






In recent years, there have been changes in the management of patients with primary immune thrombocytopenia. In this study, a review is presented of the characteristics and outcomes of children with primary immune thrombocytopenia in a children’s hospital (Hospital Infantil Niño Jesús). Moreover, an analysis is made of the changes in the care of these patients diagnosed before and after 2011, when new guidelines were published by the Spanish Society of Paediatric Haematology Oncology (SEHOP).
Material and methodsData from a cohort of primary immune thrombocytopenia patients followed up in this hospital have been retrospectively reviewed. The statistical package used for the analysis was SPSS Statistics 22.0 (IBM Corp., Chicago, IL, USA).
ResultsA review is presented on the clinical data from 235 paediatric patients diagnosed with primary immune thrombocytopenia. It was observed that some features at diagnosis, such as age younger than five years and a previous history of infection, influenced the probability of cure. Regarding the changes in the management of patients since 2011, the steroid doses received during the first month and the first year, and the number of days corresponding to the patient’s first admission have both significantly decreased. Splenectomies were also significantly reduced.
ConclusionsSince 2011, there have been changes in the medical care of our primary immune thrombocytopenia patients: they receive lower doses of steroids, they stay fewer days in the hospital, and the number of splenectomies has decreased without increasing bleeding or worsening the clinical evolution. Furthermore, it was observed that age younger than 5 years and a history of infection prior to diagnosis were related to higher chances of recovery.
En los últimos años se han experimentado cambios en el manejo de los pacientes con trombocitopenia inmune primaria. En este estudio se revisan las características de los pacientes con trombocitopenia inmune primaria del Hospital Infantil Universitario Niño Jesús y su evolución. Además, analizamos los cambios en el abordaje de los pacientes diagnosticados antes y después del 2011, año en el que se publicó la guía de la Sociedad Española de Pediatría.
Material y métodosSe han revisado retrospectivamente los datos de pacientes con trombocitopenia inmune primaria en seguimiento en nuestro hospital desde el año 2000. El paquete estadístico utilizado para el análisis fue SPSS Statistics 22.0 (IBM Corp, Chicago, IL, EE.UU.).
ResultadosSe han revisado 235 pacientes pediátricos con trombocitopenia inmune primaria observando que algunas características al diagnóstico, como la edad menor de 5 años y los antecedentes previos de infección, pueden influir en la probabilidad de recuperación. Con respecto al cambio de manejo de los pacientes, a partir de 2011 las dosis de esteroides recibidas durante el primer mes y el primer año se han reducido de forma significativa, así como el número de días del primer ingreso pasando de 5 a 3 días. Las esplenectomías también se han reducido significativamente.
ConclusionesDesde el año 2011 se han producido cambios en el abordaje de nuestros pacientes: reciben una menor dosis de esteroides, permanecen menos días ingresados y se ha reducido el número de esplenectomías sin aumentar los sangrados y sin disminuir la tasa de respuestas. Además, observamos que la edad menor de 5 años y el antecedente de infección previa al diagnóstico están relacionados con una mayor tasa de recuperación.
Primary immune thrombocytopenia, previously known as idiopathic or immune thrombocytopenic purpura (ITP), was renamed in 2009, when the ITP international working group published guidelines for the Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children. They eliminated the term purpura because bleeding symptoms are absent or minimal in many cases, but recommended preserving the acronym ITP (which would stand for immune thrombocytopenia) due to its widespread use.1
In addition to changing the name of ITP, several updates have been introduced in domestic and international guidelines. The revised guidelines of 2009 established a platelet count threshold of 100 × 109/L for diagnosis of ITP due to the high frequency of counts between 100 and 150 × 109/L in healthy individuals. The criteria for classification based on duration were revised, since there is a high probability of remission in children within 3 to 12 months, so that chronic ITP was defined as disease lasting more than 12 months. This was followed by the publication of the international consensus report on the investigation and management of primary immune thrombocytopenia in 2010.2 One of the key concepts introduced in this consensus was the importance of achieving an adequate quality of life while minimising the toxicity of treatment.
There is a very large International ITP Registry and many research projects are devoted to the disease, but clinical data in paediatrics is not as abundant. Several aspects have long been under debate and are unlikely to be settled unless large-scale studies are conducted on paediatric patients.2
In 2011, the Sociedad Española de Hematología y Oncología Pediátrica (Spanish Society of Paediatric Haematology and Oncology, SEHOP) published new guidelines for the diagnosis and treatment of ITP,3 but there have been no studies since analysing whether the publication of these guidelines has had any impact on the management of these patients. Furthermore, there has been no assessment of whether changes in management, if they have occurred, have resulted in complications or improved outcomes in children with ITP.
The aim of our study was to perform a retrospective review of the clinical characteristics of paediatric patients with ITP managed in our hospital and analyse changes in the management of cases diagnosed before and after 2011, the year the new guidelines were published. We analysed several variables and made comparisons to determine whether there have been benefits to patients after the publication of the guidelines without an associated increase in the incidence of complications. We also considered previous guidelines from 1994 and 2004 as reference, in addition to the guidelines published by the American Society of Hematology (ASH)4 that were being applied at the time of the publication of the new SEHOP guidelines in 2011.
Material, sample and methodsWe performed a retrospective review of the health records of 235 patients with a diagnosis of ITP that had been assessed or managed, intermittently or regularly, at the Hospital Infantil Universitario Niño Jesús (HIUNJ) from January 2000. The study was approved by the Ethics Committee of the HIUNJ. We collected data on the following variables for each of the identified cases of ITP:
- •
Patient-related variables: sex, date of birth and personal history of autoimmune disease.
- •
Diagnosis-related variables: date of diagnosis, history of infection or vaccine administration, disease onset, presence and type of bleeding episodes at diagnosis, blood count values at diagnosis, serological testing, antinuclear antibody (ANA) test and titre in case of a positive result and quantitative measurement of serum immunoglobulin levels (IgG, IgA, IgM).
- •
Treatment-related variables: performance of bone marrow aspiration, hospital admission at diagnosis, length of stay in case of admission at diagnosis, prescription treatment and type of treatment used.
- •
Outcome variables: treatment received in the first month following diagnosis and steroid dose during this period; steroid dosage and cycles of intravenous immunoglobulin received in the first year of follow-up; types of bleeding identified in the first year of follow-up, number of bleeding episodes, severe bleeding, platelet count at 6 months, 1 year and 2 years after diagnosis; most recent platelet count, date when patients had a platelet count greater than de 100 × 109/L after 1 month without treatment. In case splenectomy was performed, we collected the date of the surgical intervention.
We classified bleeding into 4 categories: absence of bleeding, cutaneous bleeding, mucosal or mucocutaneous bleeding and severe bleeding. Severe bleeding was defined as bleeding requiring additional intervention. We defined resolution of disease as a platelet count greater than 100 × 109/L sustained in the absence of treatment. In the analysis, we censored cases managed with splenectomy as absences of the event of interest (a platelet count above the established threshold) until the date of the surgery. We considered patients that did not achieve platelet counts greater than 100 × 109/L after 1 year of follow-up cases of chronic ITP.
We analysed all study variables to identify differences between the periods until and from 2011, the year that the SEHOP published the protocol for the investigation and management of ITP.
The statistical analysis was performed with the software SPSS Statistics versions 15.0 and 22.0 (IBM Corp., Chicago, IL, USA). We have summarised qualitative variables as frequency distributions. We have expressed quantitative variables with a normal distribution as mean and standard deviation. We assessed the normality of the distribution with the Kolmogorov-Smirnov test. For normally distributed variables, we used the Student t test in case of dichotomous variables and analysis of variance (ANOVA) in case of categorical variables with 3 or more categories.
We expressed variables without a normal distribution as median and range and compared them using nonparametric tests: the Mann–Whitney U test in case of dichotomous variables and the Kruskal–Wallis test otherwise.
When we obtained significant results in the ANOVA in non-dichotomous variables with a normal distribution, we used the post hoc Bonferroni test to identify which groups differed from one another. We compared qualitative variables using contingency tables and the chi square test. We assessed the risk associated with predictors by calculating the odds ratio with the corresponding confidence interval. We used the Kaplan–Meier method to calculate the cumulative incidence of the different factors under study, and the log-rank test to compare the incidence curves of different populations based on those factors.
ResultsCharacteristics of patients at diagnosisWe identified 235 patients given a diagnosis of ITP starting in 1991 managed at the HIUNJ at some point from January 2000. The median age of the sample was 4 years (3 months -17 years). The male-to-female ratio was 1.12 (124 male and 111 female). The difference was greater before age 5 years, with a ratio of 1.39, and was inverted after age 9 years, with a ratio of 0.69.
A total of 215 patients (92.3%) presented with some form of bleeding at diagnosis. In 129 patients (55.4%) bleeding was restricted to cutaneous manifestations, 80 had mucosal bleeding (34.3%) and only 6 (2.6%) had other forms of bleeding. Seven patients (3%) had a previous history of autoimmune disease and therefore could have had secondary immune thrombocytopenia. The most frequent autoimmune disease was hyperthyroidism (4 cases). The onset was acute in 204 cases (87.5%) and insidious in 29 cases (12.5%). In 114 patients (48.5%), the diagnosis was preceded by an infectious disease or administration of a vaccine.
Bleeding episodes in the first year of follow-upIsolated bleeding at the skin level was the most frequent type of bleeding detected in the first year of follow-up. There were only 12 patients (5.5%) that did not experience any form of bleeding during this period. The maximum number of episodes in this timeframe corresponded to one patient that experienced a total of 8. Eighteen patients (7.6%) experienced episodes of severe bleeding. Two of them experienced intracranial bleeding, which resolved without complications in both (Table 1).
Severe bleeding episodes in the first year of follow-up. Percentage of total sample.
| Type | n | % |
|---|---|---|
| Severe epistaxis | 9 | 3.8 |
| Severe epistaxis and transfusion | 2 | 0.85 |
| Intracranial haemorrhage | 2 | 0.85 |
| Haematuria | 2 | 0.85 |
| Gastrointestinal haemorrhage | 1 | 0.425 |
| Haematuria and epistaxis | 1 | 0.425 |
| Haemothorax | 1 | 0.425 |
The median time elapsed before reaching a platelet count of 100 × 109/L was 3.84 months (range, 0.12–174.72) (Fig. 1A). Only 2 variables were significantly associated with the probability of resolution: a history of recent infection at the onset of disease (Fig. 1B) and age less than 5 years (Fig. 1C).
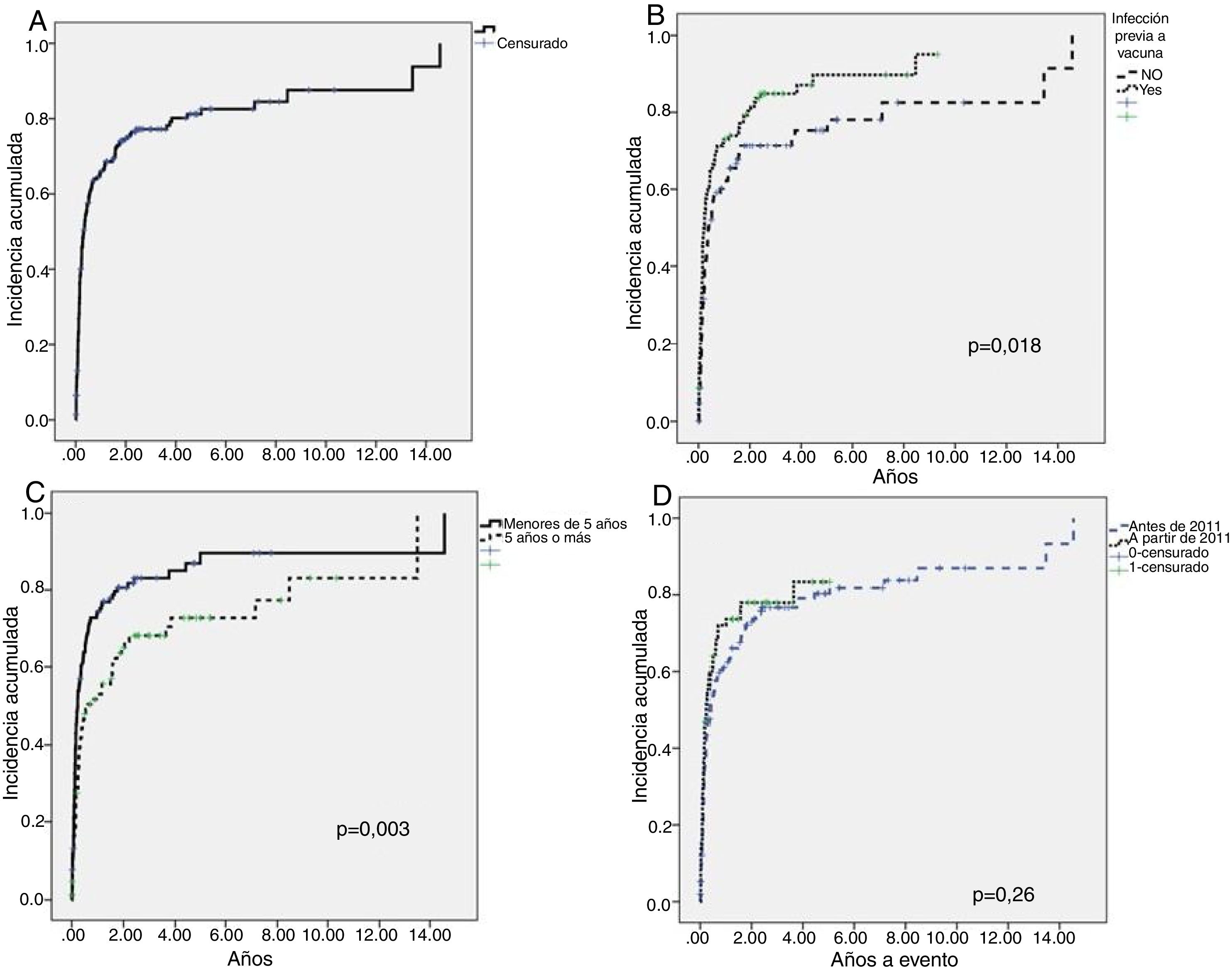
Course of disease in patients until reaching a platelet count greater than 100 × 109/L (resolution).
A) Cumulative incidence curve for the entire cohort. Median time elapsed to resolution, 3.84 months. B) Log-rank test comparing groups based on the presence or absence of a history of recent infection or vaccination. The median time to resolution was different in patients with a history of infectious disease or vaccination (0.23 years or 2.76 months) compared to those without such history (0.38 years or 4.56 months) (P = 0.018). C) Log-rank test comparing age groups. The median time elapsed to resolution was different in patients aged less than 5 years (0.23 years or 2.76 months) compared to patients aged more than 5 years (0.62 years or 7.44 months) (P = 0.003). D) Log-rank test comparing cohorts in the two time periods, without significant differences between the groups.
The multivariate analysis found a significant association of these two variables with the probability of reaching a platelet count greater than 100 × 109/L. Patients with a history of recent infection or vaccination were 1.36 more likely to exceed the threshold of 100 × 109 platelets/L than patients without such history at diagnosis (1–1.185; P = 0.05). Patient under 5 years were 1.58 more likely to reach the platelet count threshold compared to older patients (1.14–2.18; P = 0.005).
For the purpose of the analysis of the final outcomes, 22 cases were lost to follow-up. A total of 155 patients achieved resolution without splenectomy. Another 16 underwent splenectomy, of who 62.5% (10 patients) were considered cured. Of the patients that underwent splenectomy, 15 received the diagnosis before 2011, compared to a single patient that underwent splenectomy since 2011, with a clear difference between both periods (P = 0.04).
Differences in management between the periods under studyWe did not find statistically significant differences in the demographic characteristics or the complete blood count values between the 166 patients managed before 2011 and the 69 patients that received the diagnosis from that year on.
There were differences in the tests performed in each period, with an increased frequency of serological testing, measurement of serum immunoglobulin and ANA tests in patients given a diagnosis starting in 2011 (Table 2).
The frequency of bone marrow aspiration remained stable. Before 2011, it was performed in 82.9% of patients (136/164), and from 2011 in 79.4% (54/68) (P = 0.53).
We did not find differences between the 2 periods in the presence of bleeding at diagnosis or the types of bleeding. We also found no differences in the percentage of patients receiving treatment at diagnosis or the type of treatment received in the first week or the first month of follow-up.
When it came to treatment in the first year from diagnosis, we found no difference in the number of intravenous immunoglobulin cycles, but we did find a significant difference in the steroid dosage in the first month and the first year from diagnosis, which was lower since 2011 (Table 3).
Variables related to steroid therapy and initial length of stay by period in which the diagnosis was made.
| Variables | Until 2011 | From 2011 | P |
|---|---|---|---|
| Steroid dose in the first month (mg/kg) | n = 88 | n = 36 | 0.001 |
| 495 (4–150) | 10 (2–50) | ||
| Steroid dose in the first year (mg/kg) | n = 91 | n = 41 | 0.001 |
| 53 (4–414) | 16 (2–105) | ||
| Length of stay in initial admission (days) | n = 143 | n = 56 | 0.001 |
| 5 (1–28) | 3 (1–14) |
There was also no difference in the proportion of patients that were admitted at diagnosis, but there was a difference in the length of stay of the initial admission, with a median of 5 days until 2011 and a median of 3 days since 2011 (P = 0.001) (Table 3).
We found no difference in the development of chronic ITP between the two time periods. In the first period, 29.5% of patients developed chronic disease compared to 21.7% in the second period (P = 0.13). There were also no significant differences in the cumulative incidence curve of platelet counts greater than 100 × 109/L (cure) between the 2 cohorts (Fig. 1D).
There were also no differences in the number of bleeding episodes (P = 0.92) or the incidence of severe bleeding in the first year of follow-up. There were 12 episodes of severe bleeding diagnosed in the first period compared to 6 in the second period (P = 0.84).
DiscussionPrimary immune thrombocytopenia is the most frequent form of thrombocytopenia in previously healthy children. Several guidelines and protocols have been published with the aim of standardising the diagnosis and management of paediatric patients with ITP. However, in most instances, studies have not been performed to assess whether updated protocols improve outcomes or quality of life in these patients.
After the 2011 update of the guidelines for the management of patients with ITP, we were able to identify 2 main changes that had a positive impact on patients: a decrease in the dosage of steroids and a reduction of the initial hospital stay. To arrive to this conclusion, we analysed retrospective data on patients with ITP managed at the HIUNJ since 2000. We compared the care and outcomes of these patients before and after the publication of the 2011 guidelines. Such retrospective studies are very useful to determine whether the implementation of the changes recommended in new diagnosis and management guidelines is beneficial to the patients.
The general characteristics of the patients in the sample were consistent with the findings of other paediatric case series.5 Most patients received the diagnosis of ITP before age 9 years. There was a mild predominance of the male sex in the group under 5 years (male:female ratio, 1.39), a distribution that became inverted in patients aged more than 9 years, with a greater frequency in girls (male:female ratio, 0.69). These ratios were similar to those described by other authors.6,7 Most patients in our series (87.5%) had a sudden onset, with a percentage that was similar to the percentage found in previous studies.8,9 We did not find significant differences compared to other case series in the frequency or severity of bleeding, and cutaneous bleeding was the most common type at diagnosis. In our study, we also observed that age less than 5 years and a history of recent infection before diagnosis were associated with a higher frequency of recovery.
Primary immune thrombocytopenia is a diagnosis of exclusion, so the history-taking and diagnostic tests performed in the initial evaluation are important. However, there is no clear evidence on which tests should be performed routinely in the diagnostic evaluation besides the complete blood count and peripheral blood smear. Some tests may provide information regarding the underlying aetiology or help make an accurate differential diagnosis at an early stage. In this sense, there has been an increase in the performance of additional tests, such as serological tests, quantitative immunoglobulin tests and ANA test since 2011. These tests are important for ruling out other autoimmune diseases, such as systemic lupus erythematosus, and to assist in the differentiation between primary and secondary immune thrombocytopenia. In our sample, the proportion of patients that underwent bone marrow aspiration was similar before and after 2011. This may be due to the maintenance of the existing indication for performance of this test, chiefly in patients with atypical thrombopenia and for the main purpose of ruling out leukaemia. We ought to note that bone marrow aspiration is not required for diagnosis of classic ITP. In our hospital, this test was performed in a large proportion of patients due to its availability and the vague definition of classic or typical ITP. One relevant aspect that could be addressed in future updates of the guidelines would be establishment of clear criteria to differentiate classic from atypical ITP, as it was not addressed in the most recent guideline of the SEHOP.10 Furthermore, health providers should carefully review the criteria used to define the indication of bone marrow aspiration to avoid subjecting patients to this procedure when it is not necessary.
We did not find a significant decrease in the proportion of children admitted to hospital at the time of diagnosis after 2011. Admissions did not decline despite an improved understanding of the disease and the low incidence of severe complications. However, we did find a significant reduction in the length of the initial hospitalization, with a median stay of 5 days before 2011 compared to 3 days thereafter. This is a small difference that could have an impact on the quality of life of patients and their families by reducing the inconvenience associated with a prolonged hospitalization.
In cases that required treatment, we found differences in the use of steroid therapy. The dosage was lower both in the first month and the first year of treatment, decreasing to less than half the previous dosage after 2011. The protocols published by the Sociedad Española de Hematología y Hemoterapia (Spanish Society of Haematology and Haemotherapy, SEHH) in 1996 and 2004 recommended treating ITP with a 28-day course of steroid therapy at gradually decreasing doses. From 2010, based on the existing knowledge of the general efficacy and toxicity of this treatment and the similarity in efficacy between doses, the dosage was changed, and the duration of treatment reduced to 5 to 7 days, which would explain the observed difference. The reduction in the performance of splenectomy was also a clear change in the treatment delivered in our hospital, as it was substantial. When it came to surgical intervention, the indication in the Spanish protocols of 1997 and 2004 was a platelet count below 20 × 109/L for more than 6 months or below 50 × 109/L at 12 months from diagnosis, while in the 2011 guidelines splenectomy is recommended for second-line treatment for patients with severe persistent or chronic ITP without contraindications. It is currently recommended that surgery be delayed to at least 12 months after diagnosis unless the child experiences severe bleeding or there is significant impairment of the quality of life. Splenectomy is no longer recommended until 6 months have elapsed from diagnosis due to the possibility of spontaneous improvement or resolution in a small proportion of patients. This was the main factor explaining the changes in the performance of splenectomy identified in our study. In addition, the development of thrombopoietin receptor agonists has offered an alternative that have improved the potential to treat chronic ITP successfully, which probably had an impact on the number of surgeries performed after 2011. We did not address the use of thrombopoietin receptor agonists in our analysis, as their use in our hospital in the period under study took place in the context of clinical trials in nearly every case.
In short, since 2011 there have been several changes in the approach to the management of patients in our hospital: on one hand, they are given a lower dose of steroids and stay in hospital for fewer days, and on the other, there has been a reduction in the performance of splenectomies. These improvements have been achieved without an associated increase in bleeding episodes or a change in the risk of developing chronic ITP. All of these changes could have a positive impact on the quality of life of patients and their families, although corroboration of this outcome would require prospective studies with application of appropriate assessment instruments.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Fernández-Plaza S, Gonzalez de Pablo J, Gálvez E, Zubicaray J, Sevilla J, Sebastián E. Manejo de la trombocitopenia inmune primaria. Comparación de dos cohortes históricas. An Pediatr (Barc). 2021;95:86–92.
