted image (G) and sagittal T1-weighted 3D following intravenous contrast administration (H). Visualization of cortical tubers that appeared hypointense on T2-weighted imaging and hyperintense on T1-weighted images (yellow arrows in A and C), radial migration lines in white matter (blue arrows in A, C and F), subependymal nodules (red arrows in B, D, E and F) and white matter cysts that appear hyperintense in T2-weighted images and without enhancement after contrast administration (green circle in G and H). The colour features of the figures can only be discerned in the digital version.
At present, the patient is 10 months old and receiving vigabatrin for treatment of epileptic seizures. The chest ultrasound scan allowed early diagnosis that improved the follow-up and outcomes of the patient, as he was diagnosed in the presymptomatic stage.
