



Point-of-care ultrasound (POCUS) has become a key tool in the diagnosis and treatment of critically ill children and infants in emergency and intensive care settings.1,2 However, when it comes to interfacility transport, the available evidence is too scarce to support its use.3 We present the results of a descriptive study on the use of POCUS in the interfacility transport of critically ill neonatal and paediatric patients that evinced its usefulness.
We collected data on the POCUS examinations performed by a paediatric and neonatal advanced life support land transport team of the medical emergency response system of Catalonia, Spain, between November 1, 2019 and February 29, 2020. The data were collected prospectively by the paediatricians who performed the examinations, who entered the information in a database created for the purpose. All had undergone a theoretical and practical training on POCUS and had experience in the stabilization and transport of critically ill paediatric and neonatal patients. The variables under study included demographic characteristics, initial diagnosis, main compromised system, setting where the POCUS was performed, ultrasound probes and settings used, duration of POCUS, regions examined with POCUS, POCUS protocol, POCUS findings, final diagnosis and impact of findings on patient management. Images were obtained with a SonoSite Edge II® ultrasound system, linear transducers (13−6 MHz) and sector transducers (8−4 and 5−1 MHz).
There were 270 patient transports in the period under study. Twenty-six ultrasound examinations were performed in a total of 23 patients (8.5%). Table 1 summarises the main clinical and demographic characteristics of the patients, and Table 2 the main findings of POCUS. Fourteen POCUS examinations (53.8%) were performed in the ambulance and 12 (46.2%) in the referring hospital, without significant differences in patient characteristics between these groups. The median duration of POCUS examinations was 5 min (range, 3–10). The findings of POCUS led to changes in the diagnosis or management of the patients in 53.8% cases (n = 14): drainage of pneumothorax in 3, stepping up of haemodynamic support in 3 (administration of fluids and/or adrenergic agonists), optimization of ventilation after ruling out pneumothorax in 3, avoidance of volume expansion in 2 patients due to absence of signs of hypovolaemia and of performance of a chest radiograph in 1 patient, and a change in diagnosis in 2 patients.
Main clinical and demographic characteristics of patients and transport events.
| Patients with US n = 23 | Patients without US n = 247 | P | |
|---|---|---|---|
| [0,1–4]Demographic variables | |||
| Age, median (range) | 85 days (4 h–6 years) | 66 days (1.5 h–15 years) | .80 |
| Transport to neonatal units, n (%) | 8 (34.8%) | 62 (25.1%) | [1.0].31 |
| Transport to paediatric units, n (%) | 15 (65.2%) | 185 (74.9%) | |
| [0,1–4] | |||
| [0,1–4]Clinical diagnosis | |||
| Bronchiolitis, n (%) | 5 (21.7%) | 89 (36.0%) | .16 |
| Septic shock, n (%) | 4 (17.4%) | 1 (0.4%) | < .001 |
| Other types of shock, n (%) | 5 (21.7%) | 0 (0.0%) | < .001 |
| Neonatal respiratory distress, n (%) | 3 (13.0%) | 7 (2.8%) | .013 |
| Other, n (%) | 6 (26.1%) | 150 (60.7%) | .001 |
| [0,1–4] | |||
| [0,1–4]Transport variables | |||
| Time to stabilization in minutes, median (range) | 39 (21−129) | 45 (6−221) | .72 |
Time to stabilization: time elapsed between arrival to and departure from the sending hospital.
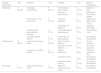
Important findings of performed ultrasound scans (n = 26).
| Detected compromise | n (%) | Indication | n (%) | Findings | n (%) | Effect on management |
|---|---|---|---|---|---|---|
| Respiratory | 14 (53.8%) | Suspected pneumothorax | 6 (23.1%) | Confirmation of pneumothorax | 3 (11.5%) | Decision to drain |
| Absence of pneumothorax | 3 (11.5%) | Optimization of ventilation settings | ||||
| Examination of lung parenchyma | 4 (15.4%) | Change in diagnosis | 2 (7.7%) | Diagnosis of RDS (1) and TTN (1) | ||
| Confirmation of diagnosis | 2 (7.7%) | Diagnosis unchanged | ||||
| Monitoring after pneumothorax drainage | 2 (7.7%) | Correct drainage of pneumothorax | 2 (7.7%) | Avoided chest X-ray | ||
| Suspected pleural effusion | 2 (7.7%) | Confirmation of pleural effusion | 2 (7.7%) | No change in management | ||
| Cardiovascular | 10 (38.5%) | Assessment of volume status | 4 (15.4%) | Signs of volume depletion | 2 (7.7%) | Volume expansion |
| No signs of volume depletion | 2 (7.7%) | No volume expansion | ||||
| Assessment of cardiac function | 6 (23.1%) | Systolic dysfunction | 1 (3.8%) | Initiation of vasoactive drug | ||
| Diagnosis of VSD | 1 (3.8%) | No change in management | ||||
| Adequate cardiac function | 4 (15.4%) | No change in management | ||||
| Neurologic | 2 (7.7%) | Suspected intracranial lesion | 2 (7.7%) | Absence of intracranial lesion (TUS) | 2 (7.7%) | No change in management |
RDS, respiratory distress syndrome; TTN, transient tachypnoea of the newborn; TUS, transfontanellar ultrasound; VSD, ventricular septal defect.
Previous evidence of POCUS demonstrates that the contribution of its findings to clinical decision-making can improve patient outcomes.4 It has also proven useful in establishing the indication for certain procedures (such as drainage of pneumothorax) or changing the diagnosis.
The scarce evidence on the use of POCUS during transport focuses on neonatal patients,5 but only one third of the patients that underwent POCUS examination in our study were newborn infants, which highlights the importance of this approach in paediatric patients, too.
There are limitations to the use of POCUS during patient transport. Chief among them is the need of specialised training to prevent errors in its interpretation. However, qualification of previously untrained staff can be achieved in a fairly reasonable time with an appropriate training format.6 Another limitation is the need to weigh the relevance of the information that may be obtained with this technique against the delay in transport that results from its use. Since transport is a very different context compared to the critical care setting (fewer staff and resources, smaller spaces and crucial importance of the time allocated to tasks), POCUS should be reserved for cases in which, given a specific suspicion, the findings may result in a change in management, clinical situations of which shock may be one example, a condition that was not assessed with the help of POCUS in only one affected patient in our study.
The main limitation of our study is its small sample size, which calls for caution in the interpretation of its results. The low proportion of patients that underwent a POCUS examination could be due to the fact that the period under study included the bronchiolitis season. Point-of-care ultrasound during transport is not indicated in patients with bronchiolitis unless it is required for differential diagnosis or to rule out complications (pneumothorax). Another limitation was that we were unable to determine whether the changes in diagnosis or management resulting from POCUS yielded actual benefits in terms of length of stay, mortality or the severity score at the time of admission.
In conclusion, our findings show that a significant proportion of patients in whom POCUS during transport is indicated may benefit from performance of this technique without an associated increase in the time to stabilization. The indication of POCUS must be determined on a case-by-case basis to avoid delays in transport. Patients with respiratory or haemodynamic compromise benefitted most from the technique. Performance of POCUS during transport needs to be documented to confirm and strengthen these findings.
Please cite this article as: Subirana Campos L, Renter Valdovinos L, Oller Fradera O, Garcés Montolio L, Gómez Rodríguez J. Utilidad de la ecografía clínica en el traslado interhospitalario del paciente crítico pediátrico y neonatal. An Pediatr (Barc). 2021;95:201–203.
