



Clinical practice guidelines have been shown to be valuable tools for guiding medical decisions. However, their mere publication has not reduced the variability of practice in terms of the way acute bronchiolitis is managed.
MethodA before-and-after study design was used to analyse the effectiveness of a method of disseminating diagnostic recommendations among physicians regarding the management of infants, hospitalised due to bronchiolitis. Patients with comorbidities, ex-premature patients, and patients transferred to other hospitals were excluded. The diagnostic resources studied were: chest X-ray, full blood count, C-reactive protein, blood culture, venous blood gas, and determination of the respiratory syncytial virus. Eleven epidemic periods were analysed.
ResultsA total of 259 patients were studied including 98 in the pre-intervention group (2006–2010), and 131 in the post-intervention group (2011–2017). The intervention took place in October of 2010 and 2011. A comparison of the two periods showed that the use of chest X-rays dropped from 73.5% to 16% (P<.01), full blood counts from 51% to 21.4% (P<.01), C-reactive protein from 48% to 22.1% (P<.01), and blood cultures from 23.5% to 7.6% (P<.01). Length of stay dropped by 0.6 (SD=1) days and there were no differences in re-admission rates.
ConclusionsThe organised and systematised dissemination, using a multimodal method, of the diagnostic recommendations contained in the clinical practice guidelines on bronchiolitis, is capable of transforming the clinical practice by reducing the use of diagnostic resources, without an increase in the re-admission rate.
Las Guías de Práctica Clínica han demostrado ser herramientas valiosas para orientar las decisiones de los médicos. Su mera publicación no ha reducido la variabilidad en el manejo de la bronquiolitis aguda, y se siguen utilizando de forma excesiva determinados recursos para su atención.
MétodoMediante una investigación con un diseño antes-después, se estudió la efectividad de un método de difusión de recomendaciones diagnósticas para el manejo de lactantes hospitalizados por bronquiolitis. Pacientes con comorbilidades, exprematuros y los que fueron trasladados a otros centros sanitarios fueron excluidos. Los recursos diagnósticos estudiados fueron: radiografía de tórax, hemograma, proteína C reactiva, hemocultivo, gasometría venosa y determinación de virus respiratorio sincitial. Se analizaron un total de 11 temporadas epidémicas.
ResultadosSe estudiaron 259 pacientes, 98 en el periodo preintervención (2006-10) y 131 en el posintervención (2011-17). La intervención se llevó a cabo en octubre de 2010 y 2011. Comparando los dos periodos, disminuyó el uso de radiografía de tórax, 73,5 a 16% (p<0,01); hemograma 51 a 21,4% (p<0,01), PCR 48 a 22,1% (p<0,01) y hemocultivo 23,5 a 7,6% (p<0,01). La duración de la hospitalización disminuyó 0,6 (DE=1) días y no hubo diferencias en los reingresos.
ConclusionesLa difusión organizada y sistematizada, mediante un método multimodal, de las recomendaciones diagnósticas contenidas en una guía de práctica clínica sobre bronquiolitis, es capaz de transformar la práctica médica, reduciendo el uso de recursos diagnósticos, sin incrementarse los reingresos.
Acute bronchiolitis (AB) is an important disease in paediatrics on account on its impact on the health of patients,1 the sharp increase it generates in the demand for services on account of its seasonal patterns at every level of care (primary, emergency and inpatient care)2 and the economic, social and family impact it has past the acute episode.3 Acute bronchiolitis provides a good example of the variability of clinical practice in paediatrics, with numerous studies demonstrating it at the primary care level,4 in emergency departments4,5 and in the management of patients staying in hospital wards4,6 or admitted to paediatric intensive care units.7,8 This variability sometimes entails the overuse of diagnostic and therapeutic resources.9 Clinical practice guidelines (CPGs) are developed with the aim of guiding physicians in making decisions about the management of patients in specific clinical situations.10 Adhering to their recommendations in clinical practice can help reduce the use of interventions that are not backed by high-quality evidence,10 reduce the variability of clinical practice and standardise the care delivered by clinicians, improving patient safety and quality of care.11 It can also result in lower costs for health care systems by increasing their efficiency.3 Studies in the literature show that variability in clinical practice and the excessive use of resources in the management of AB persist despite the publication of CPGs, which highlights a lack of adherence to their recommendations on the part of health professionals.12–15 The aim of our study was to assess whether the implementation of a bronchiolitis CPG using a structured approach to the dissemination of information succeeded in changing the practices of health professionals to improve adherence to the recommendations of the CPG, with the corresponding decrease in the use of diagnostic and therapeutic resources.
Materials and methodsStudy design and population under studyWe conducted a quasi-experimental pre–post intervention study to assess the impact of an educational intervention targeting physicians employed in the paediatrics ward and the emergency department of the Hospital Universitario Virgen de la Luz (HVL, see Appendix A) in regard to their management of infants with bronchiolitis managed first in the emergency department and subsequently admitted to the paediatrics department. We collected data on patient characteristics and other variables prospectively between 2009 and 2017, and retrospectively for the period between 2006 and 2008 through the review of health records of patients aged 12 months or less with a diagnosis of AB based on the International Classification of Diseases Ninth Revision (ICD-9), which corresponds to codes 466.11 and 466.19. We completed the study collecting data for the patients admitted for AB in the 11 epidemic seasons, which we defined as going from October of one year to May of the following year, both included. Thus, our study comprised three clearly defined periods. The pre-intervention period went from October 2006 to October 2010, and the post-intervention period from October 2011 to May 2017, with a transitional period in between that went from October 2010 to October 2011, and that corresponded to the time interval between the two educational interventions. The inclusion criteria were age 12 months of less and admission to hospital with a diagnosis of AB (based on McConnochie criteria adjusted for age).16 We excluded patients born preterm before 35 weeks’ gestation and patients with any of the following diagnoses: haemodynamically significant chronic congenital heart disease; chronic lung disease (pulmonary dysplasia, cystic fibrosis); neuromuscular disease manifesting with hypotonia, such as Down or Prader-Willi syndrome and chronic immunosuppression. We also excluded patients that were transferred for any reason to another facility during their hospitalisation.
InterventionWe performed 2 interventions 1 year apart, one in October 2010 and another in October 2011. The recommendations given in the intervention were based on the acute bronchiolitis CPG of the American Academy of Pediatrics17 and Spanish publications from later dates.18,19Appendix B presents the organisation, content and aim of these recommendations.
VariablesWe started data collection for the variables of interest in October 2009, using a form designed specifically for that purpose. Starting from this season, we collected data prospectively in each of the seasons. In addition to data on demographic variables, we collected data on the primary outcomes, the variables associated with the use of diagnostic resources and which could be subject to change, which were the following: performance of plain chest X-ray, collection of blood sample for analysis (complete blood count (CBC), C-reactive protein (CRP) levels and venous blood gases), collection of blood sample for culture, and respiratory syncytial virus (RSV) test for detection of viral fusion protein antigen in nasal secretions by the membrane chromatographic immunoassay method. The secondary outcomes were the length of stay and the readmission rate. We defined readmission as an episode requiring admission within 10 days from the previous discharge.
Statistical analysisTo determine whether educational interventions led to a decreased use of resources, we compared the pre-and post-intervention percentages of patients in whom the diagnostic tests listed above were used. We summarised qualitative variables by means of absolute frequencies and percentages and assessed changes in them by means of the chi square test. We summarised normally distributed quantitative variables as mean and standard deviation (SD) and assessed changes in them by means of the Student t test. For quantitative variables that did not follow a normal distribution, we used the median and interquartile range for their description, and the Mann–Whitney U test for their comparison. We used the software Epidat 3.0 to calculate the sample size required for comparison of unpaired measures in different groups with an alpha level (risk of type I error) of 0.05 and an absolute precision of ±5% in two-sided tests, assuming a baseline proportion of events (order of plain chest X-ray for diagnosis of AB) of 0.6 and a final proportion of 0.2, and obtained a size of 34 participants. The statistical analysis was performed with the software SPSS for Windows version 21.0 (SPSS Inc, Chicago, Illinois, United States).
Ethical considerationsThe study protocol was approved by the Clinical Research Ethics Committee of the HVL on February 15, 2011. We adhered to the principles of the Declaration of Helsinki and the Organic Law 15/99 for the Protection of Personal Data at all times during data collection, processing and analysis, and in every instance that we interacted with the families for purposes related to the study.
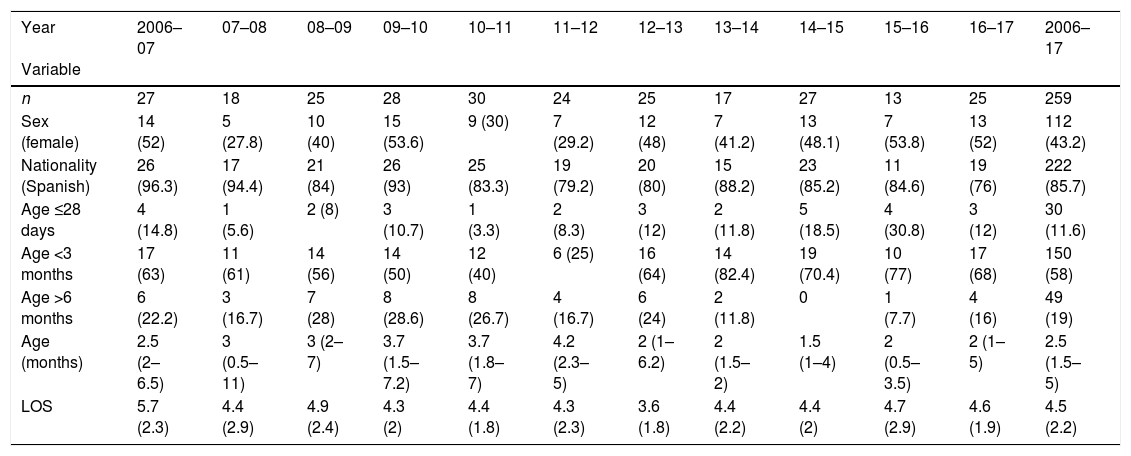
ResultsDuring the entire period under study, from October 2006 through May 2017, we initially included a total of 277 patients admitted during the 11 epidemic seasons. Of this total, we excluded 18 because they did not meet the inclusion criteria, so the final sample comprised 259 patients. Of these patients, 98 corresponded to the pre-intervention period (4 epidemic seasons, 2006–2010) and 131 to the post-intervention period (6 epidemic seasons, 2011–2017) (Fig. 1). The median age of the patients in the sample was 2.5 months (IQR, 1.5–5), with a predominance of the male sex (56.8%). As can be seen in Table 1, patients admitted for AB in the post-intervention period were younger compared to previous years. The mean length of stay of patients in the pre-intervention period was of 4.9 days (SD, 2.4), which was longer compared to the mean stay of the entire post-intervention group, of 4.3 days (SD, 2.1), although this difference was not statistically significant (P=.09). Table 1 presents these and other demographic characteristics of the sample. We found no differences between the periods in the frequency of readmission: there were 2 readmissions in the pre-intervention period and another 2 in the post-intervention period.

Demographic characteristics of patients included in the study.
| Year Variable | 2006–07 | 07–08 | 08–09 | 09–10 | 10–11 | 11–12 | 12–13 | 13–14 | 14–15 | 15–16 | 16–17 | 2006–17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 27 | 18 | 25 | 28 | 30 | 24 | 25 | 17 | 27 | 13 | 25 | 259 |
| Sex (female) | 14 (52) | 5 (27.8) | 10 (40) | 15 (53.6) | 9 (30) | 7 (29.2) | 12 (48) | 7 (41.2) | 13 (48.1) | 7 (53.8) | 13 (52) | 112 (43.2) |
| Nationality (Spanish) | 26 (96.3) | 17 (94.4) | 21 (84) | 26 (93) | 25 (83.3) | 19 (79.2) | 20 (80) | 15 (88.2) | 23 (85.2) | 11 (84.6) | 19 (76) | 222 (85.7) |
| Age ≤28 days | 4 (14.8) | 1 (5.6) | 2 (8) | 3 (10.7) | 1 (3.3) | 2 (8.3) | 3 (12) | 2 (11.8) | 5 (18.5) | 4 (30.8) | 3 (12) | 30 (11.6) |
| Age <3 months | 17 (63) | 11 (61) | 14 (56) | 14 (50) | 12 (40) | 6 (25) | 16 (64) | 14 (82.4) | 19 (70.4) | 10 (77) | 17 (68) | 150 (58) |
| Age >6 months | 6 (22.2) | 3 (16.7) | 7 (28) | 8 (28.6) | 8 (26.7) | 4 (16.7) | 6 (24) | 2 (11.8) | 0 | 1 (7.7) | 4 (16) | 49 (19) |
| Age (months) | 2.5 (2–6.5) | 3 (0.5–11) | 3 (2–7) | 3.7 (1.5–7.2) | 3.7 (1.8–7) | 4.2 (2.3–5) | 2 (1–6.2) | 2 (1.5–2) | 1.5 (1–4) | 2 (0.5–3.5) | 2 (1–5) | 2.5 (1.5–5) |
| LOS | 5.7 (2.3) | 4.4 (2.9) | 4.9 (2.4) | 4.3 (2) | 4.4 (1.8) | 4.3 (2.3) | 3.6 (1.8) | 4.4 (2.2) | 4.4 (2) | 4.7 (2.9) | 4.6 (1.9) | 4.5 (2.2) |
Each column corresponds to an epidemic season, starting with season 2006–07 and ending in season 2016–17. The rightmost column refers to all the patients included in the study. We have expressed qualitative variables as absolute frequencies and percentages. Since the quantitative variable age did not follow a normal distribution, we have expressed it using the median and interquartile range. We have expressed the length of stay (LOS) as mean and standard deviation.
n: number of cases of acute bronchiolitis with admission to hospital in each epidemic season.
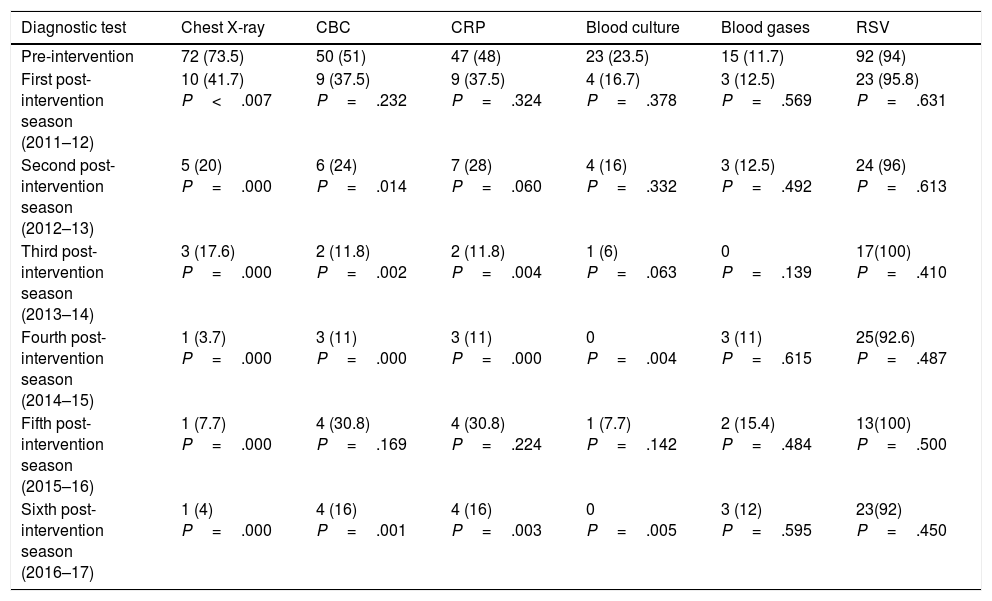
When we compared the percentage of patients in whom specific resources were used in the pre-intervention and transition periods, we found that the only resource in which there had been a reduction was the chest radiograph, as can be seen in Fig. 2. However, when we compared the pre-intervention group with the post-intervention group, we found reductions in the use of every resource targeted in the intervention. This trend was observed both in the comparison of the two periods overall (Fig. 3) and in the comparison of the use of resources year by year after the intervention (Table 2). Thus, we see a shift from the near-routine performance of a chest X-ray in 73.5% of infants admitted with AB to performance of X-rays in only 3.7%, 7.7% and 4% of these patients in years 4, 5 and 6 after the 2-step educational intervention. We found a similar pattern in the use of other diagnostic resources, including the CBC, measurement of CRP levels and blood culture. However, we did not find any reduction in the use of other tests, such as blood gases and detection of RSV in nasal secretions. Last of all, we ought to highlight that the use of some resources started increasing again several years after the 2-step educational intervention, specifically in the 2015–16 seasons, that is, 5 years after the implementation of the CPG.


Frequency of use of diagnostic resources in the pre-intervention period compared to the post-intervention period.
| Diagnostic test | Chest X-ray | CBC | CRP | Blood culture | Blood gases | RSV |
|---|---|---|---|---|---|---|
| Pre-intervention | 72 (73.5) | 50 (51) | 47 (48) | 23 (23.5) | 15 (11.7) | 92 (94) |
| First post-intervention season (2011–12) | 10 (41.7) P<.007 | 9 (37.5) P=.232 | 9 (37.5) P=.324 | 4 (16.7) P=.378 | 3 (12.5) P=.569 | 23 (95.8) P=.631 |
| Second post-intervention season (2012–13) | 5 (20) P=.000 | 6 (24) P=.014 | 7 (28) P=.060 | 4 (16) P=.332 | 3 (12.5) P=.492 | 24 (96) P=.613 |
| Third post-intervention season (2013–14) | 3 (17.6) P=.000 | 2 (11.8) P=.002 | 2 (11.8) P=.004 | 1 (6) P=.063 | 0 P=.139 | 17(100) P=.410 |
| Fourth post-intervention season (2014–15) | 1 (3.7) P=.000 | 3 (11) P=.000 | 3 (11) P=.000 | 0 P=.004 | 3 (11) P=.615 | 25(92.6) P=.487 |
| Fifth post-intervention season (2015–16) | 1 (7.7) P=.000 | 4 (30.8) P=.169 | 4 (30.8) P=.224 | 1 (7.7) P=.142 | 2 (15.4) P=.484 | 13(100) P=.500 |
| Sixth post-intervention season (2016–17) | 1 (4) P=.000 | 4 (16) P=.001 | 4 (16) P=.003 | 0 P=.005 | 3 (12) P=.595 | 23(92) P=.450 |
We have compared each epidemic season in the post-intervention period with the entire pre-intervention group, which comprises every infant admitted with bronchiolitis between October 2006 and May 2010 (4 epidemic seasons).
CBC, complete blood count; CRP, C-reactive protein; RSV, respiratory syncytial virus.
Clinical practice guidelines are among the most important tools developed to improve the quality and efficiency of health care, translating rigorous scientific evidence into measures that have clinical impact.20 Our study demonstrated that the dissemination of knowledge in health care institutions through a structured approach using direct, repeated and multimodal interventions addressed to physicians, with presentation of indicators of the quality of the care currently delivered and emphasising the specific aspects where modifications were being pursued, can achieve a sustained reduction in the use of diagnostic resources that are not recommended by CPGs,17–19 such as chest radiography, CBC, CRP measurement and blood culture, without a concomitant reduction in the use of resources not targeted in the intervention, such as venous blood gases and detection of RSV in nasal secretion samples. In addition to this reduction in the use of diagnostic resources, we also observed a decrease in length of stay in our patients, although the study design did not allow us to establish causality for this association. This reduction in the use of diagnostic resources and the associated decrease in the length of stay did not result in an increased readmission rate during the post-intervention period.
An interesting finding in our study was that while an initial intervention was implemented in October 2010, we did not start observing the desired effects until the intervention was repeated and feedback provided a year later, in October 2011. The effects did not only exceed those observed in other research projects that assessed the impact of the publication of CPGs without further intervention,14,15,21,22 but were also superior to those obtained with other structured interventions with dissemination of the evidence included in CPGs through a multimodal approach and with specific goals. Such is the case of the study by Mittal et al., where CPG implementation achieved a reduction in the use of chest X-rays from 59.7% to 39%, a significant difference, although smaller than the one observed in our study,23 or the study of Ralston et al., which found a decrease in the use of this resource of 36% compared to the pre-intervention period.24
Some of the reasons that physicians do not adhere to the recommendations of CPGs include lack of awareness of their existence, lack of familiarity with their use in actual practice, the excessive length and complexity of the CPG documents, lack of time to devote to the individual reading and summarising of their contents, disagreement with some of their recommendations, negative expectations regarding the clinical outcomes of their application, internal and external institutional barriers that impede their implementation on a large scale and difficulty overcoming the inertia of habit and continuing to deliver care using the approach learned during medical education and practiced for several years.25–27
On the other hand, to our knowledge there are no reports in the literature of the waning of the beneficial effects obtained with the implementation of CPGs. This may be because other studies in the literature did not have long follow-up periods, unlike our study. Our hypothesis is that this type of intervention requires regular reinforcements, and after the 2-step intervention we have described, there were no others. Also, there were no substantial changes in the medical staff of the clinical departments that participated in the study that would explain the increase in the use of some of the diagnostic resources that followed the initial reduction. However, further research focused on this phenomenon would be necessary to obtain a plausible explanation.
Some of the strengths of our study are that it had a prospective design for the majority of its duration, which allowed the assessment of outcomes at regular intervals and therefore implementation of corrective measures where needed, and that it analysed 11 epidemic seasons, with prospective follow-up in 8 of them, which we consider a long-term follow-up.
We believe that among the measures implemented in pursuit of our objectives, the one that may have had the greatest impact could be having made the physicians in the emergency setting the main target of our intervention, as the ordering of the initial diagnostic tests has always been their responsibility. We believe that having designed an educational intervention particularly targeted to them, providing them with a summary of the management protocol, and informing them of the outcomes of the assessment of the use of resources before and after the first intervention (October 2010) as positive feedback for their clinical practice were crucial to the success of the project.
Although this does not constitute a strength of our study, we would like to highlight the considerable difference in the number of chest radiographs performed before and after the 2-step intervention in the absence of negative consequences such as increases in misdiagnosis or readmission, which increased patient safety in our infant population by reducing their exposure to ionising radiation.
However, one limitation of our study was its small sample size, which was due to the small size of the paediatric population in the catchment area of our hospital.
Another aspect to consider is that the success of our project may have been due, at least in part, to the small size of the health care teams that manage AB in our hospital, both in the emergency department and in the paediatrics ward. This small size favours the development of closer interprofessional relationships and facilitates the attendance of a larger proportion of physicians to educational activities. For this reason, it may not be possible to generalise the results of our study to large-scale hospitals with much larger staffs. Nevertheless, and considering the favourable outcomes of our intervention, we propose that similar interventions be implemented in hospitals and primary care centres in Spain in order to assess their effectiveness in improving efficiency in the management of acute bronchiolitis at every level of care.
ConclusionThe dissemination of the scientific evidence published in CPGs by a structured, multimodal, and direct approach addressed to physicians, setting specific goals and repeatedly providing positive feedback, can achieve a reduction in the use of diagnostic resources in the management of AB that have been specifically targeted in the intervention, such as chest X-rays, CBCs, CPR tests and blood culture without an associated increase in the readmission rate in small and mid-sized hospitals. These interventions can increase the efficiency of health care facilities, which will in turn be able to offer safer and higher-quality care to their patients.
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank Luigi Álvarez Burneo for his help in the tabulation of the research data, Sara Hernández and Alberto de la Osa for their help in data collection, and also Susana Losada, Eneida del Olmo, Araceli Molina, Carlos Molina, Ruth Toledo, Carlos Herráiz, Gregorio Garde, Pablo Franquelo, Juan Ramón Toledo, Félix González, Alicia Panadero, David García, Luís Fernández, Piluca Redondo, Juan Ballesta, Fidel Mora, Francisco Pulido, Cesar Canales, Alicia Panadero, Silvia Yangües, Diana Moya and Emilio Camacho for their excellent management of the patients that participated in the study. We also thank all the resident physicians that, during these 11 years, contributed with their work and their learning to the successful completion of this project. Last of all, we thank José Antonio Nieto for his advice on the statistical analysis of the data, and Rosa Josefina Bertolín Bernades for helping us complete this project.
Characteristics of Hospital Virgen de la Luz (HVL) in Cuenca.
Hospital Virgen de la Luz is the only public hospital in the province of Cuenca and serves a catchment population of approximately 12500 patients aged 0–14 years. The initial management of patients with AB that seek care in hospital, including decisions about diagnostic procedures and treatment, is carried out by family physicians in the emergency department. Approximately 100–150 cases of AB are managed in total in the emergency department of the HVL each year, resulting in a mean of 24 admissions per year. The health care team involved in the overall hospital care of patients with AB includes 22 emergency physicians, 43 emergency nurses and nurse assistants, 14 orderlies, 10 paediatricians and 15 paediatric nurses and nurse assistants.
Multimodal intervention for dissemination of information related to the approach to the diagnosis of AB in the HVL.
Intervention 1, October 2010:
- (a)
Clinical consensus session for physicians from the Department of Paediatrics of 45 minutes’ duration.
- (b)
Joint clinical consensus session for physicians from the Department of Paediatrics and the Emergency Department of 45 minutes’ duration.
The contents of both informational sessions, based on the recommendations of the CPG published by the American Academy of Pediatrics in 2006,17 focused on AB being a clinical diagnosis in which performance of chest X-rays or blood tests such as a CBC, CRP levels and blood culture is not recommended to rule out other aetiologies.
The information in both sessions was delivered by the coordinator of the project.
Intervention 2, October 2011:
- (a)
Joint clinical consensus session for the Department of Paediatrics, the Department of Radiological Diagnosis and the Emergency Department of 45 minutes’ duration. Training delivered by the coordinator of the project. This second session reinforced the specific recommendations promoted in 2010 and also introduced the recommendations of 2 recent Spanish publications of a similar nature.18,19 The representatives of the Emergency Department were given a written protocol summarising these recommendations and the situations in which ordering an X-ray should be considered (see Appendix C). Data on the use of diagnostic resources in the first year following Intervention 1 (October 2010) were presented and compared with the use in the pre-intervention period, with the purpose of positively reinforcing the recommendations and correcting current practices. Last of all, physicians were urged to permanently implement the suggested changes in their daily practice. Furthermore, physicians in the Emergency Department were made aware that they played a key role in achieving the project goals.
Clinical situations that may warrant the request of a chest radiograph in a patient with acute bronchiolitis.
- 1.
Measured fever >38.5°C lasting more than 12h.
- 2.
Significant worsening of respiratory distress.
- 3.
Focal hypoventilation as a possible sign of pulmonary consolidation.
- 4.
Cases of acute bronchiolitis that meet the following severity criteria:
- a.
Lethargy.
- b.
History of apnoeic episodes.
- c.
Nasal flaring, severe intercostal retractions, wheezing or cyanosis.
- a.
Please cite this article as: Maraña Pérez AI, Rius Peris JM, Rivas Juesas C, Torrecilla Cañas J, Hernández Muelas S, de la Osa Langreo A. Implementación multimodal de una guía de práctica clínica en bronquiolitis: acabando con el uso excesivo de recursos diagnósticos. An Pediatr (Barc). 2018;89:352–360.
