





Up to 15–20% of adolescents have a chronic health problem. Adolescence is a period of particular risk for the development or progression of chronic diseases for both individuals with more prevalent conditions and those affected by rare diseases. The transition from paediatric to adult care begins with preparing and training the paediatric patient, accustomed to supervised care, to assume responsibility for their self-care in an adult care setting. The transition takes place when the young person is transferred to adult care and discharged from paediatric care services. It is only complete when the youth is integrated and functioning competently within the adult care system. Adult care providers play a crucial role in welcoming and integrating young adults. A care transition programme can involve transitions of varying complexity, ranging from those required for common and known diseases such as asthma, whose management is more straightforward, to rare complex disorders requiring highly specialized personnel. The transition requires teamwork with the participation of numerous professionals: paediatricians and adult care physicians, nurses, clinical psychologists, health social workers, the pharmacy team and administrative staff. It is essential to involve adolescents in decision-making and for parents to let them take over gradually. A well-structured transition programme can improve health outcomes, patient experience, the use of health care resources and health care costs.
Hasta un 15–20% de adolescentes tienen algún problema de salud crónico. La adolescencia representa un periodo de riesgo especial para la evolución de las enfermedades crónicas tanto en aquellos con enfermedades más prevalentes como en los afectados por enfermedades raras. La transición de la asistencia pediátrica a la adulta empieza con la preparación y capacitación del paciente pediátrico, acostumbrado a los cuidados tutelados, para que asuma la responsabilidad de su autocuidado en una unidad de adultos. La transferencia es el momento en el que la persona joven pasa a los servicios de adultos y es dada de alta de los servicios pediátricos. La transición sólo se completa cuando los jóvenes están integrados y funcionan con total competencia dentro del servicio de adultos. Los profesionales de adultos tienen un rol crucial a la hora de recibir e integrar a los adultos jóvenes. Un programa de transición puede incluir transiciones de diferente complejidad, desde enfermedades frecuentes y conocidas como el asma, que requieren un proceso más sencillo, hasta enfermedades raras complejas con necesidad de participación de personal muy especializado. La transición requiere un trabajo en equipo con participación de numerosos profesionales: pediatras y médicos de adultos, enfermeras, psicólogos clínicos, trabajadores sociales sanitarios, equipo de Farmacia, y personal administrativo. Es importante implicar a los adolescentes en la toma de decisiones y que los padres los dejen ir progresivamente. Un programa de transición bien estructurado puede mejorar los resultados en salud, la experiencia del paciente y la utilización y coste de los cuidados sanitarios.
Adolescents and young adults are generally regarded as a healthy age group that rarely requires medical care.1 However, up to 15–20% of adolescents have some type of chronic health problem.2–4 This number has grown on account of the increased survival of patients with diseases which, only a few decades ago, were fatal before adulthood, such as cystic fibrosis, congenital heart defects, cancer, neurodevelopmental disorders or chronic complex diseases with technology dependence5 in addition to the increasing incidence of lifestyle diseases such as obesity, asthma or diabetes or mental health disorders.2,3
The passage from adolescence to adulthood is a stage characterised by important physical, psychological and social changes that may have a significant impact on chronic diseases. Adolescents with chronic disease depend on their parents or caregivers to help them manage the condition, which limits their independence. The morbidity caused by the disease, the adverse effects of medication and hospitalizations can affect areas of their daily life including their school attendance and performance, interpersonal relationships and extracurricular activities to a considerable extent.6 Children with disabilities or special health care needs are a particular case, as their families play an indispensable role in their care that continues beyond the transition to adulthood.
In addition, adolescents with chronic diseases are more likely to suffer from mental health disorders such as anxiety or depression.7 The frequency of psychiatric comorbidities in this subset of adolescents is estimated as double that in the general population.2 At the social level, many confess to feeling lonely or isolated from the community.6
On the other hand, adolescence is a stage in which the risk for the development and worsening of chronic diseases is particularly high, both for prevalent diseases1 and rare ones.8 The desire for independence, autonomy and pushing boundaries may lead to poor adherence and risk behaviours such as smoking or alcohol or drug use. Adolescents with chronic conditions engage in these risk behaviours with a similar, if not higher, frequency compared to their healthy peers,2 leading to poorer health outcomes1; some examples of this are the increased probability of exacerbations in patients with asthma or anaphylaxis in patients with food allergy,1 of development of chronic rejection in patients with solid organ transplants and, more generally, not keeping medical appointments and decreased adherence to treatment.9–11
All of the above entails the need for specific support during the transition to adult care. The care model for young people (adolescents and young adults) should differ from the care models for children and adults, but a specific approach for young individuals is not widely implemented in health care systems. The term “developmentally appropriate care” has been proposed to refer to these specific aspects.12,13 Other proposed terms include “age-appropriate”, “adolescent-friendly” or “youth-friendly” care. Such an approach requires12:
- •
The awareness that adolescence entails interrelated physical, cognitive and psychosocial changes.
- •
Accepting the shift in the role of parents and professionals in relation to the adolescent.
- •
Implementing strategies to empower young individuals, fostering their autonomy and promoting the development of self-care skills to assume responsibility for their own management.
- •
Helping the adolescent fit health care goals with other life goals.
From this perspective, the concepts of health care transition and developmentally appropriate care are closely related, as the latter principle encompasses the care needs of all adolescents and young adults during this stage, recognises that the transition to adult care is just one of the many transitions that take place in adolescence (social, cultural and economic) and that each of these individual transitions can have an impact on the rest.12,13
What is a transition of care?The transition from paediatric to adult care services is a planned and organised process to move the patient from a child- and family-centred care system to an adult care system.14 The paediatric care model is based on a substantial involvement of the family in the follow-up of the patient and in decision-making. Adult care is based on the autonomy and independence of the patient. The transition from paediatric to adult care must be a gradual and consensus-based process, as a failed transition can result in decreased adherence to care or even withdrawing from the care pathways established for these patients.
The concept of care transition has evolved from the merely administrative transfer from paediatric to adult care to comprehend the education and empowerment of adolescents and recognise the important role of adult care providers. It has gone from being the exclusive responsibility of paediatric care teams to be shared by paediatric and adult care teams.
A health care transition is not a discrete event occurring at a specific point in time, but a process that includes three phases: transition planning, transfer, and integration into adult care.15
The transition to adult care starts with the preparation and education of paediatrics patients, accustomed to having their care supervised by others, to assume the responsibility for their self-management in adult care services. The transition process must be educational and therapeutic, planned and agreed on between the patient, the family and the paediatric and adult care teams, to the benefit of all involved parties and with the purpose of minimising any potential deleterious effects.
Transfer refers to the moment when the young individual enters the adult care system and is discharged from paediatric care. The transfer is not the end of the transition. The transition is only complete once the young person is fully integrated and functioning competently in the adult care system.15 Adult care providers play a crucial role in the reception and integration of young adults. Young adults are a vulnerable population and may not prioritise health-related issues as much as other dimensions of their lives like education, employment, relationships or leisure. For the transition to be successful, adolescents, young adults and their families must be aware that staying healthy and ensuring the continuity of care are key for achieving all their other goals.
A well-planned transition with a structured protocol and clear goals (Table 1) can facilitate the engagement of adolescents and young adults in their care, increase their self-care skills and promote adherence to care and attendance to follow-up visits in primary care centres or at hospital.9,16 Achieving these objectives requires the identification of existing barriers related to patients and families as well as health care professionals and systems, and addressing them with a multidisciplinary approach (Table 2).
General goals of a structured care transition programme.
| General goals |
| To prepare the patient and family/caregivers to transition from the supervised approach to care of the paediatric care system to a more autonomous engagement with the adult care system.To achieve a successful transition through the collaboration of the paediatric and adult care teams in the transition process, accepted by the adolescent and the family, and ensuring continuity of comprehensive and speciality care.To achieve adequate integration of the young adult in the adult care system. |
| Specific goals |
| Development of a personalised and developmentally appropriate care transition plan based on the maturity and capacities of the patient.Prepare the adolescent and family/caregivers for the transition sufficiently ahead of time, helping the patient develop self-care skills and taking into account the patient’s individual and specific abilities.Working on different aspects of patient empowerment and self-care, both in hospital and community settings.Addressing psychological factors that could pose barriers in the transition process, either in the patient or in the family/caregivers.Coordinate the transfer between the two care teams and facilitate a fluid interaction between members of paediatric and adult care teams.Develop a specific care model for young adults to facilitate integration in the adult care system. |
Difficulties or barriers in the care transition process that must be identified and addressed in a multidisciplinary approach to reduce their impact.
| Adolescent |
|
| Family/caregiver |
|
| Paediatric care team |
|
| Adult care team |
|
| Health care system |
|
It is important to take into account that a transition programme may include care transitions of varying complexity, ranging from prevalent and well-known diseases like asthma, which involve a simpler transition process, to rare and complex diseases that require the involvement of highly specialised staff17 (Fig. 1).
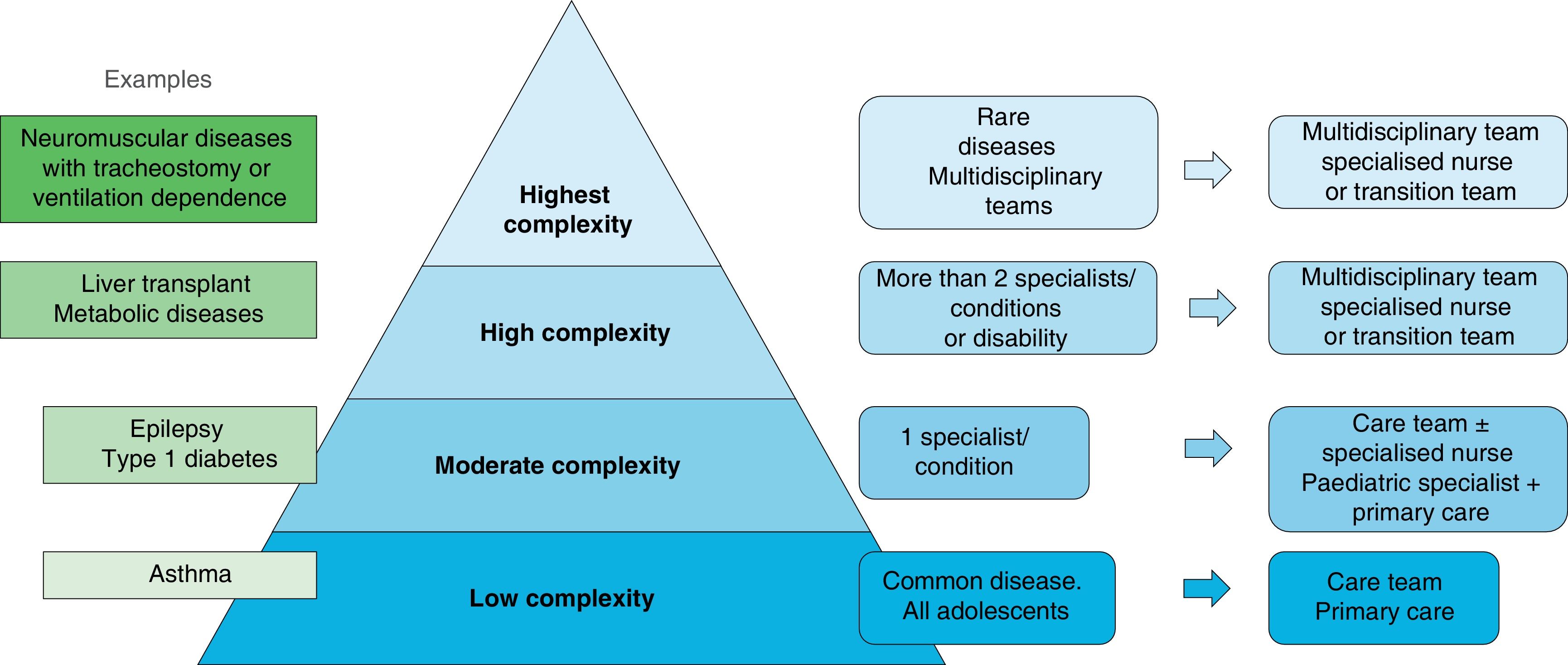
Levels of complexity in the care transition model. Adapted from Szalda D et al.17 with the permission of Elsevier.
In the past two decades, standardised, structured transition models have been developed in health care systems in different countries, such as the United Kingdom (Ready, Steady, Go)18 or the United States (Got Transition).19 In Spain, some hospitals, such as Hospital de La Paz20 or Hospital Vall d’Hebron,21 have developed institution-wide structured care transition programmes. In addition, several scientific societies and expert groups have developed recommendations for the transition to adult care of patients with specific diseases.22–26
Care transition stages and timelineThe transition process has to be individualised, organised in phases and progressive. There are 3 distinct phases: planning the transition from paediatric to adult care, making the transfer to adult care and integrating the patient into adult care, including post-transfer follow-up15 (Fig. 2, Table 3).
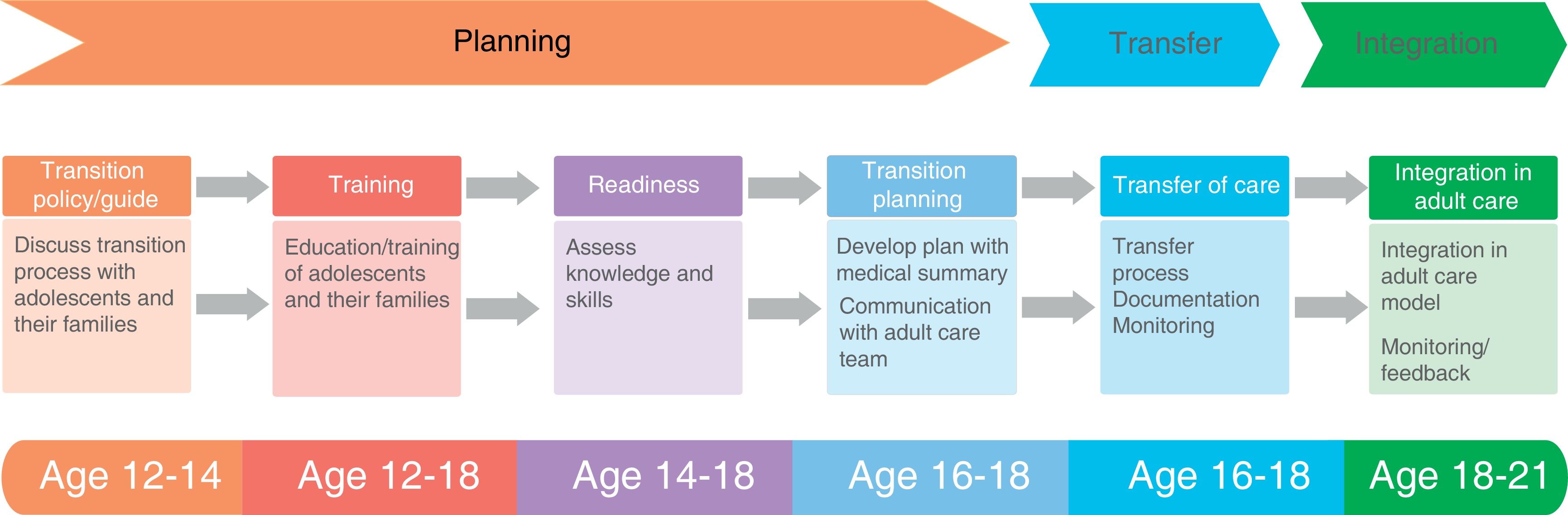
Diagram of the care transition model applied in the Hospital Vall d’Hebron of Barcelona. It is based on the 6 core element model of Got Transition.15
The phases of the transition process.
PlanningTransition guidance: discussion of the care transition process with parents and adolescents.Educating the adolescent and promoting autonomy
|
Planning starts between ages 12 and 14 years. The goal in this phase is to empower adolescents to become autonomous and assume responsibility for self-management.
Transfer usually takes place at age 18 years, although in some cases, depending on pre-existing conditions and the receiving care system, it may take place at age 15–16 years, thus shortening the care transition. Having a transfer “package” or folder with a summary of all the necessary information can be helpful (Table 3).
The integration in adult care and post-transfer follow-up should be completed within 3 years of transfer, over a period lasting 1–3 years.
In our hospital, we adapted the 6 core elements of the GOT Transition model,15,19,21 including 4 distinct components in the transition planning phase (Fig. 2).
Assessment of transition readinessAlthough the timing of transfer is chosen chiefly on the basis of patient age and the regulations of the specific health care system,11 the readiness for transition should also be assessed. Transition readiness questionnaires assess the independence of adolescents in relation to health, their knowledge and their skills, and help identify those at risk of loss to follow-up.27 The routine use of these questionnaires in the care transition process is recommended.15
The Transition Readiness Assessment Questionnaire (TRAQ)28 is widely considered the most appropriate instrument to assess readiness and has been applied in studies of patients with multiple chronic diseases, although it has not been validated for patients aged less than 16 years.27 Other frequently used instruments are the Good2Go,29 GOT Transition19 or STARx questionnaires.30 In addition, an instrument known as the Social-ecological Model of Adolescent and Young Adult Readiness to Transition (SMART)31 has been developed to make a comprehensive assessment of readiness to transition from multiple perspectives, including sociodemographic and cultural characteristics, disease-related factors, neurocognitive and psychological aspects and the level of maturity, in addition to knowledge, skills and autonomy. Other questionnaires developed to date are adequate for collecting information about knowledge and skills, but not for assessing psychosocial aspects.32
Specific questionnaires have also been developed to assess social risk, such as the HEEADSSS (Home, Education/Employment, Eating, Activities, Drugs, Sexuality, Suicidal ideation and Safety) clinician structured interview assessmeent33 or its adaptation into a digital screening instrument, YouthCHAT.34
A study conducted in the United States that included 55 022 adolescents found an increase in the proportion that were adequately prepared for transition to adult care between 2016 and 2020, from 16% to 19%, but the proportion is still small,35 which evinces the need to continue introducing care transition programmes.
Care transition teamThe transition process is team-based and requires the involvement of numerous professionals: paediatricians and adult care physicians, nurses, clinical psychologists, medical social workers and pharmacy and administrative staff.
Nurses play an essential role in educating adolescents about their chronic health condition and teaching them related skills, improving adherence, coordinating transition services and resources with different providers and levels of care, supporting youth through the care transition and monitoring transition outcomes and quality of life.36
Although it is possible to establish successful transition programmes specific diseases with dedicated teams, the implementation of a general care transition team for all adolescents, independently of the disease, can greatly benefit from the establishment of teams specialised in care transitions to coordinate the programme and support the different care teams.3,17
For the transition to be a success, it is not enough to implement a structured programme to train and educate adolescents; instead, the transition intervention must be a collaborative process involving the adolescent or young adult, parents and health care professionals.11 In a recent study, 70% of interviewed adolescents and young adults expressed the desire to have more information about their disease, including its natural history, the available treatments and their long-term effects, followed in frequency by needs related to lifestyle habits, such as nutrition or physical activity.6
It is important that health care providers involve adolescent patients in decision-making, empowering them to make choices, encouraging them to take responsibility for their own care, addressing them, asking them and listening to them so that parents do not speak for them throughout the visits, thus allowing adolescents to become increasingly independent.
Parents have to trust the ability of their children to take over their own care and proactively encourage them to self-care at home and learn to self-manage their medication. Parents must undergo a transition of their own to give up their role as primary caregivers, gradually learning to trust and let go adolescents and young adults.11
In the case of patients with severe intellectual disability that precludes autonomy in self-management or activities of daily living, the family or their legal guardians will continue to represent them. The care transition plan will be adapted to the level of understanding and ability to self-care of the adolescent.
The role of primary care in the care transition processPrimary care professionals (paediatricians, family physicians and nurses) play an important role in the transition to adult care, even in the case of adolescents with complex diseases requiring highly specialised care. In addition to addressing their general health care needs (vaccination, birth control, etc), they can ensure continuity of care for adolescents, young adults and their families, which can have a very beneficial impact on patient outcomes.4 Thus, for instance, a lower frequency of diabetes-related hospital admissions has been reported in adolescents who were followed up at the primary care level during the transition to adult care.37
The care of the patient can be transferred to a hospitalist or a family physician.38 In the case of common diseases like asthma, the care of the patient is usually transferred to family physicians, maintaining management by a specialist in severe cases.
In spite of the above, the role of primary care in the structured transition process is not adequately recognised in the literature, and communication gaps between levels of care still abound. A recent study based on interviews to primary care providers yielded the following key points to improve their contribution in care transitions38:
- •
Adequately educating adolescents and young adults of the important role of primary care providers in their care.
- •
Adapting primary care services to adolescents and young adults, offering more flexible and longer appointments.
- •
Participate, if necessary, in shared visits with specialists.
- •
Produce summary reports or letters to facilitate the transition of the patient.
An important challenge for care transition programmes is to be appealing to adolescents to attract their engagement and participation. Some authors have proposed that the support of other adolescents, especially with similar chronic conditions, could facilitate a better transition.39 Some patient associations offer transition support programmes for adolescents and parents that can contribute significantly to the success of the transition. It is important for care transition teams to collaborate with patient associations, know their activities, disseminate information about them and promote the participation of their patients.
The activities can be as varied as weekend or summer camps or overnight programmes, half-day or day-long sessions, individual interviews between the adolescent and members of the association or support groups.
These interventions can be helpful with aspects such as increasing knowledge of the disease and promoting better communication with health care professionals, improving adherence to treatment, fostering relationships between patients, providing a meeting space where adolescents can talk, interact, break their isolation and gain confidence, contributing to their empowerment and autonomy, helping them become independent from their parents and develop life goals.39
Integration into adult careAdult care providers play a crucial role in receiving and integrating young adults. Adult care systems must recognise young adults as a population with special needs. Providers serving young adults must have adequate knowledge of congenital or childhood-onset diseases and adolescent and young adult development.
In the early visits, it is important to:
- •
Address any concerns the young adult has about the transition to adult care and develop rapport.
- •
Explain the adult care approach (shared decision-making, confidentiality and consent, access to health records).
- •
Ensure that sufficient routine or follow-up visits are scheduled early in the transition, which may be greater compared to standard adult patients, in order to ensure adequate follow-up and facilitate adjustment to the new situation.
To improve the outcomes of health care transition interventions, it is important to assess their quality, preferably within a “triple aim” framework16,40:
- •
Health outcomes: adherence to care and follow-up visits, disease-specific outcomes, quality of life, self-care skills, complications, mortality. Some examples of disease-specific or adherence to care outcomes are: glycated haemoglobin levels, frequency of epileptic seizures, juvenile idiopathic arthritis control scales, renal graft survival, etc.
- •
User experience: satisfaction and barriers to care.
- •
Utilization and costs of care: frequency of pretransition vs post-transition outpatient visits, hospital admissions, emergency department visits etc.
Several systematic reviews have shown that a well-structured health care transition programme can improve these 3 aspects.16
FundingThis research did not receive any external funding.
Conflicts of interestThe authors have no conflicts of interest to declare.
