







To assess the experience with oxygen therapy with a high flow nasal cannula (HFNC) in hospital on patients with asthmatic exacerbation (AE) in a paediatric ward, and to assess the clinical outcome according with the initial oxygen flow (15lpm or <15lpm).
MethodsThis was a retrospective study of children aged 4–15 years with AE admitted to a paediatric ward in a tertiary level hospital between 2012 and 2016. Two groups of patients were compared; Group 1: patients treated with HFNC, and Group 2: patients treated with conventional oxygen therapy. A logistic regression model was constructed in order to identify predictive variables of HFNC. The clinical outcome of the patients was also compared according to the initial flow of HFNC (15lpm vs. <15lpm).
ResultsThe study included a total of 536 patients with AE, 40 (7.5%) of whom required HFNC. The median age was 5 (4–6) years. Heart rate (HR), respiratory rate (RR) and pulmonary score (PS) significantly decreased at 3–6h after starting HFNC in Group 1. In the multivariate analysis, patients with high pulmonary score values and greater number of previous admissions required HFNC more frequently. Patients treated with an initial flow of 15lpm were admitted less frequently to the PICU than those with an initial flow less than 15lpm (13% vs. 47%, P=.05).
ConclusionHFNC seems to be a useful therapy for asthma exacerbation in paediatric wards. Severity of pulmonary score and the number of previous admissions could enable a risk group that needs HFNC to be identified.
Analizar la experiencia de tratamiento con OAF en pacientes ingresados por crisis asmática (CA) en una planta de hospitalización pediátrica (PHP), así como analizar la diferencia de la evolución según sean tratados de entrada con flujos de 15lpm o inferiores a 15lpm.
MétodosEstudio retrospectivo y analítico en niños (4 a 15 años) ingresados por CA en la PHP de un hospital terciario entre 2012 y 2016. Se compararon 2 grupos de pacientes: los tratados con OAF y los tratados con oxigenoterapia convencional; se construyó un modelo de regresión logística para identificar variables predictivas de necesidad de OAF. Se comparó la evolución de los pacientes en función del flujo de inicio de la OAF (15lpm vs <15lpm).
ResultadosSe incluyeron 536 pacientes con CA, de los que 40 (7,5%) precisaron OAF. La mediana de edad fue de 5 (4-6) años. La OAF en los pacientes con CA produjo una reducción en la frecuencia cardiaca, frecuencia respiratoria y Pulmonary Score en las primeras 3-6horas de tratamiento. En el análisis multivariante los pacientes con una mayor puntuación en el PS y un mayor número de ingresos previos precisaron con más frecuencia OAF. Los pacientes tratados con un flujo de inicio de 15lpm ingresaron menos frecuentemente en UCIP que aquellos con flujo inicial inferior a 15lpm (13% vs. 47%, p=0,05).
ConclusiónLa OAF como tratamiento de las CA en las PHP parece ser una terapia de gran utilidad. El Pulmonary Score y el número de ingresos previos permite identificar un grupo de riesgo de precisar OAF.
Asthma is the most frequent chronic inflammatory obstructive airway disease in children, affecting more than 300 million people worldwide and responsible for numerous hospital admission, with up to 15% episodes requiring admission in the paediatric age group1,2 (in some cases in the paediatric intensive care unit [PICU]), with a high associated economic cost.3 When asthma exacerbations (AEs) occur, most patients improve with standard care, which includes supplemental oxygen, administration of β2 agonists and steroid therapy. Eighty percent of asthma-related deaths occur in patients with poorly controlled disease.4
Oxygen therapy with high-flow nasal cannula (HFNC) has proven to be a safe and effective technique in the management of bronchiolitis and asthma in children.5,6 It is considered an alternative to CPAP in patients with respiratory failure due to asthma or other diseases.7 Treatment with HFNC reduces the dead space, improving CO2 clearance, and produces a slight positive pressure at the end of expiration, which has also been observed in patients with asthma admitted to the PICU.8,9 Still, few studies in the literature have contributed data on the efficacy and usefulness of HFNC in the treatment AEs,6,10 and none has demonstrated its utility and safety in inpatient paediatric wards.
Although the procedure for its administration is more or less standardised, some aspects are still being debated, such as the optimal initial oxygen flow rate or the best time to deliver it, which is reflected in the variability found in the protocols employed in previously published studies. No international guidelines or publications have provided values for the optimal flow rate with which to start treatment or the maximum flow rate to use with HFNC in children admitted to the paediatric ward due to AE. Some authors estimate these values based on body weight, with flow rates ranging between 1 and 3l/kg/min, while others determine it based on the severity of the presentation, with a maximum value of 3l/kg/min. The FiO2 is usually set at 100% at the start of treatment and can be adjusted in the first few hours based on the percutaneous oxygen saturation to achieve target saturations of more than 91–93%.11
Thus, our primary objective was to analyse our experience with HFNC in the treatment of patients admitted to the paediatric ward with asthma exacerbation, and to analyse outcomes based on whether patients were treated with an initial flow rate of 15l/min versus less than 15l/min.
Patients and methodsWe conducted an observational inferential study in a retrospective cohort of children aged 4–15 years admitted to the paediatric ward due to moderate-to-severe AE. The setting was a tertiary care hospital with 38 general paediatrics beds that manages 1750 admissions per year. Asthma exacerbations were the third leading cause for admission in our hospital during the period under study.
We defined AE as an episode characterised by cough, respiratory distress and wheezing associated with bronchial hyper-responsiveness and airway obstruction of variable severity, totally or partially reversible with pharmacotherapy or with spontaneous resolution.12 The routine management of AEs conformed to the Consensus on the Treatment of Asthma in Paediatrics endorsed by the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics), the Sociedad Española de Urgencias de Pediatría (Spanish Society of Paediatric Emergency Medicine), the Sociedad Española de Neumología Pediátrica (Spanish Society of Paediatric Pulmonology), the Sociedad Española de Inmunología Clínica y Alergia Pediátrica (Spanish Society of Clinical Immunology and Paediatric Allergy) and the Sociedad Española de Pediatría Extrahospitalaria y de Atención Primaria (Spanish Society of Outpatient and Primary Care Paediatrics).13
We included all eligible patients aged 4–15 years admitted to the paediatric ward with an AE between January 2012 and December 2016 by consecutive sampling. We excluded patients outside the established age range, admitted directly to the PICU or with facial malformations or a tracheostomy precluding treatment with HFNC. The primary outcome of the study was the dichotomous variable of whether patients did or did not receive HFNC during their stay in the ward. High-flow oxygen therapy was delivered with the Fisher & Paykel MR850 humidification system. The criteria for initiation of HFNC in the paediatric ward were: progression of respiratory distress (evinced by an increase from moderate to severe in the Pulmonary Score [PS])14 or decrease in oxygen saturation (SatO2) below 91% despite administration of supplemental oxygen. The physician in charge of the patient prescribed HFNC based on these criteria and determined the initial flow rate based on the clinical condition of the patient.
The initial flow rate varied between 10 and 15l/min. In patients that did not exhibit clinical improvement with initial flow rates of less than 15l/min, the rate was increased progressively to a maximum of 15l/min. The FiO2 was adjusted to the value required to maintain an oxygen saturation of 91% or more with nasal cannulae adjusted to the weight and age to the patient. We performed an additional analysis in patients treated with HFNC. We divided these patients into 2 groups based on the initial flow rate: 15l/min and less than 15l/min. The dependent variable in this secondary analysis was the need for admission to PICU due to failure of oxygen therapy with HFNC (clinical worsening, need for more intensive monitoring or need for more advanced respiratory support). The decision to admit patients to the PICU rested with the physician in charge and was based on the progression of respiratory distress (increase relative to baseline in the PS, changing from moderate to severe, or decline in SatO2 <91%) despite optimisation of HFNC.
We collected data on clinical and epidemiological variables such as age, sex, body weight, personal history, severity (Pulmonary Score), respiratory rate (RR) and heart rate (HR) at the time of admission to the ward, of initiation of HFNC and at 3–6h of treatment. We also collected information on concomitant treatments, diagnostic tests and the need for admission to PICU or subsequent readmission. We analysed the complications associated with HFNC (ulceration, epistaxis, pneumothorax, etc.) and how patients tolerated treatment, including the need for sedation.
The statistical analysis was performed with the software SPSS version 21.0. (SPSS Inc.; Chicago, IL, USA). We summarised quantitative variables as mean and standard deviation or as median and interquartile range depending on the shape of the distribution, and qualitative variables as percentages. We used the chi square and the Fisher exact tests to compare qualitative variables, and the Mann–Whitney U test or the Kruskal Wallis test to compare quantitative variables. We used the Spearman rank correlation coefficient to assess the association between quantitative variables.
To assess the factors that could contribute to worsening and, therefore, to the need for HFNC therapy in asthma exacerbations, we fitted 2 logistic regression models. The first model only included explanatory variables corresponding to p-values of less than 0.20 in the bivariate analysis, such as age, PS, the number of visits to the emergency department in the past 3 months, the number of previous hospitalizations and passive smoking. The second model included age, PS and the number of previous hospitalizations. We have expressed the results for both models in terms of odds ratios (ORs) and 95% confidence intervals (CIs). We used the Akaike information criterion (AIC) and the Bayesian information criterion (BIC) to select and compare models. We chose the model with the lowest AIC and BIC values, which reflect a better fit (model 1).
We also fitted another logistic regression model to assess the factors that contributed to admission to the PICU. In this model the need for admission to PICU was the dependent variable, and the explanatory variables were age, PS and the initial HFNC flow rate (15l/min or <15l/min), which corresponded to p-values of less than 0.20 in the bivariate analysis.
We assessed the goodness of fit of the models with the Hosmer–Lemeshow test and Nagelkerke's R2. We ruled out collinear relations between the variables included in all the models. We defined statistical significance as a p-value of less than 0.05. The study was approved by the Ethics Board for Clinical Research (Record no. 136/17).
ResultsWe included 536 patients with a diagnosis of AE admitted in the period under study (2012–2016), of which 40 (7.5%) required HFNC therapy. In this cohort, 63% of patients were male, the median age was 5 years (IQR, 4–6) and the mean length of stay was 4 days (IQR, 3–5). The sex distribution, demographic characteristics and proportion of patients presenting with atopy at admission were similar in both groups. Patients that required HFNC had a higher RR and higher pulmonary scores at initiation of treatment (median PS, 7.5 [IQR, 6–8.7] in the HFNC group vs. 5 [4–6] in the conventional oxygen therapy group; P<.01). Furthermore, patients in the group treated with HFNC had visited the emergency department more frequently in the past 3 months (1 [0–2] vs. 0 [0–1]; P=.03), were more likely to be passive smokers, had been hospitalised more times (4 [1–6] vs. 1 [1–3]; P<.01) and were more likely to be receiving chronic treatment (Table 1).
Baseline characteristics and clinical outcomes of the group treated with HFNC and the group not treated with HFNC.
| Total sample (n=536) | HFNC (n=40) | No HFNC (n=496) | P | |
|---|---|---|---|---|
| Age | 5 (4–7) | 5 (4–6) | 5 (4–7) | .12 |
| Male sex (%) | 340/536 (63.4%) | 27/40 (67.5) | 313/496 (63.1) | .61 |
| HR | 133 (120–147) | 140 (130–146) | 133 (120–146) | .16 |
| RR | 40 (34–48) | 45 (38–56) | 40 (32–48) | .06* |
| PS | 5 (4–6) | 7.2 (6–8.7) | 5 (4–6) | <.01* |
| Emergency visits (3 months) | 0 (0–1) | 1 (0–2) | 0 (0–1) | .03* |
| Previous hospitalizations | 2 (0–4) | 4 (1–6) | 1 (1–3) | <.01* |
| Chronic treatment | 233/534 (43.6%) | 23/40 (57%) | 210/494 (42%) | .05* |
| Passive smoking | 149/375 (39.7%) | 9/40 (22.5%) | 140/335 (41%) | .02* |
| Atopy | 346/532 (65%) | 22/40 (55%) | 324/492 (65.8%) | .17 |
| Mean LOS | 4 (3–5) | 6 (4–7) | 3 (3–5) | <.01* |
| Days of O2 | 2 (1–3) | 4 (3–5.5) | 2 (1–3) | <.01* |
| MgSO4 | 29/534 (5.4%) | 15/40 (37.5%) | 14/494 (2.8%) | <.01* |
| PICU | 11/536 (2%) | 10/40 (25%) | 1/496 (0.2%) | <.01* |
| Readmission | 20/536 (3.7%) | 4/40 (10%) | 16/496 (3.2%) | .04* |
HFNC, high-flow nasal cannula oxygen therapy; HR, heart rate; LOS, length of stay; PICU, paediatric intensive care unit; PS, pulmonary score; RR, respiratory rate.
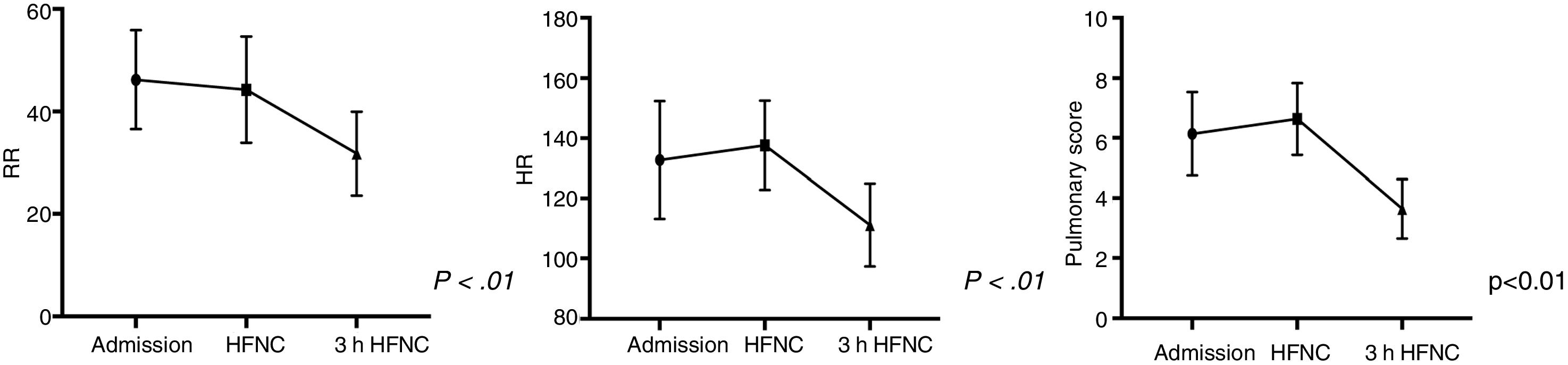
In patients with AE, treatment with HFNC was associated with significant decreases in HR, RR and the PS within 3–6h of treatment initiation (Fig. 1). Compared to patients that did not receive high-flow oxygen, patients treated with HFNC, who were more severely ill, had longer lengths of stay (6 days [4–7] vs. 3 days [3–5], P<.01), required more days of oxygen and steroid therapy, and were more likely to require administration of intravenous magnesium sulphate; in addition, a higher proportion of patients treated with HFNC were readmitted after discharge (4/40 [10%] vs. 16/496 [3.2%]; P=.04). Of the 40 patients treated with HFNC, 8 (20%) required admission to the PICU, compared to 1 of the 496 patients treated with standard oxygen therapy (0.2%) (P<.01) (Table 1).
In the HFNC group, we compared the baseline characteristics and outcomes of patients in whom treatment was initiated with a flow rate of 15l/min versus patients with lower initial flow rates. We found that a significantly smaller proportion of patients that started HFNC therapy with a flow rate of 15l/min required PICU admission, even though patients in this group had higher RRs and pulmonary scores at baseline and a higher number of asthma exacerbations in the past (Table 2).
Baseline characteristics and outcomes of patients with asthma exacerbation by oxygen flow rate at initiation of treatment with HFNC.
| Total HFNC group (n=32) | Flow rate, 15l/min (n=15) | Flow rate <15l/min (n=17) | P | |
|---|---|---|---|---|
| Age | 5 (4–6) | 4 (4–6) | 5 (4–6) | .33 |
| Male sex (%) | 21/32 (65.6%) | 11/15 (73.3%) | 10/17 (58.8%) | .47 |
| HR | 137 (126–145) | 126 (121–141) | 140 (130–145) | .27 |
| RR | 44 (38–50) | 49 (40–55) | 40 (36–48) | .09 |
| PS | 7 (6–7.7) | 7 (7–8) | 6.5 (5.7–7.2) | .07 |
| Respiratory history | 7/32 (21.8%) | 6/15 (40%) | 1/17 (5.8%) | .03* |
| Weight percentile | 42 (14–71) | 35 (13–50) | 45 (15–71) | .34 |
| Mean LOS | 6 (4–7) | 6 (4–9) | 6 (3–7) | .35 |
| Days of HFNC | 3 (1.7–4) | 3.5 (2–5.2) | 3 (2–4) | .04* |
| MgSO4 | 15/32 (46.8%) | 7/15 (46.5%) | 8/17 (47%) | .90 |
| PICU | 10/32 (31.25%) | 2/15 (13%) | 8/17 (47%) | .05* |
HFNC, high-flow nasal cannula; HR, heart rate; LOS, length of stay; PICU, paediatric intensive care unit; PS, pulmonary score; RR, respiratory rate.
In model 1, the dependent variable was the need of HFNC in the entire cohort, and the explanatory variables included in the model were those corresponding to p-values of less than 0.2 in the bivariate analysis (age, PS, number of previous hospitalizations, number of emergency visits in the past 3 months and passive smoking). In model 1, we found that the regressors that explained the highest proportions of the variance in the need for HFNC in our cohort were the PS (OR=1.38; 95% CI, 1.01–1.9; P=.03) and the number of previous hospitalizations (OR=1.2; 95% CI, 1.07–1.3; P<.01). Table 3 presents the values of Nagelkerke's R2, the AIC and the BIC for this model.
Explanatory variables in the logistic regression analysis of HFNC.
| Explanatory variables | HFNC adjusted OR (95% CI) | P |
|---|---|---|
| Age | 0.7 (0.5–1.07) | .118 |
| Pulmonary score | 1.38 (1.01–1.9) | .03* |
| Number of previous emergency visits | 1.18 (0.8–1.6) | .27 |
| Previous hospitalizations | 1.2 (1.07–1.3) | <.01* |
| Passive smoking | 0.5 (0.13–2.3) | .41 |
Model 1: Nagelkerke's R2, 0.3; AIC, 114.231; BIC, 136.5; -2LL, 102.2.
Age, the severity score and the number of emergency visits and previous hospitalizations were analysed as continuous variables, while passive smoking was a categorical variable. The asterisks mark the parameters with a statistically significant association in the adjusted analysis.
CI, confidence interval, HFNC, high-flow nasal cannula therapy; OR, odds ratio.
In model 2, the dependent variable was PICU admission. The bivariate analysis revealed that patients that required admission to the PICU had significantly higher pulmonary scores at admission compared to the group that was not admitted to the PICU (9 [7–9] vs. 5 [4–6]; P<.01), and that a significantly greater proportion of patients that started HFNC therapy with flow rates of less than <15l/min were admitted to the PICU compared to patients that started treatment with a flow rate of 15l/min (8/17 [47%] vs. 2/15 [13%]; P=.05) (Table 2). Thus, we included these 2 variables in addition to age in the logistic regression model. In this model, the covariates that explained the highest proportion of the variance in PICU admission in our cohort were the PS (OR=4.5 [95% CI: 1.2–1.7], P=.02) and a flow rate of less than 15l/min at initiation of treatment (OR=0.4 [95% CI, 0.2–0.98], P=.04) (Table 4). Table 4 presents the values of Nagelkerke's R2, the AIC and the BIC for this model.
Explanatory variables in the logistic regression analysis of PICU admission.
| Covariables | PICU admission, adjusted OR (95% CI) | P |
|---|---|---|
| Age | 2.71 (1.05–7.03) | .04* |
| Pulmonary score | 4.5 (1.2–17) | .02* |
| HFNC flow rate (<15l/min/15) | 0.4 (0.2–0.98) | .04* |
Model 2: Nagelkerke's R2, 0.65; AIC, 22; BIC, 27.3; -2LL, 14.
The age and severity score were treated as continuous variables, while the flow rate of HFNC was a categorical variable. The asterisks mark the parameters with a statistically significant association in the adjusted analysis.
CI, confidence interval, HFNC, high-flow nasal cannula therapy; OR, odds ratio; PICU, paediatric intensive care unit.
Treatment with HFNC was well tolerated. None of the patients required sedation. There were no complications associated with the use of HFNC, such as pneumothorax or ulceration, save for nasal irritation in a few cases.
DiscussionOur study is the first to describe the use of HFNC for treatment of moderate to severe asthma exacerbation in the paediatric ward setting. Of all patients admitted to the ward with AEs, 7.5% had worsening respiratory symptoms that indicated treatment with this modality of support. The use of HFNC achieved a decreased in RR, HR and PS in the first hours of treatment, associated with clinical improvement in the patient. Of all patients treated with HFNC, only 20% required admission to the PICU, which is indicative of a substantial clinical impact.
In our cohort, the strongest predictors of clinical worsening and therefore of need of HFNC therapy were the PS at admission and the number of previous hospitalizations. Thus, our study identified a subset of patients at higher risk of progressing to severe disease during AEs and more likely to require HFNC therapy, which is relevant for clinical practice, as this subset of patients could benefit from closer monitoring in the first hours of hospitalisation and early initiation of support with HFNC.8 Similarly, some authors have tried to identify criteria to define clinical worsening and for PICU admission in patients with AE: a history of 3 or more emergency department visits in the previous year, an elevated IgE level, or an oxygen saturation of less than 91% on presentation or in the course of the exacerbation.15 Other studies conducted in the PICU setting have attempted to define the subset that could most benefit from HFNC, evincing that it would be very useful to establish an algorithm or clinical criteria (such as wheezing, work of breathing, airflow or oxygen saturation) to predict the severity of exacerbations, and therefore the need of HFNC.16
Oxygen delivery through HFNC has developed and become widely used in recent years, and has been shown to improve respiratory distress and oxygen saturation by increasing mucociliary clearance, washout of the nasopharyngeal dead space and oxygen delivery to the lungs while producing some positive airway pressure17; another salient finding is the increased comfort associated with this modality, assessed by means of the CONFORT scale in the PICU setting.18 It is important to take into account that the use of HFNC requires extensive experience in the management of respiratory disease in children, adequate monitoring and a high-enough nurse-to-patient ratio.17
We found a significant decrease in HR, RR and the PS within 3h of treatment with HFNC, which was consistent with the findings of other authors that investigated the use of this modality for treatment of patients with AEs. This improvement in respiratory parameters is usually observed within 60–90min6 and persists through the following 8–12h,4 an effect that has been previously demonstrated in patients with bronchiolitis and asthma.5
Compared to CPAP, which can be less comfortable and require sedation in some case,19,20 HFNC is better tolerated, more comfortable and less noisy and does not cause nasal deformities.8,17,21,22 We found no adverse events, problems with tolerability or discomfort associated with the use of this modality of oxygen delivery in our cohort. There is evidence from multicentre randomised trials that HFNC is associated with a lower mortality at 90 days compared to NIV or standard oxygen.23 Other studies have found lower intubation rates in patients with hypoxaemia treated with HFNC (although these studies tended to use higher flow rates).24 High-flow oxygen therapy has also been shown to improve patient comfort and decrease the severity of dyspnoea and the RR, and is associated with an increased survival.23,25 In contrast, a retrospective study in the PICU setting in 42 children with AEs that compared HFNC with NIV found that while HFNC may be useful in the PICU, it can delay initiation of NIV (a modality that did not fail in any of the patients) in up to 40% of severely ill patients. The multivariate logistic regression model showed that HFNC was unlikely to fail in patients with a HR of less than 146 beats per minute and a RR of less than 55 breaths per minute, which highlights the need for caution in using HFNC and to not delay initiation of other supportive measures if there is no improvement.26
Previous observational studies have described a significant decrease in the proportion of infants with severe bronchiolitis admitted to the PICU after the introduction of HFNC in inpatient wards. Thus, in 2013 González et al.5 reported a 62% reduction in the relative risk of PICU admission in infants with bronchiolitis treated with HFNC. Similarly, in 2014 Mayfield et al.27 reported that patients with bronchiolitis treated with HFNC in the ward were 4 times less likely to need admission to PICU compared to patients treated with conventional oxygen therapy (OR, 4.086; 95% CI, 1.0–8.2; P=.043).
When we analysed the initial flow rate used in HFNC therapy, we found that patients with a higher PS at admission and those in whom HFNC was initiated with flow rates of less than 15l/min were more likely to be admitted to the PICU compared to patients treated with an initial flow rate of 15l/min, a rate that was thus associated with a lower proportion of treatment failure. This suggests that initiating HFNC therapy with higher flow rates could prevent a greater number of PICU admissions, although prospective randomised trials are needed to confirm this hypothesis.
There are limitations to our study, such as its retrospective, observational design and its performance in a single hospital, which may limit its external validity. Furthermore, the initial flow rate used in HFNC therapy was left to the discretion of the physician in charge of the patient. The sample size was small, so data from prospective, randomised multicentre studies is needed to confirm our findings. Further research is also needed to determine the optimal timing for initiation of HFNC, parameters for the early identification of at-risk patients, the optimal modality of ventilatory support and the optimal duration of treatment. Another important aspect worth investigating is the possible usefulness of HFNC in the interhospital or intrahospital transport of patients.17
In conclusion, HFNC therapy can be useful in the management of asthma exacerbations in the paediatric ward. Patients with higher severity scores and a greater number of previous hospitalizations constitute a risk subgroup that could benefit from this modality of respiratory support, so we propose closer monitoring of these patients from the moment they are admitted to the ward.
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank the nursing staff and participating patients and their families.
Please cite this article as: González Martínez F, González Sánchez MI, Toledo del Castillo B, Pérez Moreno J, Medina Muñoz M, Rodríguez Jiménez C, et al. Tratamiento con oxigenoterapia de alto flujo en las crisis asmáticas en la planta de hospitalización de pediatría: nuestra experiencia. An Pediatr (Barc). 2019;90:72–78.
