



Several studies conclude that small for gestational age (SGA) children have a higher number of comorbidities, as well as a different hormonal profile compared to those with appropriate weight for gestational age (AGA). Thyroid hormones play an important role in growth and neurocognitive development. Thyroid function in SGA children is still not completely known.
ObjectivesTo compare the thyroid function of SGA children during the first 2 years of life with that in publications on thyroid function in other groups of infants, such as AGA and premature children, using the same methodology.
MethodsA cohort of 38 SGA children was obtained, in which the thyrotropin (TSH) values in blood were measured at different points in the development of the SGA child. The results were compared with a population of AGA children from Zaragoza and a population of premature children from Barcelona by comparing the means using a 2-tailed test.
ResultsA statistically significant difference (P < 0.05) was observed between the SGA children in our study and the AGA children older than 6 months, but not between the SGA children of the study and the population of premature infants.
ConclusionsSGA children have higher TSH values compared to AGA children older than 6 months. Therefore, it seems reasonable to establish a screening and a follow-up protocol in those SGA with high risk to develop thyroid dysfunction.
Múltiples estudios concluyen que los niños pequeños para la edad gestacional (PEG) tienen un número mayor de comorbilidades, así como un perfil hormonal diferente respecto a los niños con un peso adecuado para la edad gestacional (PAEG). Las hormonas tiroideas juegan un papel importante en el crecimiento y en el desarrollo neurocognitivo. La función tiroidea en los niños PEG es, hoy en día, incierta.
ObjetivosEl objetivo de este estudio es comparar la función tiroidea de los niños PEG durante los 2 primeros años de vida con publicaciones sobre función tiroidea en otros grupos de lactantes (PAEG y prematuros) que utilicen la misma metodología.
MétodosSe obtuvo una cohorte de 38 niños PEG, en los cuales se midieron los valores de TSH en sangre en distintos momentos del desarrollo del niño PEG. Los resultados se compararon con una población de niños PAEG de Zaragoza y una población de niños prematuros de Barcelona mediante pruebas de comparación de medias de contraste bilateral.
ResultadosSe ha observado una diferencia estadísticamente significativa (p < 0,05) entre los niños PEG de nuestro estudio y los niños PAEG mayores de 6 meses, no así entre los PEG del estudio y la población de prematuros.
ConclusionesLos niños PEG tienen valores de TSH superiores respecto a los niños PAEG mayores de 6 meses. Por lo tanto, parece razonable establecer un cribado y un protocolo de seguimiento en los PEG de mayor riesgo.
Small for gestational age (SGA) infants are those whose birth weight and/or length are more than 2 standard deviations (SDs) below the mean for gestational age and sex in the reference population.1 The diagnosis of SGA in a newborn infant requires, first of all, accurate determination of gestational age, secondly, the exact anthropometric measurements at birth (length, weight and head circumference) and, lastly, cut-off points based on reference data obtained from a representative population.2–4
In developed countries, 5% to 10% of neonates are SGA. In Spain, the proportion ranges from 3% to 5% of total births, and in the province of Alava, 3.5% of the total.5,6
The causes of SGA are not well established, but are known to include foetal, maternal, uteroplacental and environmental factors.2,3,5 Several studies have concluded that SGA infants have decreased serum levels of insulin-like growth factors (IGF-1 and IGF-2).7 There is evidence of an association between these decreased levels and defects in the growth hormone receptor in SGA infants.8,9
Accurate diagnosis is important due to the increased neonatal morbidity and mortality in this group of infants, in addition to an increased risk of developing certain diseases in childhood as well as adulthood.3–5 These include metabolic and endocrine disorders such as diabetes mellitus, dyslipidaemia and high blood pressure4,10 as well as growth and developmental disorders.2,4,5
Children born SGA can be classified into different categories: symmetric SGA refers to children in whom both weight and height are affected, while asymmetric SGA refers to children in whom either weight or height are affected, but not both.2,3 This classification is important, as it can guide the aetiological diagnosis and help predict the future risk of vascular disease2 and the response to growth hormone replacement therapy, with symmetric SGA associated with an increased frequency of short stature in adulthood3 and asymmetric SGA affecting weight associated with an increased frequency of perinatal hypoglycaemia.1
When it comes to the hormone profile of children born SGA, thyroid function is among the least studied axes in this population. Thyroid hormones are essential during the foetal period and in the first months of life for normal development of the nervous system and adequate growth. They also play a key role in bone, heart and lung maturation throughout the foetal period. Therefore, low levels in the first months of life can increase the risk of intellectual disability, short stature and metabolic disorders with irreversible consequences.10 However, from a clinical standpoint, there are no specific signs or symptoms at birth that would allow suspicion of thyroid abnormalities, which makes performance of screening tests for early diagnosis essential.11
Several studies show that thyroid function in preterm infants is usually altered due to the lower gestational age, resulting in increased requirements of thyroid hormones that in turn lead to higher serum concentrations of thyroid-stimulating hormone (TSH) and lower concentrations of triiodothyronine and thyroxine compared to term neonates.12 This is why monitoring thyroid function is recommended in the first years of life in children born preterm.13
However, few studies have analysed the thyroid hormone profile in SGA infants. Some have found that there are differences compared to children with birth weights appropriate for gestational age (AGA), but few have focused on the levels of TSH and thyroxine, and the published data are contradictory, so at present there is no indication for specific follow-up or thyroid function monitoring in SGA children.14
The aim of our study was to compare thyroid function in a sample of SGA infants with thyroid function in other subsets of infants: AGA infants and preterm infants.
Sample and methodsFor the purpose of sample selection, we defined SGA as a birth weight and/or length 2 or more SDs from the mean, taking as reference the growth charts of the nationwide study of growth conducted in Spain in 2010.15
The inclusion criteria were: Caucasian infant born between June 1, 2013 and June 1, 2015 in the department of labour and delivery of the Hospital Universitario Araba (HUA) meeting the case definition of SGA. The exclusion criteria were: non-white race, infants product of a multiple pregnancy, severe malformations, death within 24 hours of birth or not meeting the case definition of SGA.
Recruitment took place by consecutive sampling: any infant born in the labour and delivery department of the HUA in the period under study that met the inclusion criteria was a candidate for participation. We collected data on the following variables: gestational age, birth weight and length, sex, and serum TSH levels in SGA infants at different time points between age 4 months and 2 years.
Subsequently, we excluded cases with incorrectly documented or missing data for the variables under study, and obtained a final sample of 38 infants.
Having obtained the sample, we proceeded to the descriptive analysis of the explanatory variables using the mean, SD and median. We then compared TSH levels based on sex (SGA boys vs SGA girls), gestational age (SGA infants born at term vs preterm, defined as birth before 37 weeks), SGA symmetry (defining symmetric SGA as low weight and length and asymmetric SGA as alteration of only one of the two) and by the age of the child born SGA at the time of collection of the blood sample (age < 6 months vs age > 6 months). We made compared means using 2-tailed tests.
We also calculated the correlation coefficient for gestational age, birth length and weight and age at the time of blood sample collection, as these were quantitative variables, with values close to 1 or −1 indicating a strong correlation and values nearing 0 a weak correlation.
We also compared the results in our sample with the data published in other studies conducted in different populations. First, we compared our sample to a sample of healthy children born AGA in a study conducted by Cortés-Blanco et al.16 Specifically, we grouped serum TSH values for healthy children from Zaragoza by age group: 1 to 6 months (n = 18) and 6 months to 4 years (n = 30). We did the same with a sample of children born preterm in Barcelona in a study conducted by Clemente et al.17 This study published longitudinal data on serum TSH levels in a sample of healthy children born preterm (between 30 and 35 weeks of gestation). We compared samples using the Student t test for quantitative variables.
ResultsResults of the descriptive analysis of the study sampleThe TSH levels in SGA children in our sample ranged from 1 to 9 μU/mL. However, as can be seen in Table 1, the sample mean was 3.68 μU/mL, with a SD of 1.88 μU/mL and a median of 3 μU/mL.
Thyroid-stimulating hormone levels in children born small for gestational age between 4 months and 2 years of life.
| TSH level (μU/mL) | SGA, n | SGA, % |
|---|---|---|
| 1-3 | 20 | 52.63 |
| 3-5 | 14 | 36.84 |
| 5-7 | 2 | 5.26 |
| 7-9 | 2 | 5.26 |
SGA, children born small for gestational age; TSH, thyroid-stimulating hormone.
The table presents the absolute frequency and percentage distribution of the total sample of children born SGA by range of serum TSH levels.
Fig. 1 presents the mean serum TSH values in children born SGA categorised based on the variables under study (sex, gestational age, symmetry and age at time of sample collection).
Results by sex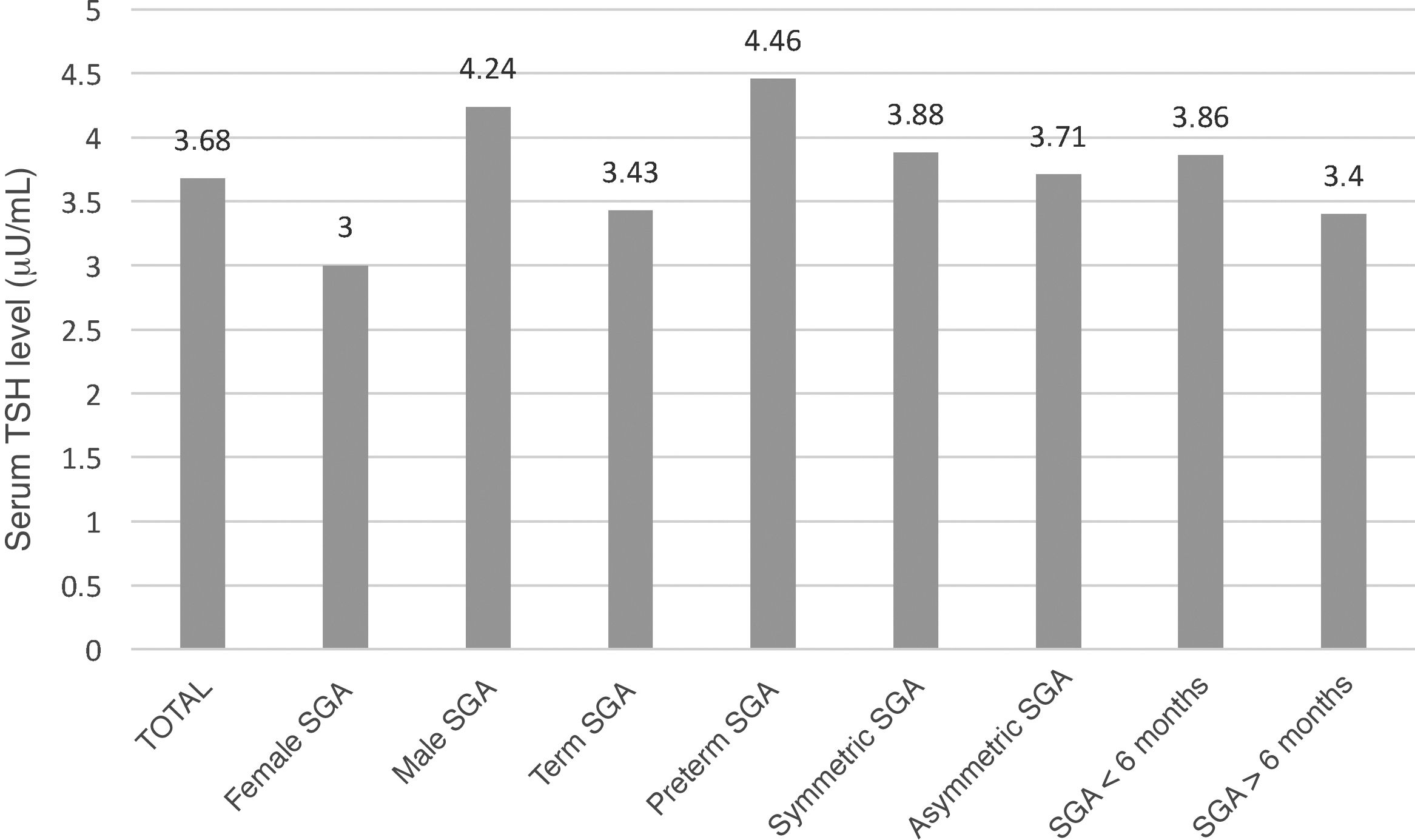
The mean TSH level in SGA boys was 4.24 μU/mL, with a SD of 1.79 μU/mL and a median of 4 μU/mL. In contrast, the mean TSH values in SGA girls ranged from 1 to 8 μU/mL, with a mean of 3 μU/mL, a SD of ±1.8 μU/mL and a median of 3 μU/mL.
We found statistically significant differences based on sex in the serum TSH levels of children born SGA in the catchment population of the health area of Alava (OSI Araba) aged 3 months to 2 years (P < 0.05). Thus, we can state that in our sample of children born SGA, boys had higher serum TSH levels compared to girls.
Results by gestational age groupThe mean TSH level in children born SGA at term was 3.43 μU/mL, with a SD of 1.78 μU/mL and a median of 3 μU/mL. In contrast, children born SGA and preterm had a mean serum TSH level of 4.46 μU/mL, with a SD of 1.86 μU/mL and a median of 4.5 μU/mL.
The correlation coefficient for the association between the gestational age of SGA infants and their serum TSH values was −0.19, indicative of a weak inverse correlation. That is, the lower the gestational age at birth, the higher the serum TSH levels in the first months of life.
Results based on anthropometric measurementsThe mean TSH level in the symmetric SGA group was 3.88 μU/mL, with a SD of 1.62 μU/mL and a median of 5 μU/mL. In contrast, in the asymmetric SGA group the mean was 3.71 μU/mL, with a SD of 2.02 μU/mL and a median of 3.5 μU/mL.
The correlation coefficients for the association between the serum levels of TSH in SGA children and their birth length and weight were −0.15 and −0.12, respectively. In other words, a low birth length/weight seems to predispose infants to decreased serum TSH levels in the early months of life.
Results based on age of children born SGAThe proportion of children born SGA aged less than 6 months was 58%, compared to 42% of children born SGA aged more than 6 months. The mean TSH level in SGA infants aged less than 6 months was 3.86 μU/mL, with a SD of 1.74 μU/mL and a median of 4 μU/mL. The mean TSH level in children born SGA aged more than 6 months was 3.4 μU/mL, with a SD of 2.16 μU/mL and a median of 3 μU/mL.
We did not find statistically significant differences in TSH levels between children born SGA aged less than 6 months and those aged more than 6 months at the time of collection of the blood sample (P > 0.05). Nevertheless, the correlation coefficient for the association between the current age of children born SGA and their serum TSH levels was −0.16. Thus, serum TSH levels in children born SGA tend to decrease with age.
Results of comparing TSH levels in the study sample with other paediatric samplesFirst, we compared the results in our sample with data obtained in healthy children in Zaragoza published by Cortés-Blanco et al.16 On one hand, we compared serum TSH levels in SGA infants aged less than 6 months in our sample with those of healthy children from Zaragoza aged 1 to 6 months, and on the other, we compared the levels in children born SGA in our sample aged more than 6 months with those in healthy children from Zaragoza aged 6 months to 4 years.
We did not find statistically significant differences in serum TSH levels in SGA infants in our sample compared to healthy infants aged 1 to 6 months in the Zaragoza sample (P > 0.05).
In contrast, we did find statistically significant differences in serum TSH levels between children born SGA aged more than 6 months in our sample and the healthy children aged 6 months to 4 years in the Zaragoza sample (P < 0.05).
Then, we compared the results in our sample with data obtained in the study of healthy children born preterm conducted in Barcelona by Clemente et al.17 To do so, we compared the groups of infants aged 4 and 6 months in the Barcelona study to the group of SGA infants aged less than 6 months in our sample, and also the groups aged 9 and 12 months in the Barcelona study with children born SGA aged more than 6 months in our sample.
We did not find statistically significant differences in TSH levels in the comparison of children in either of these age groups.
DiscussionOur study found statistically significant differences in the sample of children born SGA based on sex. It seems that boys born SGA tend to have higher serum levels of TSH compared to girls. This is consistent with the results of several studies that suggest that male infants are at increased risk of transient hyperthyrotropinaemia and transient hypothyroxinaemia in the early years of life.18–20
On the other hand, we identified gestational age at birth as a possible predictor of hyperthyrotropinaemia in children born SGA in the OSI Araba, although the association between these variables was weak. This was similar to the results of previous studies that have found differences in TSH levels between term and preterm infants, with a higher risk of hypothyroidism in the latter.12,13,21,22
When it comes to anthropometric values, some studies in the previous literature suggest that low birth weight is a risk factor for thyroid disorders,21,23 while others did not find an association between anthropometric values at birth and TSH levels in childhood.20 In our study, we found a weak association between the birth weight and length and TSH values, although we did not find statistically significant differences based on the symmetry of SGA.
We ought to highlight that TSH values varied between groups, yet they were in the normal range in 50% of the cases, so it may be worth assessing the clinical relevance of the observed differences.
As for the comparison of our sample to samples in other infant populations, we found that children born SGA in the OSI Araba had higher serum levels of TSH in the first years of life compared to healthy children in Zaragoza. Thus, while serum TSH levels tended to decrease from 6 months of age in children born AGA, they remained elevated for longer in children born SGA in the OSI Araba. The evidence on the association between SGA and thyroid disorders is insufficient, but previous studies have found that a birth weight of less than 2000 g was associated with an increased risk of hyperthyrotropinaemia in the long term,22,24 an elevation that could in turn increase the risk of developing hypothyroidism and cardiovascular problems at later ages.14
On the other hand, when we compared the sample of SGA infants in our study to the sample of preterm infants, we did not find statistically significant differences at any age. Therefore, we may conclude that the risk of thyroid disorders is similar in SGA infants and in preterm infants. Several studies have found that preterm SGA infants have higher serum TSH levels compared to preterm AGA infants,14 and therefore thyroid function in these infants should be monitored in the first months of life.
The main limitation of the study was the lack of a group of AGA infants born in the OSI Araba in the same time interval and with collection of data under the same circumstances for comparison with the SGA sample. Due to this lack, we collected information from studies conducted on AGA children in other regions, which may come from populations whose characteristics differ from the catchment population of the OSI Araba. We also ought to mention that the sample size was small, which may affect the validity of the results.
ConclusionAs noted above, the factors that seem to have an effect on the development of increased TSH levels in infants born SGA are:
- -
Male sex.
- -
Lower gestational age at birth seems to be associated with an increased risk of thyroid disorders.
- -
A low birth length and/or weight relative to the reference population seems to increase the risk of thyroid disorders in SGA infants.
The main conclusion of our study is that SGA infants have higher thyroid hormone requirements in the long term, similar to those of preterm infants. That is, our findings suggest that the risk of hyperthyrotropinaemia in SGA infants is similar to the risk in preterm infants, possibly leading to an increased frequency of thyroid abnormalities that may give rise to chronic and irreversible diseases in the future.
Taking these similarities into account, we propose the following:
- -
Screen TSH levels in SGA infants, with monitoring of thyroid function as needed in male infants and infants born at lower gestational ages or with very low birth weight or length, similar to the follow-up performed in preterm infants.
- -
Assess the need for thyroid hormone replacement therapy in SGA infants at increased risk of developing thyroid disorders or those that do not exhibit adequate catch-up growth.
The study was funded by a global medical grant from Pfizer, awarded in 2012.
Conflicts of interestThe authors received a global grant from Pfizer for performance of this study in year 2012.
Please cite this article as: González IF, Maeso-Méndez S, Miranda AS, del Hoyo Moracho M, Blázquez IL, López ID. Diferencias en la función tiroidea de los pequeños para la edad gestacional y los de peso adecuado. ¿Es normal la función tiroidea de los recién nacidos pequeños para la edad gestacional? An Pediatr (Barc). 2021;95:330–335.
