





Although several tools have been developed to assess general HRQoL in children, parental reports are required to supplement this information, especially in very young children. The parents version of the Kiddy-KINDL-R was developed to assess HRQoL in children aged 3–7 years through the reports of their parents or legal guardians.
ObjectiveThe aim of this study was to validate the parents version of the Kiddy-KINDL-R questionnaire and assess its psychometric properties in a sample of Spanish preschool-aged children.
MethodCross-sectional study in 283 parents or legal guardians of children aged 3–6 years that completed the Kiddy-KINDL-R questionnaire and an additional scale to assess anxiety problems. We performed confirmatory factor analysis to assess whether the original Kiddy-KINDL-R version fit the Spanish data; we assessed internal consistency by means of the ordinal alpha and the discriminant validity by means of the Preschool Anxiety Scale.
ResultsAlthough the original six-factor model showed a good fit, we propose a model consisting of 22 items and the same 6 factors for the Spanish version. The reliability was excellent, and the internal consistency values were adequate. Our results showed significant negative correlations between the Kiddy-KINDL-R and the external anxiety measure, which was evidence of discriminant validity.
ConclusionWe demonstrated that the Spanish version of the Kiddy-KINDL-R had good psychometric properties and that this questionnaire is an adequate assessment tool that could be useful in clinical practice.
A pesar de que se han desarrollado diferentes medidas para evaluar la CVRS general en menores, se necesitan los informes de los padres para complementar la información (calidad de vida relacionada con la salud), especialmente cuando son demasiado pequeños. La versión para padres y madres del Kiddy-KINDL-R se diseñó para medir la CVRS general en niños de 3 a 7 años a través de las respuestas de sus progenitores y tutores.
ObjetivoEl objetivo del presente estudio es validar la versión parental del cuestionario Kiddy-KINDL-R y evaluar sus propiedades psicométricas en una muestra española de menores en edad preescolar.
MétodoEn este estudio transversal, 283 madres, padres o tutores de menores de entre 3 y 6 años respondieron al cuestionario Kiddy-KINDL-R y a otra medida de problemas de ansiedad. Se realizó un análisis factorial confirmatorio para examinar si el modelo Kiddy-KINDL-R original se ajustaba a los datos españoles; la consistencia interna se estimó utilizando α ordinal y la validez discriminante se examinó con la Escala de Ansiedad Preescolar.
ResultadosEl modelo original de 6factores demostró buen ajuste, pero se propuso un modelo compuesto por 22 ítems y los mismos 6factores para la versión española. La fiabilidad fue excelente y los valores de consistencia interna fueron adecuados. Los resultados revelaron correlaciones significativas y negativas entre Kiddy-KINDL-R y la medida de ansiedad, lo que apoya la validez discriminante.
ConclusiónLa versión española del Kiddy-KINDL-R demostró buenas propiedades psicométricas y constituye un instrumento adecuado que podría ser útil para la evaluación en la práctica clínica.
Some medical treatments and lengthy stays in hospital can be unpleasant experiences for children. These situations not only affect their physical health, but also have a negative impact on psychological well-being, behaviour, academic performance and social competence in children.1–3 In order to identify the level of physical well-being, health care needs and socio-affective status of children, it is important to assess the Health-Related Quality of Life (HRQoL).4 The HRQoL constitutes a multidimensional construct that can be reported by patients or proxies.
Different assessment instruments have been developed to assess generic HRQoL in children, such as the Paediatric Quality of Life instrument,5 the KINDL,6 and the KIDSCREEN.7 These instruments provide a self-reported version for children as well as a parent-reported version, both of which are classified according to the child's age. Despite the availability of different measures of HRQoL, very young children have difficulty understanding some questions or expressing their feelings, so parental reports are needed to complement child-reported information.8 Furthermore, research on HRQoL in children has shown some lack of agreement between the information provided by parents and that provided by children, which makes it essential to gather information from both sources for a more reliable measurement of this construct.8–12
Parent reports are usually required since preschool-aged children have limited language skills, perceive time differently and have difficulty reporting their perceived HRQoL, making their information unreliable. Such proxy reports are particularly useful for assessing objective aspects of children's behaviour.13 The most widely used instruments for assessment of HRQoL in children aged less than 5 years as perceived by the parents are the Infant and Toddler Quality of Life questionnaire (ITQOL),14 the TNO-AZL Preschool children Quality of Life questionnaire (TAPQOL),15 the Paediatric Quality of Life Inventory (PedsQL),16 the DISABKIDS smiley questionnaire,17 and the Kiddy-KINDL Questionnaire–Parent Version.18
The Kiddy-KINDL Questionnaire18 was designed to measure generic HRQoL in children aged 3–7 years. This scale is within the umbrella of the KINDL questionnaire,6 which can be used between ages 4 and 16 years [http://www.kindl.org/]. There are two versions of the Kiddy-KINDL instrument, one to be completed by parents and one to be completed by the children. The parents’ version has 24 items rated on a 5-point Likert scale that ranges from ‘never’ (1) to ‘all the time’ (5) and is structured in 6 dimensions: Physical Well-Being, Emotional Well-Being, Self-Esteem, Family, Friends, and Everyday Functioning. There are another 22 items that could be considered an additional subscale, known as ‘Kiddy Parents’, to supplement self-reported information obtained with the children's questionnaire. The children's questionnaire contains 12 items, 2 for each dimension, and corresponds in structure to the parents’ version. Since the Kiddy-KINDL assesses HRQoL independent of health status, an additional subscale is available for both versions, the Disease module, which comprises 6 questions to assess specific diseases (children's version, Items 14–19; parents’ version, 48–53). The parents’ version of the Kiddy-KINDL has proven useful in the assessment of HRQoL in different countries, exhibiting an adequate internal consistency with Cronbach alpha values ranging from 0.84 to 0.89.7,19,20
The Kiddy-KINDL has been translated into more than 25 languages worldwide, including Spanish.21 However, the psychometric properties of the Spanish version of the KINDL questionnaire have only been evaluated in the self-reported version for children aged 8–16 years.22 Therefore, the aim of our study was to validate the Kiddy-KINDL parents’ version and to examine its psychometric properties in a sample of Spanish preschool-aged children. We hypothesised that: (1) The Spanish version of the Kiddy-KINDL would maintain the original six-factor structure and would be a reliable and valid measure of HRQoL in preschoolers; and (2) scoring higher on the Kiddy-KINDL dimensions (physical well-being, emotional well-being, self-esteem, family, friends, and everyday functioning) would correlate to scoring lower in anxiety measures.
MethodsParticipantsWe performed a cross-sectional study that included 283 parents or guardians of children aged 3–6 years enrolled in 6 schools in Alicante, Spain. The inclusion criteria were having a child aged 3–6 years and providing written consent to participate in the study. The age of participants ranged between 20 and 50 years (mean, 37.12; SD=5.25). Based on parental employment status and professional category, the predominant socioeconomic category in the sample was middle class. Mothers (83%), fathers (16.3%), and other guardians (0.7%) completed a questionnaire about their children's HRQoL and other anxiety measures. The mean age of their children was 4.09 years (SD=1.12), and 47% were girls. Most participants were Spanish nationals (92.9%). Table 1 provides more information about the sample characteristics.
Sociodemographic characteristics of participants.
| Type of schools | |
| 3 Public | 148 (52.3) |
| 3 Private | 135 (47.7) |
| Children | |
| Female, N (%) | 133 (47) |
| Mean age (SD), years | 4.09 (1.12) |
| 3 years | 115 (42.3) |
| 4 years | 61 (22.4) |
| 5 years | 52 (19.1) |
| 6 years | 44 (16.2) |
| Parents (evaluator) | |
| Female, N (%) | 235 (83) |
| Mean age (SD), years | 37.12 (5.25) |
| Nationality | |
| Spanish | 263 (92.9) |
| Other | 20 (7.1) |
| Marital status | |
| Married | 227 (80.2) |
| Separated or divorced | 18 (6.4) |
| Domestic partnership (unmarried) | 5 (1.8) |
| Single | 26 (9.2) |
| Other (not specified) | 7 (2.4) |
| Education | |
| Primary education | 41 (15.3) |
| Compulsory secondary education | 43 (16) |
| High school | 54 (20.2) |
| University education | 130 (48.5) |
Sociodemographic section. We collected data on the occupation and educational attainment of the head of household, and on the gender, age and number of siblings of the children.
Kiddy-KINDL-R.18 This instrument was created to assess HRQoL in children aged 3–7 independently of their current health. There are 2 versions of the questionnaire, one to be completed by parents and one to be completed by the children. In this study we used the parents’ version. It consists of 24 items grouped into six dimensions: Physical well-being, Emotional well-being, Self-esteem, Family, Friends, and Everyday functioning (School or Nursery school/Kindergarten). Parents are asked to rate the items on a 5-point Likert scale: never (1), almost never (2), sometimes (3), often (4), and always (5). The total score is calculated by adding the scores of all the dimensions (possible range per dimension, 4–20). Higher scores on individual subscales and on the whole scale indicate a better HRQoL in children.
Preschool Anxiety Scale (PAS).23 The PAS is a parent-based scale that evaluates anxiety and worries in young children aged 3–7 years. This questionnaire comprises 28 items grouped into five subscales: generalised anxiety disorder, social anxiety disorder/social phobia, separation anxiety disorder, obsessive-compulsive disorder, and physical injury fears. Each anxiety symptom is rated on a 4-point scale according to its frequency: never (0), sometimes (1), often (2), or always (3). The total score and subscale scores are calculated by adding the ratings of all the relevant items. The original version has demonstrated good construct validity against a measure of internalising disorders (r=0.59).23 The Spanish version, used in this study, was translated by Orgilés et al.,24 who demonstrated its reliability and construct validity in a format with only 20 items. The internal consistency found in our sample was excellent (Cronbach's α=0.94).
ProcedureFirst, we obtained the approval of the ethics committee of the responsible University in Spain. In this study, we used the Spanish version of the Kiddy-KINDL adapted by Rajmil et al.21 This version was developed through a rigorous process of semantic and transcultural adaptation for Spanish children, described in detail by Rajmil et al.21
We contacted 6 public and private children's schools in the southeast of Spain (Comunidad Valenciana). We informed school principals of the purpose of the study, requesting their collaboration to recruit parents and legal guardians of children aged 3–6 years. We sent written information about the study and obtained written consent from all participants. A total of 675 families were invited to participate and 283 finally enrolled in the study. Participants completed the paper questionnaires at home and returned them in a sealed envelope to the person that was the point of contact for the study. The envelope that contained the battery of tests also included instructions on how to complete them. Participants were given a dedicated phone number that they could call if they had any questions or concerns.
Statistical analysisWe performed the descriptive analysis of the sample and the instruments used in the study with the software SPSS version 25. We analysed the differences in Kiddy-KINDL-R and PAS scores based on children's age and sex, the evaluator (mother, father or other guardians) and the type of school (public or private). When the differences between groups were statistically significant, we calculated the Cohen d. We performed confirmatory factor analysis (CFA) to test the Kiddy-KINDL-R model proposed by the authors of the original questionnaire.18 We performed CFA with R Studio and the Lavaan structural model package version 0.5–12 (beta).25 We assessed the fit of the model based on 3 indexes used internationally: the CFI (comparative fit index), the TLI (Tucker-Lewis index), and the RMSEA (root mean square error of approximation). We used the values proposed by Hu and Bentler (1999)26 as reference. We defined a good model fit as CFI and TLI values greater than 0.90 and a RMSEA value of 0.08 or less. We applied the diagonally weighted least squares method (DWLS) recommended for non-normally distributed ordinal data.27,28 The internal consistency of the total scale and the subscales was assessed by calculating ordinal alpha values.29,30 We assessed divergent validity by calculating the bivariate Spearman correlations between the Spanish version of Kiddy-KINDL-R and an instrument for assessment of the main anxiety disorders (PAS).
ResultsSociodemographic characteristicsTable 1 summarises the sociodemographic characteristics of the participants, including the age and sex of the children and the evaluators’ age, sex, educational attainment, nationality and marital status.
Item analysesTable 2 presents the descriptive statistics for the original 24-item version of the Kiddy-KINDL-R: mean and standard deviation for each item, item-total correlation (rita) and ordinal alpha eliminating the item (α−i). Table 3 presents the mean, standard deviation, range and ordinal alpha (α) for each factor and for the total scale. The values for item-total correlations were greater than 0.33, except for Item 21 (rita=0.11). All items were included in the model, since eliminating one of them did not result in an increase in internal consistency.
Psychometric properties of each item in the original 24-item version of the Kiddy-KINDL.
| Item 1 | 1.58 | 1.28 | .57 | .91 |
|---|---|---|---|---|
| Item | M | SD | rita | α−i |
| 1 | 4.53 | 0.75 | 0.35 | 0.89 |
| 2 | 4.17 | 0.84 | 0.33 | 0.89 |
| 3 | 4.02 | 0.84 | 0.40 | 0.89 |
| 4 | 4.34 | 0.68 | 0.43 | 0.89 |
| 5 | 4.35 | 0.69 | 0.44 | 0.89 |
| 6 | 4.01 | 0.77 | 0.35 | 0.89 |
| 7 | 4.57 | 0.72 | 0.35 | 0.89 |
| 8 | 4.08 | 0.89 | 0.44 | 0.89 |
| 9 | 3.95 | 0.83 | 0.48 | 0.89 |
| 10 | 4.14 | 0.87 | 0.46 | 0.89 |
| 11 | 4.23 | 0.76 | 0.45 | 0.89 |
| 12 | 3.86 | 0.78 | 0.65 | 0.89 |
| 13 | 4.23 | 0.69 | 0.38 | 0.89 |
| 14 | 4.58 | 0.70 | 0.40 | 0.89 |
| 15 | 4.10 | 0.88 | 0.40 | 0.89 |
| 16 | 3.89 | 0.88 | 0.44 | 0.89 |
| 17 | 4.31 | 0.76 | 0.48 | 0.89 |
| 18 | 4.37 | 0.68 | 0.45 | 0.89 |
| 19 | 4.42 | 0.61 | 0.46 | 0.89 |
| 20 | 4.30 | 0.95 | 0.63 | 0.89 |
| 21 | 4.28 | 0.83 | 0.11 | 0.88 |
| 22 | 4.58 | 0.61 | 0.31 | 0.89 |
| 23 | 4.50 | 0.76 | 0.43 | 0.89 |
| 24 | 3.90 | 0.79 | 0.40 | 0.89 |
M, mean; rit.
Psychometric properties of the dimensions of the original 24-item version of the Kiddy-KINDL-R.
| Dimensions | M | SD | Range | α |
|---|---|---|---|---|
| Physical well-being | 17.06 | 2.18 | 6–20 | 0.71 |
| Emotional well-being | 17.01 | 2.13 | 8–20 | 0.72 |
| Self-esteem | 16.17 | 2.13 | 6–20 | 0.75 |
| Family | 16.78 | 2.20 | 9–20 | 0.73 |
| Friends | 17.40 | 2.20 | 10–20 | 0.80 |
| Nursery school/kindergarten | 17.25 | 2.04 | 6–15 | 0.64 |
| Total score of Kiddy-KINDL-R | 101.70 | 9.32 | 66–119 | 0.90 |
M, mean; SD, standard deviation; α, ordinal alpha.
The 24-item model distributed into six factors of the Kiddy-KINDL-R fit the Spanish sample adequately: CFI=0.97; TLI=0.96; RMSEA=0.08 (95% CI=0.073, 0.087). Each of the factors included four items, and the mean factor loading for each dimension was adequate: Physical well-being (F1=0.52; range, 0.35–0.66), Emotional well-being (F2=0.58; range, 0.25–0.80), Self-esteem (F3=0.32; range, 0.35–0.72), Family (F4=0.57; range, 0.35–0.72), Friends (F5=0.42; range, 0.31–0.57), and Nursery school/Kindergarten (F6=0.52; range, 0.13–0.82). The factor loadings were higher than 0.30 for all items except items 5 (‘…my child had fun and laughed a lot’, F2) (0.25), 10 (‘…my child felt on the top of the word’, F3) (0.27), 11 (‘…my child felt pleased with himself’, F3) (0.04) and 22 (‘…my child enjoyed the Nursery school/Kindergarten’, F6) (0.13).
Despite the adequate fit of the original model, we tested an alternative model from which we had removed items 11 (F3) and 22 (F6) due to their limited contribution (factorial loadings of 0.04 and 0.13, respectively). The proposed model comprised 22 items and maintained the same factors as the original model; each factor included 4 items, except Factors 3 and 6 with 3 items each. This alternative model (without items 11 and 22) also showed a good fit to the Spanish data: CFI=0.95; TLI=0.94; RMSEA=0.08 (95% CI=0.079, 0.094) (Table 4). Although the CFI and TLI values decreased slightly, they were higher than the cutoffs proposed by Hu and Bentler (1999).26 The factor loadings of most of the items increased compared to their loadings in the initial 24-item model. Coefficients were greater than 0.29 for all items except item 10 (‘…my child felt on top of the world’ (0.25). We kept this item in the model for its clinical relevance and because its factor loading was near the established cutoff of 0.30. Table 4 presents the factor loadings for the 22-item model. Thus, the final parents’ version of Kiddy-KINDL-R in Spanish comprises 22 items.
Confirmatory factorial analysis: factor loadings (n=283).
| During the past week… | F1 | F2 | F3 | F4 | F5 | F6 | |
|---|---|---|---|---|---|---|---|
| 1. | … my child had fun and laughed a lot | 0.51 | |||||
| 2. | … my child had a headache or tummy-ache | 0.54 | |||||
| 3. | … my child was tired and worn-out | 0.66 | |||||
| 4. | … my child felt strong and full of energy | 0.41 | |||||
| 5. | … my child had fun and laughed a lot | 0.27 | |||||
| 6. | … my child didn’t feel much like doing anything | 0.66 | |||||
| 7. | … my child felt alone | 0.60 | |||||
| 8. | … my child felt scared or unsure of her-/himself | 0.79 | |||||
| 9. | … my child was proud of him-/herself | 0.33 | |||||
| 10. | … my child felt on top of the world | 0.25 | |||||
| 12. | … my child had lots of good ideas | 0.67 | |||||
| 13. | … my child got on well with us as parents | 0.35 | |||||
| 14. | … my child felt fine at home | 0.55 | |||||
| 15. | … we quarrelled at home | 0.70 | |||||
| 16. | … my child felt that I was bossing him/her around | 0.72 | |||||
| 17. | … my child played with friends | 0.48 | |||||
| 18. | … my child was liked by other kids | 0.29 | |||||
| 19. | … my child got along well with his friends | 0.33 | |||||
| 20. | … my child felt different from other children | 0.58 | |||||
| 21. | … my child coped well with the assignments set in nursery school/kindergarten | 0.60 | |||||
| 23. | … my child looked forward to nursery school/kindergarten | 0.50 | |||||
| 24. | … my child made lots of mistakes when doing minor | 0.78 | |||||
F1, physical well-being; F2, emotional well-being; F3, self-esteem; F4, family; F5, friends; F6, nursery school/kindergarten.
We found adequate internal consistency values for the 6 dimensions in the 22-item version of the Kiddy-KINDL-R: Physical well-being (αF1=0.71), Emotional well-being (αF2=0.72), Self-esteem (αF3=0.77), Family (αF4=0.73), Friends (αF5=0.80), and Nursery school/Kindergarten (αF6=0.58). The internal consistency of the total scale was excellent (α=0.90).
Correlations between dimensionsThe Spearman correlation coefficients obtained from comparing the dimensions of the Spanish version of Kiddy-KINDL-R ranged from 0.16 (F1: Physical well-being and F5: Friends) to 0.77 (F5: Friends and Total scale) (Table 5). All the factors showed significant bivariate correlations with each other and with the total scale. Correlations were small and moderate at the p<0.01 level, which suggests that factors are associated with each other but assess different aspects.
Spearman correlations between dimensions (n=283).
| Dimensions | F1 | F2 | F3 | F4 | F5 | F6 | Total |
|---|---|---|---|---|---|---|---|
| 1. Physical well-being | 1 | 0.36** | 0.17** | 0.16** | 0.29** | 0.28** | 0.54** |
| 2. Emotional well-being | 1 | 0.39** | 0.37** | 0.50** | 0.27** | 0.73** | |
| 3. Self-esteem | 1 | 0.32** | 0.48** | 0.37** | 0.68** | ||
| 4. Family | 1 | 0.39** | 0.28** | 0.64** | |||
| 5. Friends | 1 | 0.39** | 0.77** | ||||
| 6. Nursery school/kindergarten | 1 | 0.54** |
F1, physical well-being; F2, emotional well-being; F3, self-esteem; F4, family; F5, friends; F6, nursery school/kindergarten.
We found significant and negative correlations among Kiddy-KINDL-R subscales and most PAS subscales, which were evidence of the divergent validity of the instrument. These results indicate that children with higher HRQoL (as reported by guardians) tended to present fewer symptoms of anxiety disorders (as reported by guardians). The total score of the Kiddy-KINDL-R was significantly and negatively correlated to the total score and all the subscale scores of the PAS (Table 6).
Spearman correlations among Kiddy-Kindl-R and PAS (n=283).
| Kiddy-KINDL-R | PAS | |||||
|---|---|---|---|---|---|---|
| GAD | SAD | OCD | PIF | SP | Total | |
| 1. Physical well-being | −0.22** | −0.20** | −0.18** | −0.08 | −0.10 | −0.10 |
| 2. Emotional well-being | −0.43** | −0.30** | −0.08 | −0.13** | −0.24** | −0.32** |
| 3. Self-esteem | −0.27** | −0.28** | −0.08 | −0.08 | −0.17** | −0.27** |
| 4. Family | −0.44** | −0.26** | −0.20** | −0.14** | −0.27** | −0.37** |
| 5. Friends | −0.37** | −0.30** | −0.08 | −0.08 | −0.18** | −0.29** |
| 6. Nursery school/kindergarten | −0.33** | −0.34** | −0.21** | −0.09 | −0.20** | −0.34 |
| Total score | −0.52** | −0.40** | −0.20** | −0.15** | −0.29** | −0.44** |
Note: PAS=Preschool Anxiety Scale; GAD=generalised anxiety disorder; SAD=separation anxiety disorder; OCD=obsessive-compulsive disorder; PIF=physical injury fears; SP=social phobia.
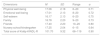
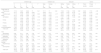
As shown in Table 7, we found no differences in the Kiddy-KINDL-R and PAS scores based on child age or gender, the evaluator or the type of school, except in the scores for social phobia and total anxiety. Children aged 6 years showed more manifestations of social anxiety than children aged 3 years (p=.03; d=0.24). Children attending public schools scored higher in total anxiety compared to those attending private schools (p=.03; d=0.25). Children enrolled in private schools had higher HRQoL scores compared to those enrolled in public schools, but these differences were not statistically significant.
Mean and standard deviation (SD) of Kiddy-KINDL-R and PAS scores by children's age and sex, evaluator and type of school.
| Children's age | Children's sex | Evaluator | School | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 3 | 4 | 5 | 6 | F | Male | Female | t | Mother | Father | Others | F | Public | Private | t | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |||||
| Kiddy-KINDL-R | |||||||||||||||
| Physical well-being | 17.16 (2.17) | 16.81 (2.03) | 16.86 (2.09) | 17 (2.54) | 0.41 | 17.11 (2.24) | 17 (2.11) | 0.40 | 17.08 (2.19) | 17.04 (2.14) | 15.50 (2.12) | 0.52 | 16.83 (2.20) | 17.31 (2.13) | −1.83 |
| Emotional well-being | 17.13 (2.17) | 16.95 (2.32) | 16.65 (1.99) | 17.09 (1.82) | 0.66 | 16.99 (2.09) | 17.03 (2.18) | −0.17 | 16.94 (2.16) | 17.45 (1.92) | 15.50 (0.70) | 1.64 | 16.89 (2.08) | 17.14 (2.18) | −0.95 |
| Self-esteem | 12.20 (2.10) | 11.77 (1.80) | 11.51 (1.90) | 12.04 (2.10) | 1.59 | 11.93 (2.15) | 11.96 (1.84) | −0.12 | 11.97 (2.05) | 11.82 (1.82) | 12 (0) | 0.09 | 11.97 (2.02) | 11.91 (2.00) | 0.22 |
| Family | 16.86 (2.10) | 16.63 (2.63) | 16.92 (2.13) | 16.77 (2.16) | 0.19 | 16.69 (2.23) | 16.89 (2.21) | −0.76 | 16.71 (2.28) | 17.19 (1.88) | 16.50 (2.12) | 0.93 | 16.68 (2.12) | 16.90 (2.32) | −0.83 |
| Friends | 17.12 (2.42) | 17.50 (2.18) | 17.53 (2.03) | 17.90 (1.89) | 1.48 | 17.34 (2.32) | 17.48 (2.05) | −0.56 | 17.31 (2.24) | 17.93 (1.93) | 17 (2.82) | 1.58 | 17.25 (2.27) | 17.57 (2.11) | −1.22 |
| Nursery school/kindergarten | 12.72 (1.62) | 12.68 (1.62) | 12.57 (1.79) | 12.61 (1.67) | 0.10 | 12.61 (1.60) | 12.75 (1.71) | −0.73 | 12.68 (1.68) | 12.67 (1.68) | 12.50 (2.12) | 0.98 | 12.62 (1.67) | 12.74 (1.64) | −0.64 |
| Total score | 88.96 (8.67) | 88.09 (7.82) | 87.75 (7.55) | 89.11 (7.99) | 0.39 | 88.85 (7.88) | 88.85 (7.88) | −0.45 | 88.41 (8.19) | 89.86 (7.77) | 84.50 (3.53) | 0.41 | 88.06 (7.46) | 89.22 (8.75) | −1.20 |
| PAS | |||||||||||||||
| Generalised anxiety disorder | 6.28 (2.65) | 6.14 (2.20) | 6.32 (2.13) | 7.09 (2.55) | 1.47 | 6.26 (2.32) | 6.47 (2.56) | −0.73 | 6.44 (2.52) | 5.82 (1.88) | 8.50 (0.70) | 2.03 | 6.62 (2.43) | 6.06 (2.41) | 1.94 |
| Separation anxiety disorder | 5.36 (2.34) | 5.24 (2.37) | 5.88 (2.06) | 6.11 (1.91) | 1.95 | 5.35 (2.09) | 5.72 (2.36) | −1.39 | 5.85 (2.29) | 4.68 (1.75) | 5 (1.41) | 2.49 | 5.69 (2.32) | 5.34 (2.12) | 1.34 |
| Obsessive-compulsive disorder | 7.46 (3.02) | 7.19 (2.23) | 6.98 (2.34) | 7.29 (2.08) | 1.14 | 7.06 (2.35) | 7.44 (2.80) | −1.22 | 7.21 (2.65) | 7.39 (2.18) | 7 (2.82) | 0.09 | 7.39 (2.72) | 7.07 (2.39) | 1.05 |
| Physical injury fears | 5.68 (2.37) | 5.42 (2.03) | 5.86 (2.24) | 6.22 (2.22) | 0.33 | 5.39 (2.10) | 6.17 (2.36) | −2.93 | 5.79 (2.30) | 5.52 (2.19) | 7 (0) | 0.58 | 5.97 (2.26) | 5.52 (2.25) | 1.66 |
| Social phobia | 8.48 (3.19) | 8.50 (3.34) | 9.30 (3.43) | 10.25 (3.64) | 3.48* | 8.82 (3.35) | 9.05 (3.49) | −0.57 | 9.08 (3.53) | 8.13 (2.68) | 9.50 (2.12) | 1.52 | 9.25 (3.53) | 8.57 (3.25) | 1.69 |
| Total score | 32.28 (10.56) | 34.36 (8.35) | 36.97 (8.33) | 33.90 (9.62) | 2.18 | 32.89 (9.08) | 34.86 (10.05) | −1.73 | 34.20 (9.90) | 31.73 (7.64) | 37 (7.07) | 1.38 | 34.95 (10.06) | 32.57 (8.89) | 2.10* |
PAS=Preschool Anxiety Scale.
The main aim of our study was to examine the factorial structure and psychometric properties of the Kiddy-KINDL-R parents’ version in a sample of Spanish preschool-aged children aged 3–6 years. Confirmatory factor analysis revealed the good fit of the six-factor model proposed by the authors of the original questionnaire,6,18 with values greater than 0.29 and all the items fitting in their corresponding dimensions. Our results were similar to those reported by the authors of studies conducted in Japanese19 and Turkish20 samples, who also found a 6-factor structure in the Kiddy-KINDL parents’ version. Although the structure of the Spanish model is composed of the same 6 dimensions as the original version, in the current study we proposed a new version with 22 items due to the low contribution of the 2 items that were eliminated. Thus, 2 of the 6 factors contain 3 items each, and the others continue to have 4 items each. In spite of this change, the Spanish Kiddy-KINDL structure is consistent with the original scale and suitable for assessing children's HRQoL as reported by parents.
The Spanish version of the Kiddy-KINDL for parents showed an excellent overall reliability, with a Cronbach alpha of 0.90 and adequate internal consistency values that ranged between 0.71 and 0.80, except for the Nursery school/Kindergarten subscale (α=0.58). A possible reason why the internal consistency for the Nursery school/Kindergarten subscale was low is that it had a lower number of items (n=3), combined with the low contribution of item 23. The internal consistency found in our study was higher than the one reported for the original version (Cronbach's α=0.89)18 and the validated versions in Turkey (Cronbach's α=0.84)20 and Japan (Cronbach's α=0.88).19 We assessed the correlations between the scores for individual Kiddy-KINDL-R subscales and between the scores for each subscale and the total score, finding weak to strong correlations (r range, 0.16–0.77; p<.01). Although each dimension refers to a different aspect of HRQoL in children, these values show that the different factors of the questionnaire are related.
To assess discriminant validity, we calculated the correlations between the subscale scores and total scores of the Kiddy-KINDL-R and of the PAS. We found significant negative correlations between the Kiddy-KINDL-R and the anxiety measure, which was evidence in support of the discriminant validity of the questionnaire. We found the highest correlations between the total score of the Kiddy-KINDL and the total score and Generalised anxiety disorder (GAD) and Separation anxiety disorder (SAD) subscales of the PAS, and between the GAD subscale of the PAS and the Emotional well-being and Family subscales of the Kiddy-KINDL. Thus, consistent with our second hypothesis, our results suggest that children with a greater HRQoL (as reported by their parents) are less likely to have anxiety symptoms. In the following stages of the Kiddy-KINDL evaluation process, it would be important to test convergent validity with an equivalent scale validated for this age group in Spain.
In our study, HRQoL and psychiatric morbidity did not vary significantly based on the age or sex or the child, the characteristics of the evaluator or the type of school. However, children enrolled in private schools scored lower in anxiety symptoms compared to those enrolled in public schools. This may be due to children raised in families of higher socio-economic status having fewer risk factors for emotional problems and more resources for healthy development and early detection and treatment of problems.31 Social anxiety symptoms were more prevalent in children aged 6 years compared to the youngest children. The importance that children assign to the perception of others increases with age and peaks in adolescence, a stage when the prevalence of social anxiety disorder is high.32 The mean scores obtained from parental reports in our study revealed a high HRQoL in Spanish pre-schoolers in every area assessed. This was consistent with the original study in a reference sample of German preschool-aged children.33 Although we found high mean scores in each Kiddy-KINDL-R dimension and the total scale, we were unable to establish valid cut-off points because our study was conducted in a community sample. Therefore, it would be interesting to replicate this study with a clinical sample.
This study has several limitations that should be taken into account. The main limitation we were unable to establish causality in the relationships between the variables under study due to its cross-sectional design. Also, the results are based on the information provided by parents about the HRQoL of their children. Obtaining information from other sources would be convenient to further build the evidence supporting the scale. Due to the young age of the assessed subjects, we consider direct evaluation inappropriate, and would instead propose interviewing teachers or using direct observation of children's behaviour as adequate approaches for future research. A second important limitation is that we did not assess test–retest reliability or convergent validity in this study, aspects that should be explored in future studies about the Kiddy-KINDL-R parents’ version. Last of all, we conducted the study in a community sample, so its results may not be generalised to clinical samples.
In short, despite the limitations noted above, the results of our study show that the Spanish parents’ version of the Kiddy-KINDL-R has good psychometric properties, despite the reduction in the number of items compared to the original scale. Our findings confirmed the six-factor structure of the questionnaire, a satisfactory internal consistency, and divergent validity assessed with an external scale for anxiety symptoms. To conclude, validation of the Kiddy-KINDL-R through parent or guardian reports fills an important gap in the evaluation of HRQoL in preschool-aged children in Spain, providing an adequate measuring instrument that could also be useful for assessment in clinical practice.
FundingThis research received financial support from the Ministry of Economy and Competitiveness in Spain (PSI2014-56446-P).
Please cite this article as: Orgilés M, Melero S, Penosa P, Espada JP, Morales A. Calidad de Vida Relacionada con la Salud informada por los padres en preescolares españoles: propiedades psicométricas del Kiddy-KINDL-R. An Pediatr (Barc). 2019;90:263–271.
