



Congenital haemangiomas are benign vascular tumours that are fully formed at birth. There are 3 subtypes: rapidly involuting congenital haemangioma (RICH), partially involuting congenital haemangioma (PICH) and non-involuting congenital haemangioma (NICH). Unlike infantile haemangiomas, they do not progress after birth and they are GLUT-1 negative.1
We present the case of a term newborn with an unremarkable history who at birth had a purplish mass in the middle phalanx of the middle finger of the right hand measuring 2 cm and with telangiectasias on the surface (Fig. 1).

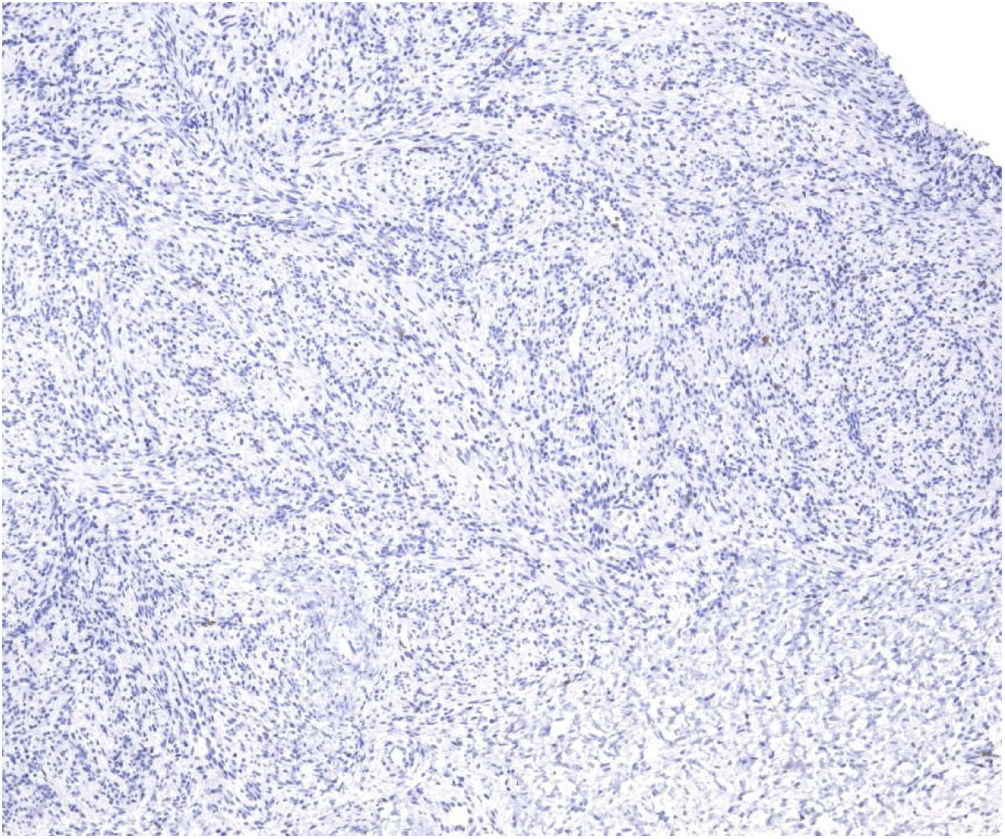
The ultrasound scan showed a heterogenous hypoechoic mass with profuse vascularization. The histological examination revealed spindle-cell proliferation in the dermis, with a storiform pattern around endothelial vessels, and the GLUT-1 stain was negative (Fig. 2).
There were no complications during the delivery, and the complete blood count was normal. At age 9 months, the lesion had involuted significantly, which confirmed the diagnosis of RICH (Fig. 3).

Due to their favourable prognosis with complete involution, RICH rarely require treatment. However, cases manifesting with transient coagulopathy and thrombocytopenia have been described in newborns with large RICHs (>5 cm).2
Diagnostic tests are useful to establish the diagnosis and rule out other possible conditions, such as vascular tumours with an intermediate risk of malignancy (kaposiform and retiform haemangioendothelioma, tufted angioma) and other benign and malignant congenital tumours. Doppler ultrasound is indicated (a vascular MRI may be needed in some cases), as is a skin biopsy, to be performed at hospital, as it causes minimal complications and offers a high diagnostic and prognostic yield.
