

Developmental dysplasia of the hip (DDH) refers to the spectrum of abnormalities of maturation and development of the hip. Breech presentation is associated with DDH. This risk factor can be modified by external cephalic version (ECV). The aim of this study is to evaluate the incidence of DDH in patients who successfully underwent ECV, as well as to evaluate need for these children (breech for a period during gestation) to be included in the DDH screening protocol.
Material and methodsA prospective cohort study was conducted in the Hospital Universitario de Vigo from January 1, 2015 to December 31, 2015. It included children born in cephalic presentation after a successful ECV, as well as children born in breech presentation. They all were screened for DDH by ultrasound examination of the hip.
ResultsOut of a total of 122 newborns included in the study, ECV was attempted on 67 (54.9%), of which 35 (52.2%) were successful. Out of the 14 children diagnosed with DDH, 3 of those born in cephalic presentation after a successful ECV were found to be normal on physical examination.
ConclusionsSuccessful ECV is associated with a lower incidence of DDH as regards breech presentation. However, these patients should be included in the DDH screening protocol for the early detection of this disorder.
La displasia del desarrollo de la cadera (DDC) engloba un espectro de anomalías que afecta a la maduración y desarrollo de la cadera. La presentación podálica es uno de los factores de riesgo asociado a esta patología y puede ser modificada en las últimas semanas de gestación mediante la versión cefálica externa (VCE). El objetivo de nuestro trabajo es determinar la incidencia de DDC en pacientes sometidos a una VCE exitosa, así como valorar la necesidad de incluir a estos niños (podálicos durante gran parte de la gestación) en el protocolo de cribado de DDC.
Material y métodosEstudio de cohortes prospectivo realizado en el Hospital Universitario de Vigo entre el 1 de enero y el 31 de diciembre del 2015. Participaron niños sometidos a VCE y niños podálicos no sometidos a VCE. A todos ellos se les realizó una ecografía de cadera para estudiar la incidencia de DDC en ambos grupos.
ResultadosSe incluyeron un total de 122 pacientes. Se intentó realizar VCE en 67 (54,9%) siendo exitosa en 35 (52,2%). De los 122 niños: 14 fueron diagnosticados de DDC mediante ecografía. Tres (8,5%) de los niños con DDC nacieron en presentación cefálica tras VCE exitosa con exploración física de caderas normal al nacimiento.
ConclusionesLa VCE reduce el riesgo de DDC con respecto a la presentación podálica pero de no incluir a los niños versionados con éxito en el protocolo de cribado de DDC, corremos el riesgo de no detectar precozmente esta patología.
Developmental dysplasia of the hip (DDH) is a spectrum of anomalies that affect the maturation of the hip in the newborn in which the femoral head and acetabulum have an abnormal relationship and development. In the first weeks of life, newborns may have a physiological laxity in the hip joint and immaturity of the acetabulum that resolves spontaneously and with no sequelae.1 However, uncorrected DDH is associated with significant long-term comorbidities, such as gait abnormalities, chronic pain or degenerative disease of the coxofemoral joint.1,2 Certain factors, such as female sex, first-born status, breach presentation (after 34 weeks’ gestation), reduced foetal movement, oligohydramnios or a positive family history of DDH increase the risk of this disease.3
Every risk factor for this disease is non-modifiable, except for the presentation of the foetus at birth. External cephalic version (ECV) aims at decreasing the frequency of caesarean sections performed due to breech presentation, thus reducing the maternal and child morbidity and mortality associated with this type of delivery.4 External cephalic version is a relatively easy, safe and inexpensive manoeuvre. After sedating the mother, the obstetrician externally manipulates the foetus by exerting mild pressure on the abdominal wall of the mother to shorten the foetal long axis and achieve its full rotation.4,5 To guarantee the safety of the foetus, the foetal heart rate is monitored throughout the procedure.
In the first days of life, the paediatrician carries out a comprehensive and thorough physical examination of the child that includes an assessment of the hip joints. A meticulous examination is essential, and especial attention should be paid to the examination of the hip in patients with risk factors for DDH. It is important to remember that the earlier the diagnosis is made, the easier and more effective the treatment will be, and the better the final outcome.6–8 In Spain, imaging tests are not performed routinely. An ultrasound scan of the hip is performed in patients with abnormal findings on physical examination or who have 2 or more risk factors (female sex, breach presentation at birth and/or history of DDH in first-degree relative).9 In patients with normal findings in the physical examination, the best time to do the ultrasound scan is 6 weeks after birth, when the hip is sufficiently mature to avoid false positives yet plastic enough for conservative treatment to be successful.
External cephalic version changes the presentation of foetuses that have been in a breech position during part of the pregnancy in the last weeks of gestation. However, since these children are finally delivered head-first, they are not considered at risk of DDH and are not included in the current protocol. The aim of our study was to determine the incidence of DDH in patients successfully turned with ECV and assess whether the current protocol should be changed to include patients that were turned successfully, considering them as breech for the purposes of screening.
Materials and methodsWe conducted a retrospective cohort study between January 1 and December 31, 2015. We included children born in our hospital that had undergone successful ECV in the last trimester of gestation, and children that were not turned or in who ECV was unsuccessful and had a breech birth as controls. All children underwent an ultrasound scan of the hip at 6 weeks post birth to analyse the incidence of DDH in either group. All parents of the children included in the study were informed about it and signed their consent for participation.
ResultsThe study included a total of 122 patients, 68 (55%) female and 54 (44%) male, with gestational ages ranging between 34 and 41 weeks. They were all products of singleton pregnancies, 108 (89%) born to term and 81 (66%) with first-born status. As for the mode of delivery, 94 (77%) were born by caesarean section (86 due to breach presentation, 4 to prolonged labour, 3 to abnormalities in the ECG tracings and 1 to cephalopelvic disproportion), and 28 (23%) by normal or instrumental vaginal delivery. Prenatal ultrasound examination found evidence of intrauterine growth restriction in 8 (6.6%), macrosomia in 8 (6.6%), oligohydramnios in 3 (2.5) and renal abnormalities in 3 (2.5%). Nearly 10% of the mothers had a history of gestational diabetes or hypothyroidism. Ten patients had a family history of DDH, 7 of them in a first-degree relative (mother).
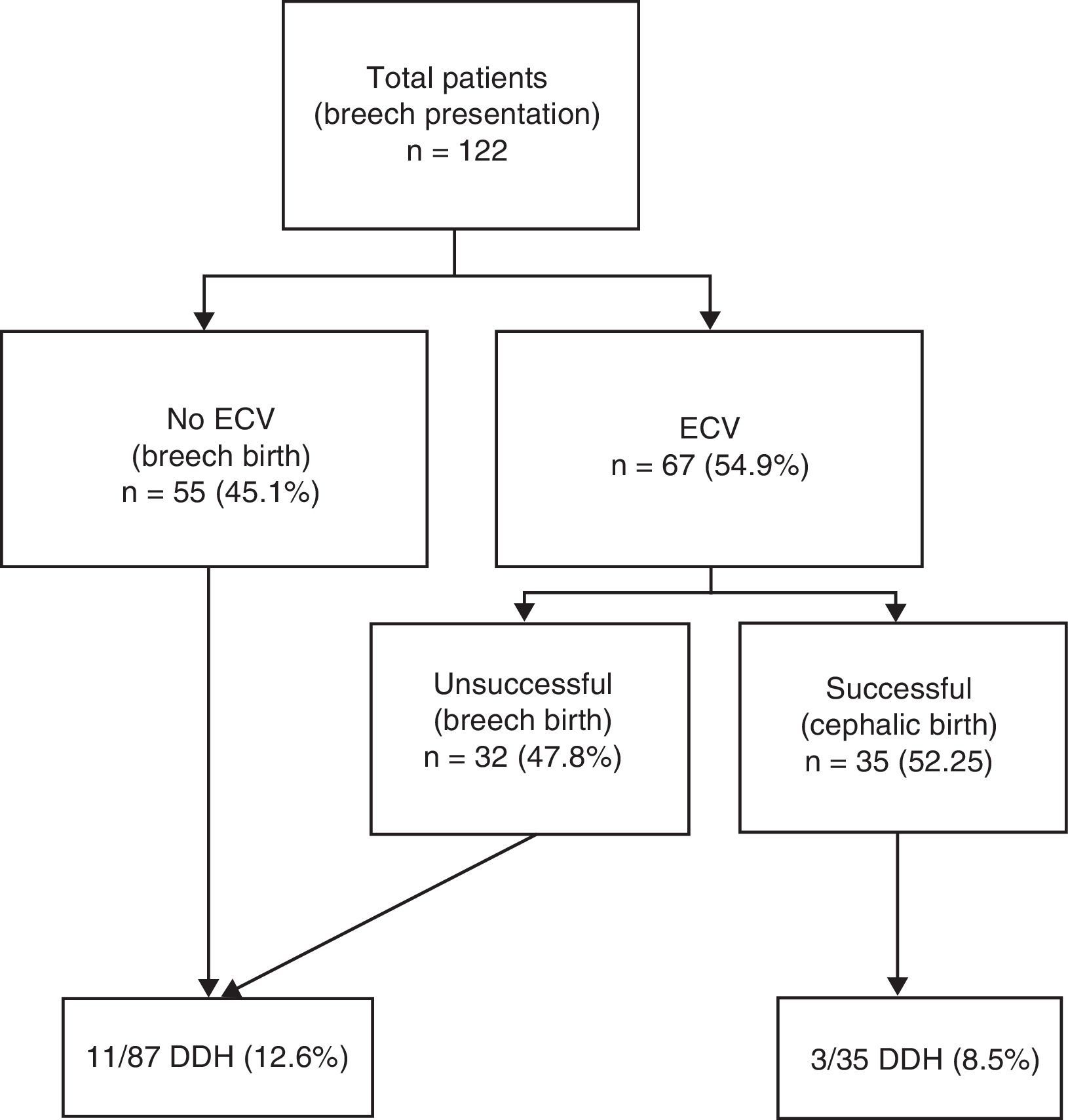
External cephalic version was attempted in 67 patients (55%) between weeks 36 and 40 of gestation. It was successful in 35 cases (52.2% success rate) and failed in 32 (47.8%). Of the 35 patients that were turned, 28 were born in a normal vaginal delivery and 7 by caesarean section (4 due to prolonged labour, 2 to risk of foetal distress, 1 to cephalopelvic disproportion).
Ultrasound examination of the hip detected DDH in 14 patients: 11 who had not been turned and were born breech (ECV had been attempted and unsuccessful in 6) and 3 successfully turned and born with a cephalic presentation (2 female foetuses turned at 38 weeks’ gestation and 1 male foetus turned at 37 weeks’ gestation). Fig. 1 presents a flowchart with the number of patients included in each group under study with the corresponding percentages of DDH.
The characteristics of the 14 infants with DDH confirmed by ultrasound were the following: 9 were female and 5 male, 11 were first-born children, 2 were large for gestational age, 3 had a history of DDH in first-degree relatives, 1 had associated torticollis and 1 had a history of intrauterine growth restriction. The physical examination had been abnormal in 5 and normal in the remaining 9 (including the 3 patients in whom ECV was successful). We ought to note that in one patient, the physical examination was abnormal but the ultrasound scan found no evidence of DDH.
There were different reasons for ordering an ultrasound scan of the hip in the 14 patients with DDH. Six met the criteria established in the current DDH screening protocol of our hospital, 5 had abnormal findings in the physical examination, and in the remaining 3, the scan was ordered with the objective pursued in this study: to determine the incidence of DDH in infants in whom ECV had been successful with a normal physical examination and no other risk factors.
DiscussionDevelopmental dysplasia of the hip is a disease that requires early diagnosis and treatment on account of the significant consequences that result from delays in treatment. This disease has been associated with various risk factors, including female sex, first-born status, breech presentation after 34 weeks’ gestation, oligohydramnios or a history of DDH in first-degree relatives. In our study, we found evidence of the association of DDH with female sex, breech presentation and positive family history. The disease was also associated with other causes of a reduced intrauterine space that have an impact on hip development in addition to breech presentation, such as macrosomia or oligohydramnios.
In recent years, there have been changes in the practice of obstetrics. Caesarean section is becoming the routine mode of delivery in breech births, as it is associated with a reduction in perinatal mortality.10 The introduction of ECV has succeeded in reducing the number of foetuses with a breech presentation and therefore the frequency of caesarean delivery and its associated risks. However, there are very few studies that assess its impact in relation to DDH.11 The modification of the foetal presentation is beneficial for both mother and child, but we need to investigate its potential impact on the newborn's hip. Two methods are currently available for the early diagnosis of this disease: routine physical examination and routine ultrasound examination in children with 2 or more risk factors. This raises the question whether an ultrasound examination should be ordered in infants whose physical examination is normal and who do not strictly meet the criterion of breech birth because they were born in a normal vaginal delivery following successful ECV. Considering the pathophysiology of DDH, it would be reasonable to hypothesise that these children are at lower risk of DDH compared to children who are in a breech position until birth, and that this risk would decrease the longer the time elapsed between ECV and delivery. In any case, it would also be logical to assume that having temporarily been in a breech position would increase the likelihood of DDH in these children compared to children with a strictly cephalic presentation.
The overall incidence of this disease in Spain is 4.3%, based on data from two studies that included 40,243 newborns.12,13 To date, no studies have assessed the impact of ECV on DDH in Spanish children. However, a study conducted in the Netherlands found a prevalence of DDH of 2.8% in children that had a cephalic birth after successful ECV.11
In our study, there were 35 children that had been turned in utero and had cephalic births and a normal neonatal physical examination. They all underwent ultrasound examination (outside of the current protocol), which detected DDH in 3 (8.5%). If we had not included these children in the DDH screening protocol, their diagnosis and treatment would have been delayed, probably until they started walking, at which point DDH would have had irreversible consequences. Therefore, we should reassess whether we should not consider infants in whom ECV was successful breech for the purpose of DDH screening. Successful ECV offers significant advantages. From a clinical standpoint, it prevents the morbidity associated with surgical intervention (caesarean section), and from an economic standpoint, it decreases the mean length of stay following birth (2 days for normal vaginal delivery vs 4–5 days for caesarean delivery). However, while ECV reduces the risk of DDH associated with breech presentation, there is a risk that DDH will go undetected in children successfully turned with ECV if they are excluded in the screening protocol.
As for the limitations of our study, we ought to highlight that the sample size was small, resulting in a reduced power to find statistically significant results. We need to continue this line of research in order to find significant results that can be applied to clinical practice.
The results of our study supported our working hypothesis: foetuses who were in the breech position during gestation and successfully turned to the cephalic position have a risk of developing DDH that, while lower than that of those with a breech presentation at birth, is still significant, and therefore should not be excluded from DDH screening. Thus, we should continue investigating the association between DDH and this risk factor. Furthermore, or results evinced the need of forming multidisciplinary teams where obstetricians, paediatricians and paediatric radiologists could work collaboratively with the purpose of adapting advances in the field of obstetrics to the field of paediatrics.
Conflict of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Sarmiento Carrera N, González Colmenero E, Vázquez Castelo JL, Concheiro Guisán A, Couceiro Naveira E, Fernández Lorenzo JR. Riesgo de displasia del desarrollo de la cadera en pacientes sometidos a versión cefálica externa. An Pediatr (Barc). 2018;88:136–139.
