





Giardiasis is a gastrointestinal parasitosis that has a great public health impact.
Patients and methodsObservational case study — in children under 15 years old in the Health Department 3 of the Province of Castellon (Spain), during the period 2012–2019.
ResultsA total of 190 cases of giardiasis were recorded in children under 15 years old. The number of cases varied significantly according to age group and month of the year. There were 115 males. The most frequent symptoms were diarrhoea and abdominal pain. The most commonly used treatment was standard metronidazole (80% of patients). Co-infection occurred in 13% of cases, and comorbidities in 36%, especially atopic dermatitis and lactose/fructose intolerance. Relapses and/or re-infections were recorded in 8%. All cases were diagnosed by conventional parasitological stool tests and complementary immunochromatography (63 cases). Thirty-five samples were positive for Giardia duodenalis by qPCR. The direct health cost per patient was 117€. A disease notification bias was detected between 2012–2016 at a national scale.
ConclusionsGiardiasis is a current disease in Castellon, and should be considered as a probable diagnosis of gastrointestinal disease in a child under 4 years-old with diarrhoea and abdominal pain. Its correct clinical and therapeutic management could reduce the possibility of worsening of the patient's condition and, additionally, would reduce the economic impact of the disease in terms of direct health costs.
La giardiosis es una parasitosis gastrointestinal de impacto en salud pública.
Pacientes y métodosEstudio observacional de los casos en menores de 15 años atendidos durante el periodo 2012–2019 en el Departamento 3 de Salud de Provincia de Castellón (España).
ResultadosSe registraron 190 casos en menores de 15 años. El número de casos varió significativamente según grupo etario (55% en grupo 0−4 años) y momento del año (mayoría agosto-noviembre). El índice de masculinidad resultó de 115. Los síntomas más frecuentes fueron diarrea y dolor abdominal. El tratamiento más empleado fue metronidazol en pauta estándar (80% de los pacientes). El 13% de los casos presentaron coinfección y el 36% comorbilidades, principalmente dermatitis atópica e intolerancia a la lactosa/fructosa. Se registró un 8% de recidivas/reinfecciones. Todos los casos se diagnosticaron por tests coproparasitológicos convencionales y algunos, además, con inmunocromatografía (63 casos). Treinta y cinco muestras fueron confirmadas para Giardia duodenalis por qPCR, descartándose sesgo diagnóstico. Se detectó un sesgo de notificación a escala nacional para el periodo 2012–2016. El coste sanitario directo por paciente resultó de 117€.
Conclusionesla giardiosis es una enfermedad vigente en nuestra región que debe ser considerada (en el diagnóstico diferencial) como diagnóstico probable de patología gastrointestinal ante un niño menor de 4 años con diarrea y dolor abdominal. Su correcto manejo clínico disminuiría la posibilidad de empeoramiento del paciente y evitaría la hospitalización, reduciendo el impacto económico de la patología en términos de coste directos sanitarios.
Giardiasis is a gastrointestinal parasitic infection caused by Giardia duodenalis that is found worldwide.1 In Spain, there were 16 974 reported cases of giardiasis between 1989 and 2010,2 with a prevalence rate of infection of 3%–7% in asymptomatic individuals and 13%–25% in symptomatic individuals.2–8
The main group at risk of this disease is the paediatric population,9 as there is a significant association between giardiasis and malnutrition, cognitive impairment and growth.10–13 In some cases, giardiasis is not included in the differential diagnosis of patients presenting with symptoms such as persistent diarrhoea, vomiting and epigastric pain.14 This results in delays in diagnosis that increase health care costs and cause inconvenience to patients in terms of wasted time and serious discomfort, with a general worsening of overall health and development of chronic disease and additional complications.10,15,16
We conducted a study to review the paediatric cases of giardiasis diagnosed on Department 3 of the public health system of the province of Castellon (Valencian Community, Spain), in the past 7 years with the aim of describing the epidemiology, characteristics, clinical management and economic impact of this infection.
MethodsWe conducted a mixed-method observational study of the cases of giardiasis in children aged less than 15 years managed in Department 3 of the public health system of the province of Castellon, with a retrospective review of cases in the 2012–2017 period and prospective surveillance in the 2018–2019 period. The inclusion criteria were age 0–15 years and date of diagnosis between January 2012 and January 2019. We collected data from the health records to analyse sociodemographic variables (age, sex, town of residence), clinical variables (signs and symptoms, complications, relapses, reinfections, coinfections, comorbidities, mortality) and management variables (diagnostic methods, hospital admission, prescribed treatment, post-treatment follow-up). We assessed diagnostic inaccuracy by testing 35 samples selected at random by quantitative PCR (qPCR) for detection of the small subunit ribosomal ribonucleic acid (SSU rRNA) of G. duodenalis.12 To compare the identified cases by area of residence we used the incidence rate (IR) by town of residence, calculated as follows:
We defined the population at risk as the number of inhabitants of each town, retrieved from the official data published by the Instituto Nacional de Estadística (National Institute of Statistics, https://www.ine.es). We performed hypothesis testing for two proportions to analyse sex, the chi square test to analyse age and the 2-sample Student t-test to analyse seasonality. To assess reporting bias, we compared the number of cases documented each year to the number reported in the bulletins of the Instituto de Salud Carlos III de Madrid and the Department of Universal Health Care and Public Health of the Valencian Community. To calculate direct health care costs (DHCCs), we used the GAIA® pharmacy management system17 and the rates for the Groups Related to the Diagnosis and Procedures in outpatient and inpatient care established by Law 20/2017, of December 28 on rates and fees of the government of Valencia.18 The study was approved by the Clinical Research Ethics Committee of the Hospital Universitario de la Plana (code 31.01.2018).
ResultsBetween 2012 and 2019, 190 cases of giardiasis were diagnosed in children under 15 years, which amounted to 39% (2017) to 59% (2015) of the total cases reported in the province. Between 2012 and 2016, total numbers of cases were not published in official bulletins at the national level.
The IR of the period under study was of 0.9 cases per 1000 inhabitants (95% confidence interval [CI], 0.8–1.1). Fig. 1 presents the distribution by town of residence, showing that Onda was the town with the highest cumulative incidence (1.6 cases/1000 inhabitants) and Alquerías del Niño Perdido the lowest one (0.4 cases/1000 inhabitants). The sex distribution was 54% male and 46% female, with a male-to-female ratio (MFR) of 1.15 (cases in male individuals per case in female individuals), although the observed difference between sexes was not significant (P = .119). The age group with the highest number of cases was the 0−4 years group (55%; n = 101), with a significant difference in the incidence compared to other age groups (P < .001) (Table 1). We found variation in the incidence throughout the year, with a significant increase (P < .001) in the months of August, September, October and November.
 of paediatric giardiasis in Department 3 of the health system of the province of Castellon, Spain, by town of residence of the patient. Image generated with the free access tool mapinseconds.com (Eugene Chen, Darkhorse Analytics), available at: http://www.mapinseconds.com/.")
Incidence rate (cases ×105 inhabitants) of paediatric giardiasis in Department 3 of the health system of the province of Castellon, Spain, by town of residence of the patient. Image generated with the free access tool mapinseconds.com (Eugene Chen, Darkhorse Analytics), available at: http://www.mapinseconds.com/.
Epidemiological data of the 190 cases of giardiasis in children under 15 years diagnosed in the 2012–2019 period in Department 3 of the health system of the province of Castellon, Spain.
| Age range (years) | Female | Male | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| 0−4 | 48 | 54 | 58 | 57 | 106 | 56 |
| 5−9 | 33 | 37 | 31 | 31 | 64 | 34 |
| 10−14 | 8 | 9 | 12 | 12 | 20 | 10 |
| TOTAL | 89 | 100 | 101 | 100 | 190 | 100 |
The most frequent symptoms were diarrhoea (n = 80 patients) and abdominal pain (n = 65) (Table 2). A conventional stool ova and parasite examination (Parasep SF Patient Care Pack®) was performed for diagnosis in 100% of cases, with the addition in 34% of cases (n = 63) of Giardia antigen detection by immunochromatographic assay (OPERON, S.A. Zaragoza, Spain). The 35 samples selected for confirmation of G. duodenalis by qPCR were all positive, with a Ct of less than 30 in 16.
Clinical features of the 190 paediatric cases of giardiasis diagnosed in the 2012–2019 in Department 3 of the public health system of the province of Castellon, Spain.
| Feature | n | % |
|---|---|---|
| [0,1–3]Signs and symptoms | ||
| Diarrhoea | 80 | 42 |
| Abdominal pain | 65 | 34 |
| Fever | 41 | 22 |
| Loss of appetite | 21 | 11 |
| Dysphagia, odynophagia, dyspepsia | 15 | 8 |
| Nausea/vomiting | 13 | 7 |
| Rectal itching | 10 | 5 |
| Weight loss/anorexia | 11 | 6 |
| Stools with blood, mucus, pus or abnormal colour | 19 | 10 |
| Abnormal stool consistency | 8 | 4 |
| Asthenia, fatigue | 3 | 2 |
| Meteorism and constipation | 3 | 2 |
| Headache | 3 | 2 |
| Dermatitis | 3 | 2 |
| [0,1–3] | ||
| [0,1–3]Laboratory features | ||
| Hypoproteinaemia | 3 | 2 |
| Eosinophilia | 3 | 2 |
| [0,1–3] | ||
| [0,1–3]Other | ||
| Asymptomatic | 11 | 6 |
| Not documented | 13 | 7 |
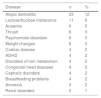
In 13% of cases (n = 24), the stool examination detected the presence of other microorganisms, most frequently Campylobacter species (n = 9) and Blastocystis species (n = 8) (Table 3). Seventy patients had documented comorbidities (37%), the most frequent being atopic dermatitis (n = 23) and lactose/fructose intolerance (n = 11) (Table 4). The abnormalities detected in blood tests were hypoproteinaemia (n = 3) and eosinophilia (n = 3). Eleven patients were asymptomatic, and the health records of 13 patients did not include information on clinical manifestations. One patient required hospital admission with a length of stay of 5 days, and the rest were managed and followed up at the outpatient level. The most frequent initial treatment was metronidazole (n = 154; 83%), administered orally every 8 h for a total dose of 15 mg/kg/day for a total of 7 days (Table 5). The alternative regimens prescribed included doses of 750 mg every 8 h for 15 days, of 250 mg every 8 h for 5 days and of 500 mg every 8 h for 5 or 7 days. An additional ova and parasite test was performed in 60% of patients after completion of treatment, which detected relapse or reinfection in 15 patients (8%). The patient admitted to hospital was a boy aged 3 years with coinfection by rotavirus that presented with fever, vomiting and diarrhoea.
Other microorganisms detected in the stool samples of the 190 paediatric patients with giardiasis diagnosed in the 2012–2019 in Department 3 of the public health system of the province of Castellon, Spain.
| Microorganisms | n | % |
|---|---|---|
| [0,1–3]Bacteria | ||
| Campylobacter spp. | 9 | 5 |
| Salmonella spp. | 1 | 0.5 |
| [0,1–3] | ||
| [0,1–3]Parasites | ||
| Blastocystis sp. | 8 | 4 |
| Dientamoeba fragilis | 2 | 1 |
| Entamoeba histolytica | 1 | 0.5 |
| Chilomastix mesnili | 1 | 0.5 |
| Cryptosporidium spp. | 1 | 0.5 |
| Endolimax nana | 1 | 0.5 |
| [0,1–3] | ||
| [0,1–3]Virus | ||
| Rotavirus | 1 | 0.5 |
Comorbidities identified in the 190 paediatric cases of giardiasis diagnosed in the 2012–2019 period in Department 3 of the public health system of the province of Castellon, Spain.
| Disease | n | % |
|---|---|---|
| Atopic dermatitis | 23 | 12 |
| Lactose/fructose intolerance | 11 | 6 |
| Anaemia | 9 | 5 |
| Thrush | 6 | 3 |
| Psychomotor disorders | 6 | 3 |
| Weight changes | 6 | 3 |
| Coeliac disease | 4 | 2 |
| ADHD | 4 | 2 |
| Disorders of iron metabolism | 4 | 2 |
| Congenital heart diseases | 4 | 2 |
| Cephalic disorders | 4 | 2 |
| Breastfeeding problems | 4 | 2 |
| Anorexia | 3 | 2 |
| Renal disorders | 2 | 1 |
Clinical management of 190 paediatric cases of giardiasis in the 2012–2019 period in Department 3 of the public health system of the province of Castellon, Spain.
| Management | n | % |
|---|---|---|
| [0,1–3]Hospital admission | ||
| Yes | 1 | 1 |
| No | 150 | 79 |
| Not documented | 39 | 20 |
| [0,1–3] | ||
| [0,1–3]Initial treatment | ||
| Metronidazole | 154 | 81 |
| Mebendazole | 1 | 1 |
| Fluconazole | 1 | 1 |
| Paracetamol | 1 | 1 |
| Probiotic | 1 | 1 |
| Homeopathic treatment | 1 | 1 |
| Not documented | 31 | 14 |
| [0,1–3] | ||
| [0,1–3]Metronidazole regimen | ||
| Standard* | 128 | 67 |
| Other regimens | 26 | 14 |
| Not documented | 36 | 19 |
| [0,1–3] | ||
| [0,1–3]Control posterior | ||
| Yes | 115 | 60 |
| No | 49 | 26 |
| Not documented | 26 | 14 |
The total DHCCs amounted to €22 179.65, with an annual mean of €3168.52 and a mean DHCCs per patient of] €117 (Table 6).
Direct health care costs derived from the management of 190 paediatric cases of giardiasis in the 2012–2019 period in Department 3 of the public health system of the province of Castellon, Spain.
| Service category | Cost category | Number of instances | Cost per instance (€) | Total (€) |
|---|---|---|---|---|
| Medical visit | Initial primary care visit at the health care centrea | 155 | 56.95 | 8827.25 |
| Initial visit to paediatrician or neonatologistb | 21 | 124.75 | 2619.75 | |
| Initial visit to emergency departmentc | 5 | 189.49 | 947.45 | |
| Initial visit to doctor in a different speciality* | 3 | 65.02 | 195.06 | |
| Primary care visit, follow-upd | 92 | 29.05 | 2672.6 | |
| Paediatrics visit, follow-upe | 20 | 49.49 | 989.8 | |
| Visit to a different specialist, follow-up*,f | 3 | 40.02 | 120.06 | |
| Diagnosis | Ova and parasitesg | 190 | 8.58 | 1630.2 |
| Immunochromatographyh | 63 | 16.09 | 1013.67 | |
| Treatment | Metronidazole (tablets) | 154 | 1.12 | 172.48 |
| Metronidazole (syrup) | 18 | 1.45 | 26.1 | |
| Fluconazole | 1 | 12.86 | 12.86 | |
| Mebendazole | 1 | 3.34 | 3.34 | |
| Paracetamol | 1 | 0.86 | 0.86 | |
| Probiotics | 1 | 8.65 | 8.65 | |
| Subsequent follow-up | Ova and parasitesg | 115 | 8.58 | 986.7 |
| Admission | Inpatient carei | 1 | 1952.82 | 1952.82 |
| Total | 844 | 2569.12 | 22179.65 |
Procedure codes18.
Our study identified giardiasis as a potential cause of gastrointestinal disease in the paediatric population of our region. The area covered in the study contributes a large number of cases to the total in the province, where parasitosis has an uneven distribution.
In Spain, official reports only present a portion of the total cases, as they do not include asymptomatic carriers.2,8,19 The latter play an important role in the transmission of disease, which poses a risk to vulnerable groups, such as children, the elderly and immunosuppressed individuals.1,2 Our study evinced that the cases diagnosed in the 2012–2016 period were not included in government bulletins.
In our case series, we found differences based on age, with more than half of the cases occurring in children under 5 years. Giardiasis affects growth and cognitive development, which may have an impact on the future potential of the patient if it is not treated correctly.
When it came to diagnostic testing, we found that the ova and parasite stool examination continued to be the routine test used. In some cases, an immunochromatographic assay was performed for confirmation, a method that works well for medium to high parasite loads but is not sensitive enough to detect low parasite loads, with a false negative rate of 13.3% and a false positive rate of 5.2%.20,21 We used qPCR to confirm the presence of G. duodenalis, which revealed a good diagnostic yield in the microbiology department in terms of the specificity of the test.
Most molecular tests performed in Spain to evaluate giardiasis identify genotype B, the most frequent genotype isolated in human cases.12,22,23–25 Recently, evidence has emerged that suggests that the distribution of G. duodenalis genotypes may be different in children and adults; children under 12 years are more commonly infected with assemblage B and present with abdominal pain, swelling and diarrhoea as the main symptoms.26 In our study, diarrhoea was the most frequent symptom, followed by abdominal pain. One of the limitations of our study was that we could not establish the genotype of the Giardia isolates, a factor that remains to be studied in relation to the symptoms, the course of disease and the response to treatment.
Chief among the microorganisms detected in cases of coinfection are the Campylobacter species, whose involvement in the aetiology of gastrointestinal illness is well known, and Blastocystis species, whose role in pathogenesis is controversial and requires further research. The most relevant among the frequent comorbidities identified in the sample were atopic dermatitis and lactose/fructose intolerance. Endemic countries have reported a significant association between the detection of this parasite and the severity of atopic dermatitis, and in our region there is evidence of a significant association with fructose malabsorption on account of the high prevalence of this combination.27,28 Carbohydrate malabsorption has a multifactorial aetiology, and the role of parasites as a potential trigger or in increasing severity has yet to be established.
In most patients, the initial treatment consisted of a standard regimen of metronidazole,29 and half of the patients were followed up until the infection resolved. The frequency of metronidazole resistance in Giardia is increasing,30 so it is important to be aware of the current situation of drug resistance in each geographical area. In our study, given that the resolution of symptoms is not documented in the health records of the patient, we were unable to determine whether the detection of the parasite during the post-treatment follow-up evaluation constituted a recurrence due to drug resistance, was due to lack of adherence to the prescribed treatment or was due to reinfection. The latter is particularly frequent in children aged less than 5 years.2
The potential association between the time of the year and the increase in the cases of giardiasis was corroborated, with the number of cases peaking in the late summer and early autumn (August–November). This may indicate waterborne transmission due to recreational aquatic activities (swimming pools, water parks) during the warm months.2 This has also been reported by Azcona-Gutiérrez et al.12
Paediatric giardiasis has a significant economic impact in terms of DHCCs. It must be taken into account that actual costs could be even higher than those calculated in our study due to information biases associated with the use of health records,31 due to which not all components used in the calculation of the total cost had the same sample size. The intervention that contributes the most to direct costs is hospital admission, as the single instance of hospital admission in our study accounted for 10% of the total DHCCs. With correct treatment, patients do not usually progress to severe presentations requiring hospital admission. The only patient admitted in our study had coinfection by rotavirus, which may have been the cause of this outcome. Most economic evaluations of health care interventions in Spain concern noncommunicable chronic diseases, with only a minority of analyses focusing on infectious diseases.32 With the exception of the study by Turrientes et al.,33 which only estimated the costs of the laboratory diagnosis of parasitic diseases overall without differentiating between them, there is no evidence on the economic impact of giardiasis or any other parasitic infectious disease in Spain. Our estimate is the first measurement of the overall direct health care costs generated by giardiasis, including medical attention (initial visit and follow-up), diagnostic procedures, treatments and hospital admission. This calculation of DHCCs is affected by care quality,34 as it can be influenced by inaccurate diagnoses and disease progression in patients due to inadequate management.
Lastly, the low sensibility of the techniques used for detection was a limitation in our study, as a greater number of cases would have been identified if qPCR were used as the first-line diagnostic test.
ConclusionsGiardiasis continues to be a prevalent disease in our region and should be considered a probable diagnosis in children presenting with diarrhoea and abdominal pain and/or atopic dermatitis or lactose/fructose intolerance. Appropriate management decreases the probability of disease progression, thus preventing hospital admission and reducing the economic impact of this disease in terms of health care costs.
FundingThe study received €1900 of funding through a IDOC/UCHCEU grant, Universidad CEU Cardenal Herrera (file: PARATRESCV_IDOC1820).
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Saura-Carretero Z, Villanueva-Alarcón M, Pérez-Olaso O, Aleixandre-Górriz I, Real-Fernández A, Sánchez-Thevenet P, et al. Giardiosis en población pediátrica de la provincia de Castellón: clínica e impacto. An Pediatr (Barc). 2021;94:278–284.
Previous presentation: partial results of this study were presented at the 11th European Congress on Tropical Medicine and International Health, September 2019, Liverpool, United Kingdom.

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals