








The consumption of nutritional and protein supplements by adolescents may have important consequences for their health.
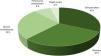
MethodsProspective observational study based on a survey of adolescents enrolled in 6 schools selected at random in the city of Seville. Our primary objective was to determine the actual consumption of dietary supplements in the adolescent population and quantifying their protein content.
ResultsWe obtained a total of 263 valid responses that showed a prevalence of consumption of nutritional supplements of any kind of 19.01%, of which 56.0% (10.64% of the total) corresponded to adolescents that consumed protein supplements for a mean protein intake of 0.26 g/kg/day (SD, 0.18). The profile of consumers of any type of supplements differed from that of nonconsumers in age, use of long-term medication and weight loss or high-protein diets. The comparison of adolescents who consumed protein supplements versus nonprotein supplements only evinced a significant difference in the control of supplement consumption. Although most of these adolescents were not subject to external control, 25.92% of those who consumed protein supplements were monitored by a professional, compared to 7.38% of consumers of nonprotein supplements. In the group that consumed protein supplements, 85.18% of adolescents achieved the desired effect and 18.51% reported some form of negative effect.
ConclusionsThe prevalence of protein supplement consumption among adolescents in our area is 10.64%, with consumption of amounts corresponding to 25% of the recommended daily allowance of protein. The profile of protein supplement consumers is very similar to that of nonprotein supplement consumers.
El consumo de suplementos nutricionales y proteicos por adolescentes puede tener importantes repercusiones para su salud.
Material y métodoEstudio prospectivo observacional, basado en una encuesta, dirigido a los adolescentes de 6 colegios, seleccionados aleatoriamente, de la ciudad de Sevilla. Nuestro objetivo principal es conocer el consumo real de suplementos alimentarios entre la población adolescente, cuantificando su contenido proteico.
ResultadosSe obtuvieron 263 respuestas válidas, objetivando una prevalencia de consumo del 19.01% para todos los suplementos nutricionales, de ellos el 56.0% consumían suplementos de proteínas (10.64% del total), con un consumo medio de proteínas de 0.26 ± 0.18 gr/kg/día. El perfil de consumidor de cualquier tipo de suplementos se diferencia de los no consumidores en la edad, uso de medicación habitual y realizar dieta para perder peso o hiperproteica. Al comparar los adolescentes que consumían suplementos proteicos con no proteicos, la única diferencia significativa estuvo en el control del consumo. Aunque la mayoría no tienen control externo, en el 25.92 % de los que consumían proteínas el seguimiento lo hacía un profesional, frente al 7.38 % de los que consumían suplementos no proteicos. El 85.18% de los consumidores de suplementos proteicos consiguió el efecto buscado, y el 18.51% refirió algún efecto negativo.
ConclusionesLa prevalencia de consumo de suplementos proteicos entre los adolescentes de nuestro medio es del 10.64%, en cantidades que suponen el 25 % de las proteínas que deben ingerir diariamente. El perfil de consumidor de suplementos proteicos es muy similar al consumidor de suplementos no proteicos.
The European Food Safety Authority defines food supplements as concentrated sources of nutrients or other substances with a nutritional or physiological effect, whose purpose is to supplement a normal diet.1,2 As the Agencia Española de Seguridad Alimentaria y Nutrición (Spanish Agency of Food Safety and Nutrition) states, it is important that food supplements not to be used to replace a healthy diet.3 Most adolescents who follow a balanced diet do not need supplements, and their unjustified use without medical guidance can pose health risks.4 Recent evidence shows that athletic performance in adolescents is more likely to improve through adequate nutrition and regular training than with supplementation.5
In adolescents who are not athletic, the dietary reference intake for protein ranges from 0.85 to 0.95 g/kg/day,6 but the practice of high-intensity sports increases the energy intake requirements. Although establishing individual energy requirements in athletic adolescents is complicated, some authors have estimated daily expenditures 3640 kcal/day for males and 3100 in females.7 The daily protein requirement of an adolescent athlete is of approximately 1.5 g of protein per kilogram of body weight, as long as the total energy requirements are met,8 and it is recommended that that the intake saturated fats not account for more than 10% of the total energy intake.9
Adolescence is a period characterised by physiological and psychological changes in addition to physical growth, and it is important to prevent imbalances between the diet, physical activity and body image leading to pathological eating behaviours. A recent systematic review and meta-analysis found that universal eating disorder prevention interventions were found to be effective in improving children’s body esteem, self-esteem, and internalization of appearance ideals.10
There have been studies attempting to determine the prevalence of food supplement consumption, consumption habits, types of supplementation and factors associated with their use in the adolescent population, with the reported prevalence of consumption ranging from 69%11 to 97%.12 The most frequently consumed supplements are multimineral and multivitamin supplements, sports drinks, caffeine, protein powder and iron supplements, and the more frequent reasons for their consumption are facilitating recovery, health maintenance and increasing energy.11–13
In the specific case of protein supplements in adolescence, few studies have been published on the subject, and there is little evidence on the magnitude of their consumption.14 Numerous types of protein can be found in protein supplements, but the ones recommended by the Sociedad Española de Medicina del Deporte (Spanish Society of Sports Medicine) are those based on casein, whey and hydrolysed protein.15
Food supplements can cause complications, and 8%–9% of consumers experience adverse effects, most frequently gastrointestinal symptoms and headache, although more severe events have also been described, such as hepatotoxicity, drug interactions and neurologic disturbances.2 In the specific case of protein supplements, a recent systematic review found an association between their use and the development of acne and changes in the microbiota, in addition to warning that the chronic use of whey protein is much more harmful, with the kidneys and liver being most affected. All these adverse effects are aggravated if the consumption of protein supplements is combined with a sedentary lifestyle.16 Although a high protein intake in childhood may contribute to an increased risk of future obesity, this association has not been found in adolescents.17,18
Furthermore, the composition of supplements may not exactly match the description in the label. Labelling is frequently fraudulent, with inaccurate amounts and omission of substances contained in the product, which results in a high risk of consuming amounts exceeding the recommended threshold or substances that are not featured in the label.19
A compounding problem is that these products are frequently advertised and sold through the internet, without any form of restriction and without warning of the risks that may be associated with their use.20
With the primary objective of understanding current trends in supplement consumption in adolescents in our region, we developed and conducted a survey to determine the prevalence and habits of supplement consumption, analyse the association between the use of protein supplements and dietary habits, assess adverse events and identify potential preventive measures.
Material and methodsAfter obtaining the approval of the Clinical Research Ethics Committee of the Área Sur health district of Seville (external file 2636-N-21, internal file 2164-N-22), we conducted a prospective observational study in March and April 2023 through an online survey aimed at adolescents aged 12–18 years enrolled in secondary schools in the city of Seville.
To calculate the sample size, we needed to know the size of the population of adolescents in Seville and the estimated prevalence of supplement consumption. We obtained the number of students enrolled in secondary schools from the Statistics Yearbook of the City Council of Seville, which was 44,732 in total. As for the prevalence of supplement consumption in youth in our region, a previous study with a response rate of 31.42% found that 21.68% of respondents used some form of dietary supplement.21 Based on these data, for a 95% level of confidence and a precision of 5%, we calculated a minimum sample size of 253, and given an expected loss of 68%, that we needed to invite a minimum of 792 adolescents to participate.
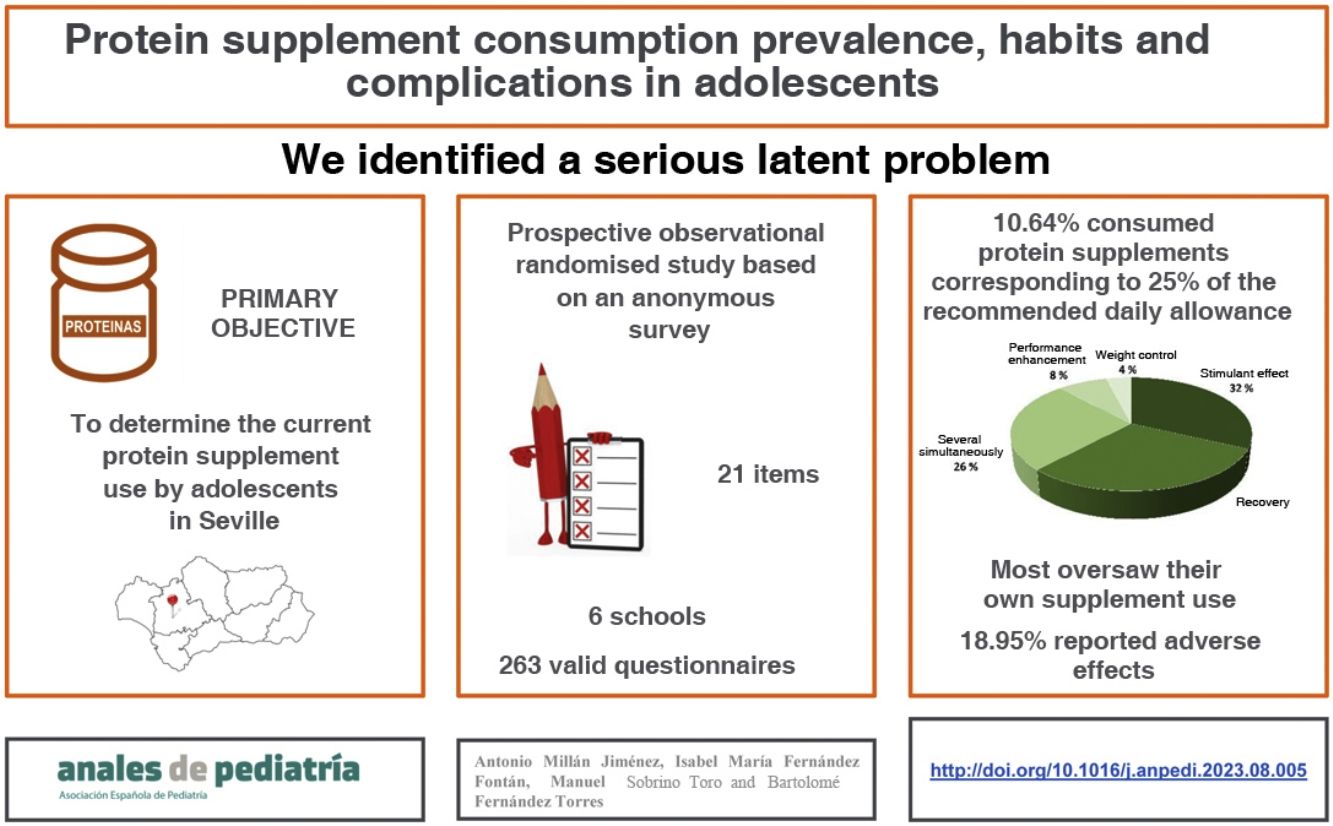
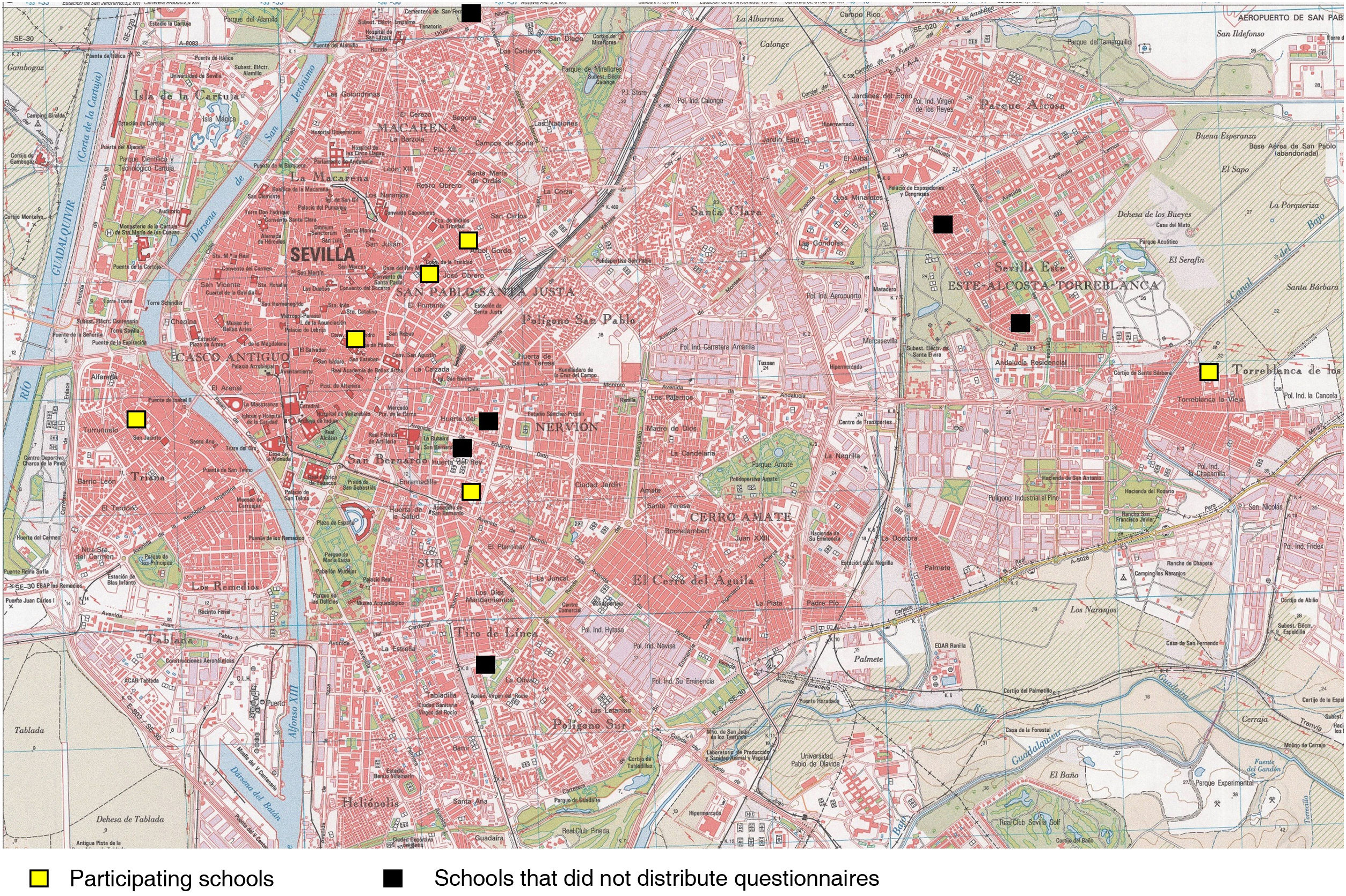
To identify schools through which to distribute the questionnaire, the first step was to use the search tool of the Department of Education of the Government of Andalusia, identifying all schools offering secondary education cycles (ESO/bachillerato) in the city of Seville. The definitive list included 71 public, private and publicly funded private schools (Appendix A). Taking into account the student-to-school ratio, we decided to include 12 schools in the survey. The schools were selected at random with the Mersenne Twister algorithm for generation of random numbers integrated in Microsoft Excel.
The questionnaire (Appendix A) comprised 21 items, was preceded by an introductory text, and included a link to contact the authors by electronic mail. The completion of the first item was required for inclusion, since it entailed informed consent, which adolescents provided with the prior knowledge and authorization of the governing board of each participating school, which included parents, students, teachers and administrative and service staff. The study variables can be classified into 4 categories: (1) characteristics of the population under study, (2) classification of dietary supplements, (3) factors associated with the consumption of protein supplements, and (4) other factors, such as prescription and monitoring by a specialist.
We attempted to contact schools in person, requesting an interview with the principal. If this was not possible, as an alternative, we requested the collaboration of the school by electronic mail. If a response was not received within 10 days, a reminder email was sent, and if there was no response within 20 days from the initial contact, the school was eliminated from the pool of candidates.
Once the schools had agreed to participate, we distributed the questionnaire to the students. We formatted the questionnaire as an online form with the Google Forms platform and provided access to it through a QR code with a link that made the questionnaire available for 14 days for adolescents in each school. The statistical analysis was conducted with the software SPSS version 25.0, using the χ2 and Student t tests, analysis of variance (ANOVA) and logistic regression, defining statistical significance as a P value of less than 0.05.
All the data were handled confidentially in adherence with the Organic Law 3/2018 on the Protection of Personal Data and the Guarantee of Digital Rights.
ResultsOf the 12 schools that we reached out to, only 6, all of them public, agreed to participate, and we obtained 263 valid responses (Figs. 1 and 2). Of the total participants, 52.47% were male and 44.11% female. The mean age was 14.82 years (standard deviation [SD], 1.58), the mean body mass index (BMI) 20.42 kg/m2 (SD, 3.48), and 8.37% received long-term medication. Most (66.16%) reported a balanced diet and 46.39% practicing sports 3–4 times a week. None reported being a professional athlete. Only 50 (19.01%) had used supplements in the previous 2 years. Table 1 summarises the characteristics of the study sample.
General characteristics of the sample.
| n | |
|---|---|
| Sex | |
| Male | 138 (52.47%) |
| Female | 116 (44.11%) |
| Declined to answer | 9 (3.42%) |
| Chronic medication | |
| No | 241 (91.63%) |
| Yes | 22 (8.37%) |
| Athletic activity | |
| 5−7 days/week | 68 (25.86%) |
| 3−4 days/week | 122 (46.39%) |
| 1−2 days/week | 73 (27.76%) |
| Usual diet | |
| Balanced | 174 (66.16%) |
| High-protein diet | 28 (10.65%) |
| Selective diet | 51 (19.39%) |
| Weight loss diet | 10 (3.8%) |
| Supplement consumption recommended | |
| Yes | 67 (25.48%) |
| No | 196 (74.52%) |
| Supplement consumption (past 2 years) | |
| Yes | 50 (19.01%) |
| No | 213 (80.99%) |
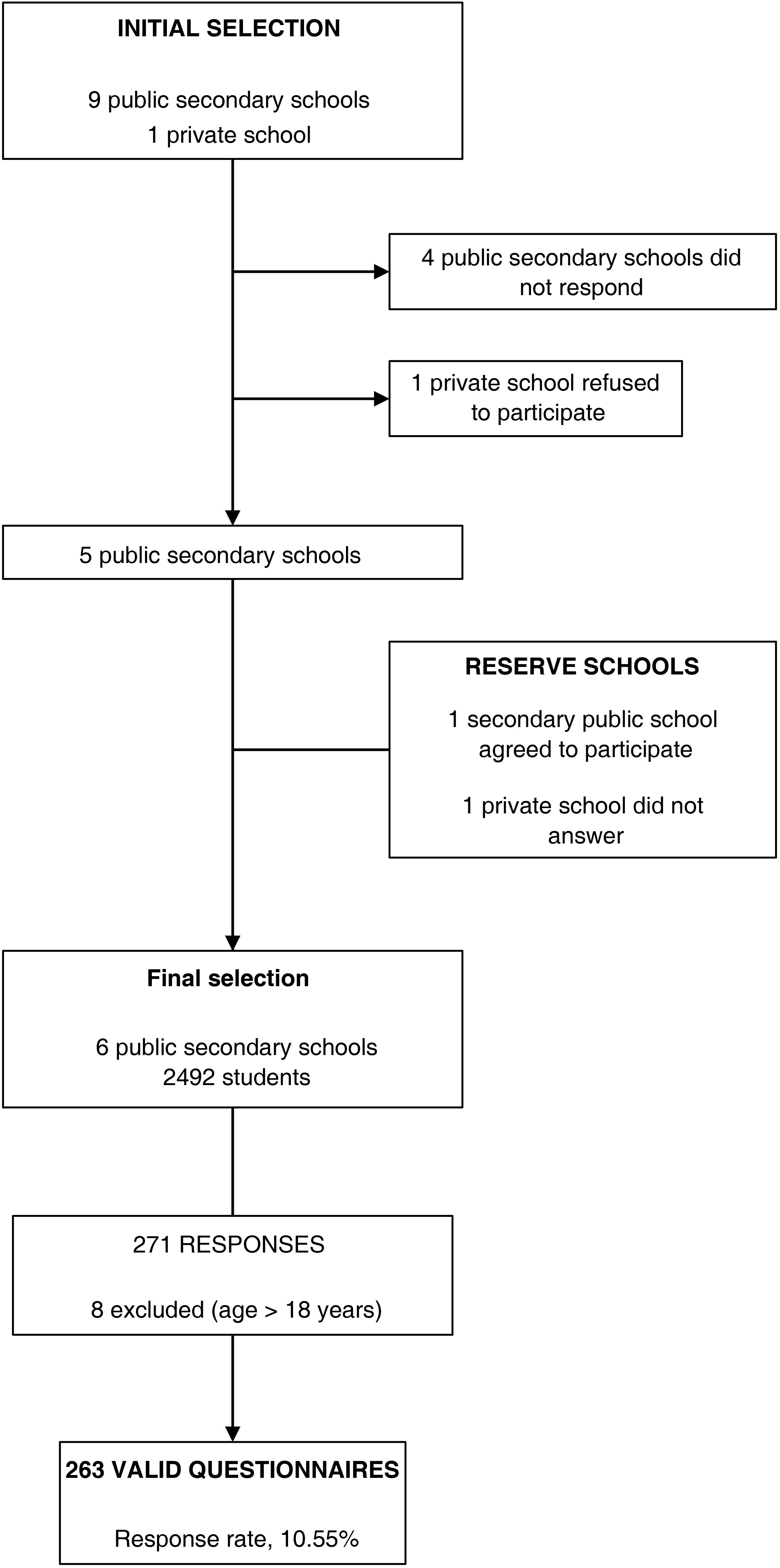
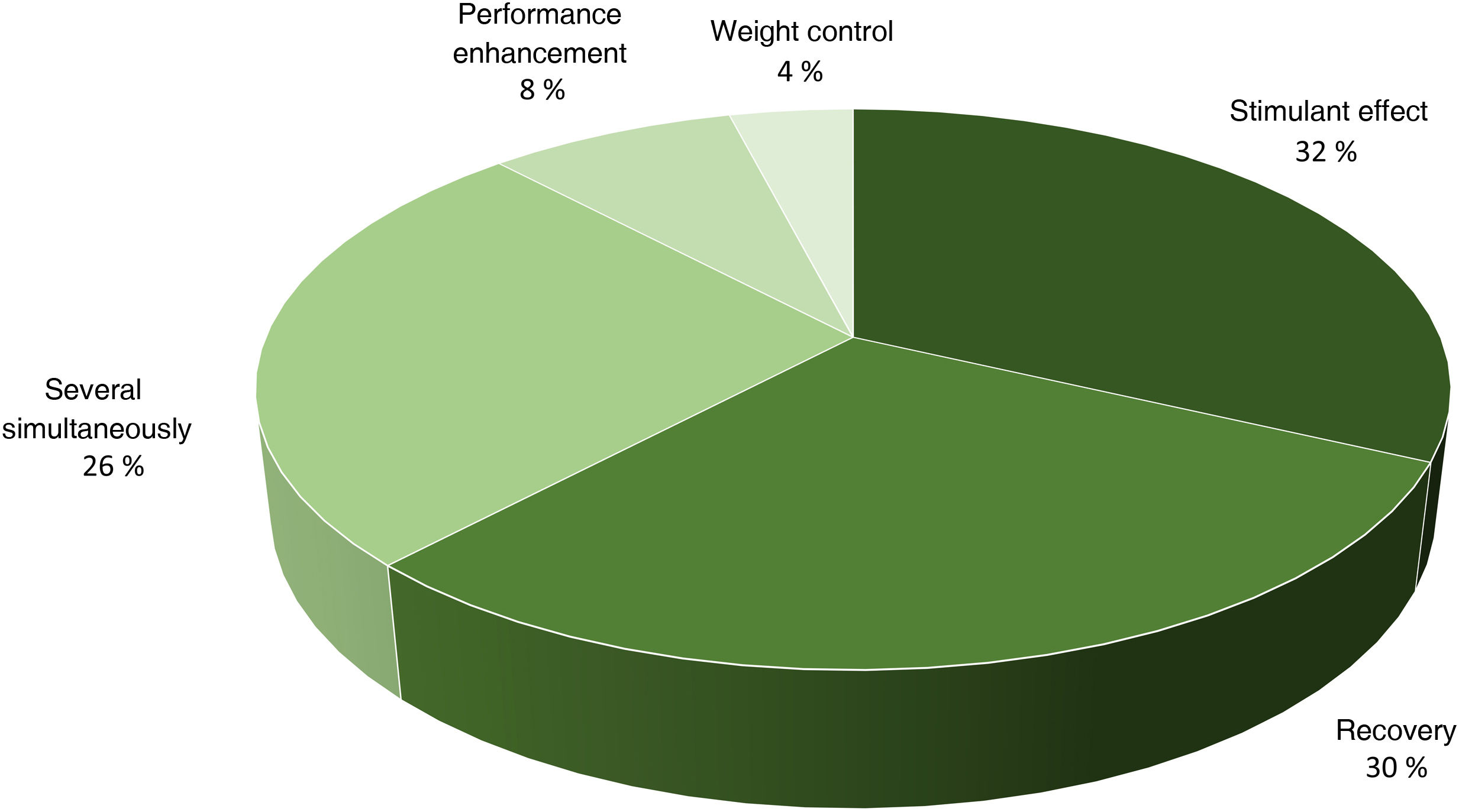
The supplements consumed most frequently were those with a stimulant effect (32.0%), followed by those used for recovery (30.0%); 26% of adolescents who used supplements consumed both types simultaneously (Fig. 3). The recommendation to use supplements most frequently came from friends and schoolmates (47.45%), and supplements were usually purchased in physical stores (61.90%), online (28.57%) and in training facilities (7.14%).
The adolescents that consumed supplements were older and had a higher BMI, differences that were statistically significant. We also found a significant association with the frequency of athletic activity, the usual diet and the use of medication for underlying disease (Table 2). We conducted a univariate and multivariate analysis of the categorical variables significantly associated with the consumption of supplements (Table 3), and found that the significant risk factors were chronic medication and following a weight-loss or a high-protein diet. Moderate physical activity, 3–4 days a week, emerged as a protective factor against the consumption of dietary supplements.
Comparison of participants based on the consumption of supplements.
| Consumed supplements n = 50 | Did not consume supplements n = 213 | P | ||
|---|---|---|---|---|
| Age (years) | 15.54 ± 1.45 | 14.64 ± 1.56 | .0003 | |
| BMI (kg/m2) | 21.30 ± 4.00 | 20.21 ± 3.33 | .0476 | |
| Sex | Male n = 138 | 32 (64.0%) | 106 (49.76%) | .1865 |
| Female n = 116 | 17 (34.0%) | 99 (46.47%) | ||
| Declined to answer n = 9 | 1 (2.0%) | 8 (22.06%) | ||
| Regular medication | No n = 241 | 41 (82.0%) | 200 (93.89%) | .0062 |
| Yes n = 22 | 9 (18.0%) | 13 (6.10%) | ||
| Athletic activity | 1−2 days/week n = 73 | 14 (28.0%) | 59 (27.69%) | .0074 |
| 3−4 days/week n = 122 | 15 (30.0%) | 107 (50.23%) | ||
| 5−7 days/week n = 68 | 21 (42.0%) | 47 (22.06%) | ||
| Usual diet | Balanced n = 174 | 24 (48.0%) | 150 (70.42%) | .0002 |
| High-protein n = 28 | 12 (24.0%) | 16 (7.51%) | ||
| Selective n = 51 | 9 (18.0%) | 42 (19.71%) | ||
| Weight loss n = 10 | 5 (10.0%) | 5 (2.34%) |
BMI, body mass index.
Variables associated with the use of any kind of supplement (logistic regression analysis).
| Consumed supplements | Univariate model | Multivariate model | |||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | ||
| Sex | |||||||
| Male | 23.18% | 1.69 | 0.89 – 3.20 | .10 | 1.53 | 0.72 – 3.25 | .26 |
| Female | 14.65% | 1 | – | – | 1 | – | – |
| Chronic medication | |||||||
| Yes | 40.90% | 3.37 | 1.35 – 8.42 | < .01 | 3.77 | 1.40 – 10.17 | < .01 |
| No | 17.01% | 1 | – | – | 1 | – | – |
| Athletic activity | |||||||
| 5−7 days/week | 30.88% | 1.88 | 0.86 – 4.09 | .11 | 1.39 | 0.56 – 3.43 | .46 |
| 3−4 days/week | 12.29% | 0.59 | 0.26 – 1.30 | .19 | 0.47 | 0.19 – 1.14 | .09 |
| 1−2 days/week | 19.17% | 1 | – | – | 1 | – | – |
| Usual diet | |||||||
| Weight loss | 50.00% | 6.25 | 1.68 – 23.21 | < .01 | 6.00 | 1.55 – 23.19 | < .01 |
| High-protein | 42.85% | 4.68 | 1.97 – 11.11 | < .01 | 3.86 | 1.54 – 9.71 | < .01 |
| Selective | 17.64% | 1.33 | 0.57 – 3.09 | .495 | 1.21 | 0.50 – 2.92 | .66 |
| Balanced | 13.79% | 1 | – | – | 1 | – | – |
CI, confidence interval; OR, odds ratio.
Table 4 presents the differential characteristics of the consumers of protein supplements. Of all adolescents, 10.64% reported consuming protein supplements, which accounted for 56.0% of the dietary supplement consumption reported in our study, with a mean protein intake of 0.26 g/kg/day (SD, 0.18). The most frequent source of information leading to starting consumption of protein supplements was a health care professional (39.13%), in contrast to the respondents that consumed nonprotein food supplements, who chiefly obtained their information from the internet. In the group of protein supplement consumers, 85.18% reported achieving the desired effect, which was to improve their athletic performance or their physical appearance. On the other hand, 18.51% reported experiencing adverse effects: diarrhoea (9.09%), asthenia (4.54%), nausea (4.54%) or oedema (4.54%).
Comparison of participants based on supplement use and type of supplements consumed.
| No supplementsn = 213 | Protein supplementsn = 28 | Nonprotein supplementsn = 22 | P | ||
|---|---|---|---|---|---|
| Age (years) | 14.64 ± 1.56 | 15.78 ± 1.34 | 15.22 ± 1.57 | .0007 | |
| BMI (kg/m2) | 20.21 ± 3.33 | 21.53 ± 4.07 | 21.00 ± 3.99 | .6447 | |
| Sex | Male n = 138 | 106(49.76%) | 19(67.85%) | 13(59.09%) | .3518 |
| Female n = 116 | 99(46.47%) | 8(28.57%) | 9(40.90%) | ||
| Declined to answer n = 9 | 8(4.22%) | 1(3.57%) | 0(0%) | ||
| Chronic medication | No n = 241 | 200(93.89%) | 25(89.28%) | 16(72.72%) | .0026 |
| Yes n = 22 | 13(6.10%) | 3(10.71%) | 6(27.27%) | ||
| Athletic activity | 1−2 days/week n = 73 | 59 (27.69%) | 7 (25.0%) | 7 (31.81%) | .0310 |
| 3−4 days/week n = 122 | 107 (50.23%) | 10 (35.71%) | 5 (22.72%) | ||
| 5−7 days/week n = 68 | 47 (22.06%) | 11 (39.28%) | 10 (45.45%) | ||
| Usual diet | Balancedn = 174 | 150(70.42%) | 14(50.0%) | 10 (45.45%) | .0001 |
| High-proteinn = 28 | 16(7.51%) | 8(28.57%) | 4(18.18%) | ||
| Selectiven = 51 | 42(19.71%) | 5(17.85%) | 4(18.18%) | ||
| Weight lossn = 1 | 5(2.34%) | 1(3.57%) | 4(18.18%) |
BMI, body mass index.
When we compared adolescents who used protein versus nonprotein supplements, we did not find significant differences in age, BMI, sex, chronic medication, frequency of physical activity, usual diet, source of information, reason for consumption, achievement of desired effect or adverse events (Table 5). The only significant difference was the oversight by a professional. Although the consumption of supplements was not monitored externally in most adolescents, in 25.92% of protein supplement consumers, their use was monitored by a professional (physician, coach/trainer or nutritionist), compared to 7.38% of consumers of nonprotein supplements.
Characteristics of the adolescents based on the type of supplement consumed.
| Protein supplements | Nonprotein supplements | P | ||
|---|---|---|---|---|
| Age (years) | 15.78 ± 1.34 | 15.22 ± 1.57 | .1820 | |
| BMI (kg/m2) | 21.53 ± 4.07 | 21.00 ± 3.99 | .6447 | |
| Sex | n = 28 | n = 22 | .4759 | |
| Male n = 32 | 19 (67.85%) | 13 (59.09%) | ||
| Female n = 17 | 8 (28.57%) | 9 (40.90%) | ||
| Declined to answer n = 1 | 1 (3.57%) | 0 (0%) | ||
| Chronic medication | n = 28 | n = 22 | .1303 | |
| No n = 41 | 25 (89.28%) | 16 (72.72%) | ||
| Yes n = 9 | 3 (10.71%) | 6 (27.27%) | ||
| Athletic activity | n = 28 | n = 22 | .6039 | |
| 1−2 days/week n = 14 | 7 (25.0%) | 7 (31.81%) | ||
| 3−4 days/week n = 15 | 10 (35.71%) | 5 (22.72%) | ||
| 5−7 days/week n = 21 | 11 (39.28%) | 10 (45.45%) | ||
| Usual diet | n = 28 | n = 22 | .3564 | |
| Balanced n = 24 | 14 (50.0%) | 10 (45.45%) | ||
| High-protein n = 12 | 8 (28.57%) | 4 (18.18%) | ||
| Selective n = 9 | 5 (17.85%) | 4 (18.18%) | ||
| Weight loss n = 5 | 1 (3.57%) | 4 (18.18%) | ||
| Source of information | n = 23 | n = 16 | .2348 | |
| Internet n = 7 | 2 (8.69%) | 5 (31.25%) | ||
| Schoolmates/friends n = 9 | 5 (21.73%) | 4 (25.0%) | ||
| Health care provider n = 11 | 9 (39.13%) | 2 (12.50%) | ||
| Coach/trainer n = 8 | 4 (17.39%) | 4 (25.0%) | ||
| Nutritionist n = 2 | 2 (8.69%) | 0 (0%) | ||
| Relative n = 2 | 1 (4.34%) | 1 (6.25%) | ||
| Monitoring | n = 27 | n = 17 | .0290 | |
| Self-monitored n = 33 | 20 (74.07%) | 13 (76.47%) | ||
| By professional (physician, trainer, nutritionist) n = 8 | 7 (25.92%) | 1 (7.38%) | ||
| Relative n = 3 | 0 (0%) | 3 (22.14%) | ||
| Motivation | n = 25 | n = 17 | .1238 | |
| To help with training n = 5 | 3 (12.0%) | 2 (11.76%) | ||
| Recovery n = 5 | 4 (16.0%) | 1 (5.88%) | ||
| Performance enhancement n = 18 | 9 (36.0%) | 9 (52.94%) | ||
| Deficient diet n = 8 | 3 (12.0%) | 5 (29.41%) | ||
| Improve appearance n = 6 | 6 (24.0%) | 0 (0%) | ||
| Achieved desired effect | n = 27 | n = 17 | .4655 | |
| Yes n = 36 | 23 (85.18%) | 13 (76.47%) | ||
| No n = 8 | 4 (14.81%) | 4 (23.52%) | ||
| Adverse effects | n = 27 | n = 17 | .5509 | |
| Yes n = 7 | 5 (18.51%) | 2 (11.76%) | ||
| No n = 37 | 22 (81.48%) | 15 (88.23%) | ||
| Place of purchase | n = 27 | n = 15 | .1090 | |
| Physical store n = 26 | 14 (51.85%) | 12 (80.0%) | ||
| Internet n = 12 | 10 (37.03%) | 2 (13.3%) | ||
| Training facility n = 3 | 3 (11.11%) | 0 (0%) | ||
| Pharmacy n = 1 | 0 (0%) | 1 (6.66%) |
The scarcity of studies on the use of protein supplements by adolescents in Spain is noteworthy, and, in fact, we did not find any published in the past 5 years. One of the difficulties we met when we attempted to compare our findings with the current evidence was the heterogeneity of the studies, as some were conducted on the general adolescent population2,4,11,22–27 while others focused on athletes or elite athletes.5,12–14,20,28–32
The percentage of schools that agreed to participate in the study was 50%, similar to the study conducted by Svantorp et al. published in 2021, in which 60% of centres agreed to collaborate.11 Several factors may be at play in this low percentage, such as the lack of time of school staff or limitations of the intranet to give students access to the survey, although schools may have chosen not to participate without a specific reason.
In our study, we found a prevalence of protein supplement consumption of 19.01%, lower compared to the prevalence reported recently in a sample of high school students in Norway (69.05%),11 adolescent athletes in Switzerland (97%)12 and adolescent athletes in Australia (87%).13 The protein supplements used most frequently in our sample were those used for recovery (proteins, glutamine, amino acids, branched-chain amino acids) or with a stimulant effect (caffeine, taurine, pre-workout), a pattern that was similar to the one described by Waller et al. in 2019.13
When it comes to protein supplements in particular, the prevalence of consumption found in our study was of 10.64%, similar to the one reported by Fältström et al. (2022), who reported that 11% of adolescent female football players took protein supplements several days a week.14 Although these percentages may seem high, in reality they are very low in comparison to other studies that report prevalences of 35%,22 49.8%25 or 63%23 in the general adolescent population. These figures are very similar to the ones described in young athletes and sportspersons, which range between 42%13 and 54.5%.31
Our study did not find the consumption of protein supplements to be significantly associated with age, sex, or BMI. This was consistent with the findings of the studies published by Yager et al33 and Waller et al.,13 who also found no differences between consumers and nonconsumers of protein supplements in age, sex13,33 or BMI.33
Adolescents who reported a high-protein diet were the group that used protein supplements most frequently, and the impact of this excessive intake of protein on the development of adverse effects could be investigated in future studies. Barrack et al., whose results differ from ours, found an association between the consumption of protein supplements with very specific aspects of the diet, such as following a vegetarian diet, weight loss in the past year, skipping meals or trying to gain weight.29
The contribution of protein, calculated based on the amount and concentration of the consumed products, reached 25% of the recommended dietary allowance of protein for the adolescents included, so, if we assume that the usual diet contributes an adequate protein intake, the consumption of these supplements would result in an excessive intake in that proportion. However, since we did not know the actual dietary intake of participants, we can only state that the protein supplements consumed by respondents correspond to, or at least would cover, 25% of the recommended daily intake, but we do not know the actual excess, as determining it would require collection of intake data, not to mention the possibility that respondents, out of a lack of knowledge, may not be capable of correctly identifying their own dietary pattern. We did not find any studies in adolescents measuring the protein intake contributed by supplements. The Asociación Española de Pediatría (AEP, Spanish Association of Pediatrics) has noted that there is evidence that protein supplements are not required in the diet of the adolescent,9 agreeing with Berg, who states that adolescent athletes will improve their performance more through adequate nutrition than through any form of supplementation.5
In our study, 85.18% of protein supplement consumers reported achieving the desired effects, as 36.0% perceived an improvement in their athletic performance and 24.0% an improvement in their physical appearance. Jovanov et al., like us, found that the most frequent motivation to use supplements was to enhance athletic performance,31 while Yager et al. found that the desire to increase muscle bulk was a significant predictor of increased consumption.33 The most frequent reasons to consume supplements in the study by Waller et al. were recovery, health maintenance and improved energy.13
There is consensus in the literature that the widespread and substantial use of food supplements is associated to a lack of knowledge4 and use of poor-quality information,12 and it poses a risk to the health of adolescents.4 There is substantial variability in the literature as to who is recommending these products, which may include friends and family,12 coaches or trainers,31 health professionals and online sources.13 In addition, Waller et al. found that younger age and lower income were associated with an increased probability of having relatives and friends as sources of information.13 In our study we also found differences, although not significant, and while consumers of protein supplements mainly obtained information from health professionals (39.13%), consumers of nonprotein supplements obtained information chiefly from the internet.
Most adolescents acquired the supplements in a physical store, a finding that diverged from the only previous study that had analysed the place of purchase, which found that 63% of the youth purchased the products online.20
Another important variable in our study was who monitored the consumption of the supplements, as lack of guidance and monitoring can cause problems, among others, in association with poor body image.4 In our study, most participants controlled their own use of supplements, which was consistent with the findings of a study by Tsarouhas et al., in which none of the adolescents had consulted with a physician or nutritionist.20 Health care professionals must increase their knowledge on the indications, interactions and potential adverse effects of protein supplements,2 which is essential for these products to be used as safely and effectively as possible.5 Although the AEP strongly recommends that supplements be prescribed and their use monitored by a specialist,9 the aggressive advertising of these products promotes their misuse by adolescents.4,24
Another aspect that must be taken into account is that due to the lack of legislation regulating supplements, it is easier for these products to be contaminated.4 Tsarouhas et al. concluded that 9% of the products were contaminated with substances that had endocrine modulating properties not stated in the label,20 and the AEP has warned of the presence of doping substances in several of the supplements in the market.9 Martínez-Sanz et al. reached similar conclusions in a study in adults, finding issues such as the presence of legal substances at doses exceeding the recommended threshold.19
In our study, 18.51% of the adolescents who used protein supplements reported some form of adverse event. There was hardly any data on the adverse events associated with protein supplements in the reviewed literature, and given the lack of guidance and monitoring by health care professionals, their incidence is probably greater than we expect. The only source in our literature search that made reference to adverse events was the review by Ganson et al., which found that the consumption of supplements was associated with adverse medical events, in addition to alcohol problems and future anabolic-androgenic steroid use.22 Determining the actual incidence of adverse events is complicated, and doing so would require a prospective study with short- and long-term follow-up.
Among the limitations of our study are the low participation (only 6 of the randomly selected schools agreed to participate), that we did not obtain data concerning the social environment or socioeconomic status of the adolescents, and that, due to its cross-sectional nature, it was not possible to establish causality. In addition, the sample size was calculated for the purpose of the primary objective, which was to determine the prevalence of consumption, but the size may not have been sufficient to find differences in the factors associated with supplement us in certain subgroups. Another limitation concerned the anonymous participation of the students and schools and the lack of direct contact with them, which precluded the calculation of the response rate, overall and per school. But the most important limitation is probably the study design, as the data were obtained in an anonymous survey through a questionnaire completed by adolescents without guidance, so that the reliability of certain aspects may not be optimal, such as the knowledge of adolescents of what constitutes a balanced diet, specific clinical aspects related to chronic diseases or the particular circumstances under which supplement consumption is considered sporadic or regular.
Despite these limitations, our study had a sufficiently large sample and a sample selection method that was adequate to consider its findings representative of the consumption of food supplements in adolescents in our region. In addition, since the data collection process was completely anonymous, it is fair to assume that the results are reliable, and not biased due to the knowledge that the participants or the schools could be identified. In future studies, it would be interesting to include adolescents from different populations, attending private and/or publicly funded private schools and who are professional athletes. Ideally, participants would undergo a more reliable and thorough nutritional assessment with laboratory tests and anthropometric measurement, although this would entail the loss of anonymity.
In conclusion, the prevalence of food supplement consumption by adolescent is higher than would be desired, and protein supplements are the most commonly consumed. These supplements may contribute an amount of protein of up to 25% of the recommended intake for adolescents and, paradoxically, adolescents who reported consuming a high-protein diet were also the group with the highest consumption of protein supplements. A large proportion of adolescents experienced adverse effects due to the use of these products, and most managed their consumption themselves, despite the recommendation of the AEP to subject their consumption to strict monitoring and follow-up by a specialist. Our findings suggest that this is a serious although latent problem for which data are unavailable to predict trends for the next few years. Although larger studies are needed, we are convinced that the health care authorities must strictly control the advertising, distribution and sale of dietary supplements to adolescents.
FundingThe authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
