


The prevalence of ankyloglossia has been estimated at around 4% of live births. Its prevalence at national level is unknown.
Material and methodsThis is a multicenter, prospective observational study. Six hospitals in Asturias took part. All newborns were examined on Sundays, Tuesdays and Thursdays for 3 months. Coryllos and Hazelbaker criteria were used to diagnose ankyloglossia.
ResultsThe prevalence in the 667 newborns examined was 12.11% (95% CI: 9.58–14.64), of whom 62% were male. One in 4 children with ankyloglossia had a family history. According to Coryllos’ classification, type II was the most common (54%).
ConclusionsThe prevalence of ankyloglossia in Asturias was 2–3 times higher than expected.
The diagnostic criteria for ankyloglossia needs to be unified, and further studies are required to determine the association with breastfeeding difficulties and other health problems.
La prevalencia de anquiloglosia ha sido estimada alrededor del 4% de los recién nacidos vivos. Se desconoce la situación a nivel nacional.
Material y métodosEstudio multicéntrico, observacional, prospectivo en el que participaron 6 hospitales asturianos. Durante 3 meses se exploró a todos los recién nacidos los días domingo, martes y jueves. Para el diagnóstico de anquiloglosia se utilizaron los criterios de Coryllos y Hazelbaker.
ResultadosSe exploró a 667 recién nacidos. La prevalencia de anquiloglosia fue del 12,11% (IC 95%: 9,58-14,64). El 62% eran varones. Uno de cada 4 niños con anquiloglosia tenía antecedentes familiares de frenillo lingual corto. Según la clasificación de Coryllos el tipo ii fue el más frecuente (54%).
ConclusionesLa prevalencia de anquiloglosia en Asturias fue 2 o 3 veces superior a la esperada.
Es necesario unificar los criterios diagnósticos, así como realizar estudios para conocer su asociación con dificultades en la lactancia u otros problemas posteriores.
Ankyloglossia is defined as an embryological remnant of tissue remnant between the undersurface of the tongue and the floor of the mouth that restricts normal tongue movement.1
It has been linked to latch-on difficulties and maternal pain, which are 2 of the main causes of weaning in our environment.1 Therefore, it could be the source of breastfeeding problems, a circumstance that has not been proven mainly due to the methodological limitations of the published studies.
The Hazelbaker score assessment2 is the tool commonly used for diagnosis. Its main drawback is that it has low inter-rater reliability, especially for the function items.3 The Coryllos classification allows the distinction of different types of ankyloglossia based on the insertion point of the frenulum.
There are no standardised objective clinical criteria for the diagnosis of ankyloglossia, so the prevalence rates observed in the literature are varied (4–10%), with varying study designs that complicate or prevent their comparison.1,4,5 In Asturias there is a reported prevalence of 2% among schoolchildren.6 But the prevalence among newborns at the national and regional level for the rest of Spain is unknown. Our objective was to learn the current prevalence of ankyloglossia in Asturias.
Materials and methodsType of studyWe did a prospective, observational, multi-centre study with the participation of 6 out of the 8 public hospitals in the Principality of Asturias.
For 3 months (from June 1 to August 31, 2012) a researcher examined all the neonates born in each centre on Sunday, Tuesday, and Thursday. All newborns with gestational age less than 34 weeks or birth weight below 1500g were excluded. We obtained informed consent prior to participation. The study was approved by the regional research ethics committee, the Comité Regional de Ética de Investigación (N. 68/2012).
Case definitionTo classify the newborns as having or not having ankyloglossia, we inspected and palpated the tongue and assessed its function during the examinations performed within the first 48h of life. To homogenise criteria, prior to the study we conducted a workshop with images and practicing on newborns to train all the participants in the application of the Hazelbaker classification, as well as a month-long pilot study. To classify a patient as having ankyloglossia the following two criteria had to be met:
- -
Anatomical criterion: detection, by examination or palpation, of a membrane anterior to the base of the tongue extending to the floor of the mouth. The patients were classified according to the Coryllos classification7 (Fig. 1).
 Figure 1.
Figure 1.Coryllos anatomical classification
•Type I: thin and elastic frenulum; attaches the tip of the tongue to the alveolar ridge, and the tongue forms a heart shape.
•Type II: thin and elastic frenulum; 2–4mm behind the tongue tip, attaches by the alveolar ridge.
•Type III: thick, fibrous, and non-elastic frenulum; attaches mid-tongue to the floor of the mouth.
•Type IV: the frenulum is not seen, but felt, with fibrous or submucosal thick and shiny attachment from the base of the tongue to the floor of the mouth.
- -
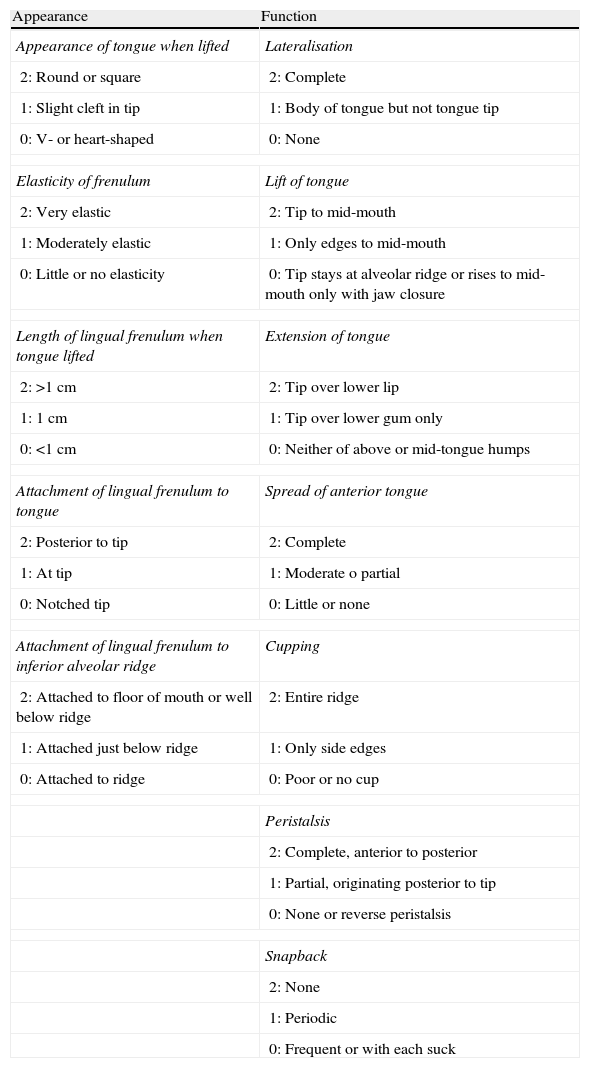
Functional criterion: score ≤4 out of 6 obtained by analysis of the first 3 function items of the Hazelbaker assessment tool: lateralisation, lift, and extension of tongue3 (Table 1).
Table 1.Hazelbaker assessment.
Appearance Function Appearance of tongue when lifted Lateralisation 2: Round or square 2: Complete 1: Slight cleft in tip 1: Body of tongue but not tongue tip 0: V- or heart-shaped 0: None Elasticity of frenulum Lift of tongue 2: Very elastic 2: Tip to mid-mouth 1: Moderately elastic 1: Only edges to mid-mouth 0: Little or no elasticity 0: Tip stays at alveolar ridge or rises to mid-mouth only with jaw closure Length of lingual frenulum when tongue lifted Extension of tongue 2: >1cm 2: Tip over lower lip 1: 1cm 1: Tip over lower gum only 0: <1cm 0: Neither of above or mid-tongue humps Attachment of lingual frenulum to tongue Spread of anterior tongue 2: Posterior to tip 2: Complete 1: At tip 1: Moderate o partial 0: Notched tip 0: Little or none Attachment of lingual frenulum to inferior alveolar ridge Cupping 2: Attached to floor of mouth or well below ridge 2: Entire ridge 1: Attached just below ridge 1: Only side edges 0: Attached to ridge 0: Poor or no cup Peristalsis 2: Complete, anterior to posterior 1: Partial, originating posterior to tip 0: None or reverse peristalsis Snapback 2: None 1: Periodic 0: Frequent or with each suck

There are about 1750 births in Asturias each trimester. We estimated a sample size of 625 newborns, based on an estimated prevalence of 2–5%, a desired precision of 1.2–1.8%, and 95% confidence level.
ResultsWe examined a total of 677 newborns, of whom 82 met the diagnostic criteria for ankyloglossia. The total prevalence was 12.11% (95% CI: 9.58–14.64). Depending on the hospital, the prevalence ranged between 3.4% and 50% (Fig. 2).

Of the 82 patients with a short frenulum, 62% were male. Normal delivery was reported in 57% of cases, instrumental delivery in 37% and caesarean in the remaining 6%. There was a family history of ankyloglossia in 1 out of 4 newborns diagnosed with the condition, which in most cases (86%) concerned first-degree relatives: parents or siblings.
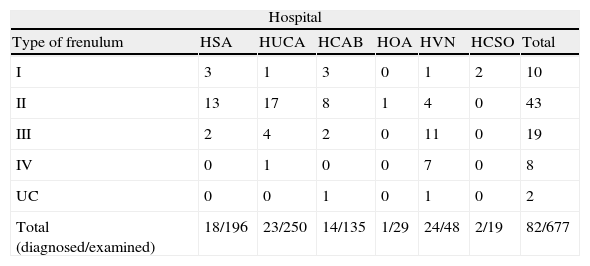
According to the Coryllos anatomical classification, 10 patients (12%) had a type I frenulum, 43 patients (54%) a type II, 19 patients (24%) a type III, and 8 patients (10%) a type IV. The distribution by hospital is shown in Table 2.
Anatomical classification of ankyloglossia cases distributed into the hospitals where they were diagnosed.
| Hospital | |||||||
| Type of frenulum | HSA | HUCA | HCAB | HOA | HVN | HCSO | Total |
| I | 3 | 1 | 3 | 0 | 1 | 2 | 10 |
| II | 13 | 17 | 8 | 1 | 4 | 0 | 43 |
| III | 2 | 4 | 2 | 0 | 11 | 0 | 19 |
| IV | 0 | 1 | 0 | 0 | 7 | 0 | 8 |
| UC | 0 | 0 | 1 | 0 | 1 | 0 | 2 |
| Total (diagnosed/examined) | 18/196 | 23/250 | 14/135 | 1/29 | 24/48 | 2/19 | 82/677 |
HCAB: Hospital de Cabueñes; HCSO: Hospital Carmen y Severo Ochoa; HOA: Hospital del Oriente de Asturias; HSA: Hospital San Agustín; HUCA: Hospital Central de Asturias; HVN: Hospital Valle del Nalón; UC: unclassified.
The 12% prevalence is the highest reported in the literature up to now, between 2 and 3 times greater than expected.1,4,5,8,9 This circumstance reminds us of the importance of examining the oral cavity in newborns, with special emphasis on the assessment for ankyloglossia.
The Coryllos classification allowed the identification by means of palpation of type III and IV frenula that may be missed in a visual inspection.7 On the other hand, we believe that functional criteria must be used in the diagnosis. If we were to use anatomical criteria alone, it would seem, erroneously, as if many newborns had ankyloglossia.
We are aware that it is difficult to assess the range of movement of the tongue correctly, and that there may be inter-rater differences. For these reasons, we used the first 3 function items of Hazelbaker as diagnostic criteria, as they have shown substantial inter-rater agreement (kappa values 0.6 and 0.7) and are easier to assess.3 The cut-off point used in the study (score ≤4), proposed by Amir,3 showed a strong correlation with Hazelbaker's definition of significant ankyloglossia: score <11 out of 14, if all the function items are analysed.2
The observed prevalence was greater than expected. This difference may be due to the digital examination that allowed the identification of cases that could not be detected by visual inspection (34% of types III–IV). The proportion of this type of ankyloglossia was similar in 5 hospitals; in one other hospital up to 65% of frenula fell into this category. This fact may suggest a classification bias resulting from subjectivity and the difficulty involved in establishing anatomical limits. Nevertheless, the results from the 3 hospitals with the largest populations in the study (85% of the sample), were pretty homogeneous, with a prevalence of 10%.
The short, type IV lingual frenulum may be the most difficult to diagnose. There are no data on its prevalence, as this classification is not specified in the published studies. Recently, O’Callahan10 described the performance of 131 frenotomies in newborns younger than one month with breastfeeding problems, with type IV being the most frequently treated (40%).
In our series, 10% of the frenula were classified as type IV, although most of them were diagnosed at a single hospital. Without the participation of this centre, the prevalence of this type of ankyloglossia would be 0.16% and it would account for 1% of the lingual frenula. We do not know whether the criteria used results in underdiagnosis of this type of frenula, so that its prevalence may be even higher than the observed 12%. Still, this once again underscores a subjective factor dependent on the assessor.
There was a family history of ankyloglossia in up to 25% of patients, most concerning first-degree relatives. Genetics play an important role in this condition. Ankyloglossia can be seen in isolation or associated with syndromes such as Ehlers–Danlos, Beckwith–Wiedemann, Simosa, and orofaciodigital syndrome. The higher prevalence in males, along with genetic studies, suggest a pattern of X-linked inheritance.11,12
One of the limitations of the study was interobserver variability. The performance of a practical workshop and an early pilot study allowed us to unify the criteria among researchers. However, these did not suffice, as can be seen in the prevalence disparity of one of the centres. The use of functional criteria lessened this limitation and helped objectivise the subjectivity in diagnosing ankyloglossia, especially for types III and IV.
To our knowledge, this is the first study on the prevalence of ankyloglossia in newborns in Spain. García Pola et al.6 found a prevalence of 2% in our region, but in 6-year-old children. In contrast to other publications, our study employed objective diagnostic criteria and the anatomical classification. The only 2 centres in our region that did not participate account for less than 8% of all births. Furthermore, their socioeconomic factors are equivalent to those of other hospitals that were included, and thus our data are representative of the prevalence of ankyloglossia in Asturias.
To conclude, we found a high prevalence of ankyloglossia. Newborn and infant check-ups should include a routine examination of the oral cavity, focusing on the presence of ankyloglossia, to ensure detection of this condition. Further research is needed in order to unify diagnostic criteria and to elucidate the impact of ankyloglossia on breastfeeding and other problems that may arise later in life.
FundingThis study was funded by the Ernesto Sánchez Villares Foundation on the occasion of the XV Convocatoria de Ayuda a la Investigación Clínica y Epidemiológica of year 2012 (project 15/2012).
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: González Jiménez D, Costa Romero M, Riaño Galán I, González Martínez M, Rodríguez Pando M, Lobete Prieto C. Prevalencia de anquiloglosia en recién nacidos en el Principado de Asturias. An Pediatr (Barc). 2014;81:115–119.
