




Pediatric hospitalization at home (HAH) aims to provide the patient and his family with an alternative to conventional hospitalization, safely and effectively, improving the quality of life of the patient and his family. The most frequent pathologies in HAH in pediatric acute patients are acute respiratory pathology and bacterial infections that require parenteral antibiotic therapy. The success of an acute patient home hospitalization program relies on the proper selection of patients and exhaustive training of caregivers, as well as good communication and coordination between the different services and levels of care involved.
La hospitalización a domicilio (HAD) pediátrica tiene como objetivo proveer al paciente y a su familia de una alternativa a la hospitalización convencional, de forma segura y eficaz, mejorando la calidad de vida del paciente y su familia. Las patologías más frecuentes en HAD de paciente agudo pediátrico son la patología respiratoria aguda y las infecciones bacterianas que precisan antibioterapia parenteral. El éxito de un programa de hospitalización domiciliaria de paciente agudo recae en la adecuada selección de pacientes y la exhaustiva capacitación de los cuidadores, así como en una buena comunicación y coordinación entre los diferentes servicios y niveles de atención implicados.
Paediatric hospital at home (HAH) is a clinical service offering care to acutely ill patients employing the staff, equipment, technology, medication and expertise typically available at hospital, yet delivered at the home of the patient.
The aim of hospital at home is to provide patients and families an alternative to conventional hospitalization for the delivery of care and treatment that is safe and effective yet improves the quality of life of patients and families, as it is carried out at home. This approach to hospital care recognises that the satisfaction of patients and families increases on account of the greater involvement of the family in patient care and the more humane approach to care delivery. There is also evidence of improved outcomes in terms of certain complications, such as a reduction in the incidence of health care-associated infection.
This care model also allows the optimization of health care resources, helping reduce the pressure on hospitals by making more beds available and reducing the costs of hospitalization through home-based care.1
Background and current situationThe origins of HAH hail back to 1947, at the Hospital Guido Montefiore in New York. The hospital instituted its home care programme to allow patients to complete their recovery at home with support from the hospital including nursing, rehabilitation and social work services. The goals of this pioneering programme were to alleviate the care burden on the hospital and to humanize patient care. In 1951, similar projects were implemented in France, and thereafter throughout Europe.2 In Spain, the first HAH unit was instituted in 1981 at the Hospital Provincial de Madrid on the initiative of Dr. José Sarabia.3
In Spain, home-based hospital care services for adults are well established, with more than 100 HaH units currently devoted to adult care. When it comes to the paediatric population, there have been HAH units for more than 20 years, but they are chiefly focused on the care of patients who are medically complex, chronically ill or with palliative care needs (whose numbers have been increasing in recent years) or other specific fields, such as neonatology, cystic fibrosis or oncology. While there are mixed units serving both chronic and acute patients, such as those at Hospital General Universitario in Alicante or Hospital Universitario La Fe in Valencia, at present there are only 3 units specifically devoted to patients with acute conditions (at Hospital Niño Jesús de Madrid, Hospital Sant Joan de Déu de Barcelona and Hospital de la Paz de Madrid), created in 2018, 2019 and 2021, respectively.
The need for HAH in acute paediatric patientsIn 1986, the European Parliament passed the Charter of the Rights of Children in Hospital, followed in 1988 by the EACH (European Association for Children in Hospital) Charter. Some of the articles in this charter stipulate that all ill children have the right to receive care at home or an ambulatory centre and that “children shall be admitted to hospital only if the care they require cannot be equally well provided at home or on a day basis”. It also specifies that children should be hospitalized for “the shortest possible time”.4 All of these rights are pursued through HAH units.
In recent decades, in the field of paediatrics, as has occurred in adult care, the concepts of self-care and of empowerment in relation to the disease process, both for the patient and the caregivers, have gained prominence. Self-care is defined as the set of actions carried out by a person in pursuit of their own health or wellbeing. According to the principle of autonomy, individuals have the ability to make decisions regarding their health. In short, the HAH model agrees perfectly with these concepts, as it empowers patients and their caregivers.
The benefits of HAH include the humanization of care and the improved wellbeing of the patient, health education, improved doctor-patient/family communication, reduced risk of complications related to health care (such as infection), economic benefits and more efficient use of health care resources.
Another significant factor is the substantial saturation of hospitals, chiefly due to the surge in paediatric chronic diseases and periodic seasonal outbreaks of disease. In the past 40 years, medicine has undergone significant changes, partly due to technological advances in the field. As a result, it has been possible to make many diseases that used to be lethal chronic instead, with the drawback that these patients tend to need many health care resources, including hospital beds. In this regard, the HAH model offers a more efficient alternative than conventional hospitalization, optimizing the use of the available health care resources and possibly reducing overall costs.
Characteristics of HAH units for acute paediatric patientsIt is recommended that HAH units be staffed by a multidisciplinary team of physicians and nurses with previous experience in conventional hospitalization. The unit should also be supported by various specialists depending on the type of patient that it serves. The support of the department of pharmacy is essential to these units to provide both guidance on the appropriate selection of drugs, including information on their physical and chemical stability, and in the preparation of drugs to improve their microbiological stability. Support from specialists in other fields, such as infectious disease or haematology and oncology, is also recommended, as patients in these fields tend to be good candidates for home-based hospital care.
Since HAH units tend to be cross-departmental, patients can be referred to it from any of the hospital departments as long as they meet the eligibility criteria and their clinical stability can be guaranteed.
The programme must offer a schedule of in-person home visits (from the physician and/or nurse) to ensure that the quality of the follow-up is the same as in conventional hospitalization. The interval between visits is determined based on the clinical condition of the patient, the required treatment and its route of administration and the resources of the institution.
It is recommended to give families support through telemedicine services adapted to the disease of the patient and telephonic access to the unit 24 h a day to consult on any concerns that arise.
After-hours care, depending on the available resources, is delivered by the staff of the HAH or by the staff of the emergency department of the hospital, who should have been previously trained for the purpose.
A substantial part of the daily activity of the HAH team concerns the identification and eligibility assessment of potential candidates and patient education. The responsibility for candidate identification and selection is usually shared by the doctors and nurses of both HAH and conventional hospitalization care teams. Patient education is usually delivered by nurses in the HAH team.
Patient eligibilityThe identification of the main diseases and treatments suitable for HAH and ensuring that the home environment is appropriate are key to the success of home-based hospital care. Table 1 presents the conditions that must be met for a paediatric patient to be admitted to a HAH unit. We ought to highlight that these criteria apply both to patients with acute disease and patients with chronic disease experiencing an acute exacerbation.
Necessary conditions for admission to HAH.
| Necessary conditions for admission to HAH |
|---|
| Family |
|
| Disease |
|
| Home |
|
| Hospital |
|
Once it has been confirmed that the patient meets the eligibility criteria, the transfer is prepared. A care plan must be established by the HAH team, including planning for any diagnostic tests that may require transport to the hospital, the collection of samples at home and the estimated length of stay.
Acute respiratory infections are among the most prevalent diseases in the paediatric population and responsible for substantial surge pressures on hospitals, especially in the winter months. Among them, acute bronchospasm is one of the most frequent reasons for admission in children’s hospitals, with most cases requiring respiratory support with low-flow oxygen therapy and bronchodilators. These treatments can be provided safely at home, always after adequate training. The health education delivered to patients admitted to HAH due to bronchospasm is not only useful for the acute disease that is the reason for admission but also for future episodes, as the parents are provided with tools to identify clinical worsening and signs of severe disease and taught the correct technique to administer medication.
Another frequent reason for hospital admission is infection requiring intravenous antibiotherapy. Most commonly used antibiotics can be administered at home after establishing the appropriate vascular access and with a dose frequency not exceeding 3 or 4 doses a day. When patients require administration of several doses per day, the active participation of the caregiver is essential. Despite the initial reservations that the autonomous administration of intravenous medication by nonpractitioners may elicit, in the past few years of experience there have been no serious medication administration errors and the experience of families has been very positive.
Training of the primary caregiverThe patient and the caregiver become especially important in hospital at home. Their involvement is key to the success of the programme and they play an active role throughout the care delivery process. One of the main roles of HAH nurses is to empower families by providing basic knowledge and resources on the disease of the patient and its management, teaching the necessary skills to use monitoring devices (pulse oximeter, blood pressure monitor, thermometer, glucose meter or scale), administer treatment and specific care procedures depending on the reason for admission. We must underscore the importance of correctly anticipating potential incidents or complications to be able to respond quickly and effectively, thus minimising the risk to patients.
During the training process, the main caregiver will receive a large amount of technical information that may be complex. Therefore, it is important to adapt the language used in its communication to the particular recipient and summarise the most important information clearly and concisely. Providing support materials to families, in the form of printed content or videos, may also be helpful.
The key points that need to be addressed in the educational session are: (1) basic aspects of how the unit works, (2) description of the disease and its potential complications and 3) care delivery, administration of treatment and management of at-home devices.
The training session is tailored to the disease of the patient, the devices to be used and the personalized care plan based on the patient’s needs. Since respiratory infections requiring oxygen therapy and infections requiring intravenous antibiotherapy are the diseases managed most frequently in HAH units, the devices most frequently used at home are those use for respiratory support intravenous drug delivery (Fig. 1).
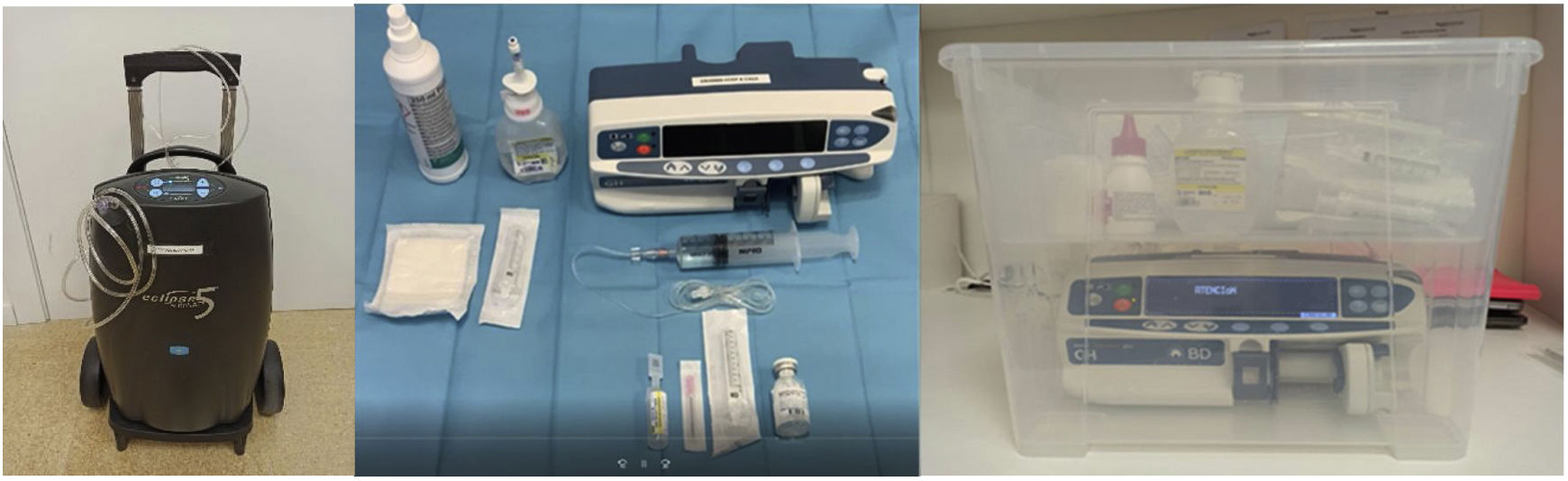
There are different methods for low-flow oxygen delivery, among which liquid oxygen systems and oxygen concentrators are the most widely used, especially small, automated devices easily portable within and outside the home. If there are smokers in the household, they must commit to maintain a smoke-free environment.
As regards the administration of intravenous antibiotherapy, most drugs are delivered over periods of less than 1 h with continuous infusion pumps. It is essential that appropriate vascular access suitable for the intended duration of treatment be established; in patients that required prolonged treatment, a peripherally inserted central catheter is the preferred option. Antibiotic drugs must be stable once they are reconstituted with doses delivered, ideally, every 12–24 hours. In select cases, it may be possible to use antibiotics that must be administered immediately after being reconstituted. The fact that in paediatric care the caregivers tend to be comparatively young facilitates the use of more complex medication (greater dose frequency, drugs that need reconstituting).
The understanding and appropriate implementation of care procedures will be assessed before the transfer home and reassessed in successive visits, also addressing any questions or concerns as they arise.
Challenges of HAH to take into accountThe creation of a HAH unit for patients with acute conditions or exacerbations of chronic disease involves poses multiple organizational challenges. First of all, staffing may not necessarily meet the ratios established for conventional hospitalization. While physicians and nurses may not be able to manage the same number of patients that they would in hospital, HaH allows a reduction in staffing in terms of nursing shifts, technician-level and janitorial staff or nutrition services, or even the necessary staff to provide after-hours or urgent care. Multiple factors also affect the organization of daily care delivery: significant patient turnover, the location of the hospital, the geographical dispersion of the homes, the means of transport used, the time of transport, traffic, etc. In this regard, a route planning system can be used optimise the organization of care delivery.5 Lastly, home-based care differs from hospital-based care in terms of material resources, which need to be as compact and user-friendly as possible, and in decision-making, which requires a pragmatic approach and a focus on patient safety, always attempting to anticipate potential complications. The success of a HAH programme for acute patients hinges on the adequate selection of patients and the thorough training of caregivers. It depends largely on the composition of the multidisciplinary unit, including nurses with experience in conventional and home-based hospital care and capable of delivering care and education autonomously. Candidates to HAH need to be stable and have a low risk of clinical complications. It is also important to assess socioeconomic aspects before transfer, for instance, the number of people living in the household, whether the home meets hygiene and sanitation standards or any language and cultural barriers that could interfere with the home-based delivery of hospital-level care, among other factors. Adequate education of all caregivers, if there is more than one, needs to be ensured, in addition to verifying throughout the care episode the adequate understanding and delivery of care and the establishment of a treatment plan, known to the parents, including the potential problems that may arise.
What has been learned in the past few years and future lines of researchAs demonstrated in previous studies6–9 and by other research groups, HAH is a safe and effective strategy as an alternative to conventional hospitalization. Leaving aside the economic and organizational advantages that it may offer at the level of health care administration or hospital management, patients and their families derive the greatest benefits of HAH. Home-based care prevents the deleterious effects of institutionalization and improves the comfort of patients and their families. In addition, this care modality promotes the empowerment of families in the management of the child, involving them actively in care delivery. In addition, the improvement in the doctor-patient rapport and communication achieved with HAH contributes to the satisfaction of families and the professionals responsible for the care of these children.
Acute patients require continuous care around the clock, so good communication and coordination between the different departments and levels of care involved is of the essence. Although patients admitted to HAH are stable and families trained on how to administer treatments and resolve the most common incidents that can be expected to arise, to guarantee patient safety it is important that 24/7 remote care is offered in addition to in-person home visits. After hours urgent care pathways must also be established with involvement of the specialities and fields required for the management of the patient.
Institutional support is essential in the framework of a plan to consolidate and expand paediatric HAH services, which should be promoted through policy and by public health administrators to ensure that the development of these units does not depend exclusively on the motivation and effort of individual hospitals and that the greatest possible number of children can benefit from this modality of care.
The infrastructure and human resources required to launch a HAH unit are not available in every hospital serving the paediatric population, but there is no question that home-based hospital care services for children must continue to develop. Possible strategies include the development of HAH referral units covering the needs of several hospitals, or the involvement of adult HAH units to offer care to select paediatric patients with the support of paediatric staff (paediatricians and paediatric nurses). Since many diseases can be treated at home, it is important to reflect on his matter and attempt to expand the type of patients that could benefit from HAH services (oncological, psychiatric, surgical patients…).
Although there are still few paediatric units to deliver home-based hospital care to acute paediatric patients in Spain, this approach has proven to be safe and satisfactory for patients, families and health care providers. The coordination of care delivery and the development of standardised protocols across the different HAH programmes in Spain can improve the performance of existing units and promote the development of new HAH services in other institution. In brief, we consider that it is important to promote the creation of new programmes in order to integrate paediatric HAH in everyday clinical practice.
FundingNo funding was awarded to this project.
Conflicts of interestThere are no conflicts of interest to disclose.
We thank the Working Group on Hospital at Home of the SEPIH (Beatriz Agúndez, Andrea Aldemira, Joaquín Aliaga, Mara Andrés, Astrid Batlle, Isabel Cabrera, Silvia García, Ester Pérez, Rebeca Gracia).
We also want to express our appreciation to María Fabregat, from the Paediatric Haematology and Oncology team of the Hospital at Home Unit of the Hospital Sant Joan de Déu.
