
In 2015, the Patient Experience team was created in our hospital with the aim of incorporating the perspective of patients and their families to the operations of the centre. We reviewed how families experienced the care process in our hospital and identified the initial communication of the diagnosis as an opportunity for improvement. This led to the development of a guideline1 aimed at all care providers, including those in clinical practice but also those offering psychosocial and spiritual support, to assist with the aspects that ought to be taken into account before, during and after the initial communication of bad news. To disseminate the contents of this guideline to professionals and therefore improve patient care, the team in the simulation programme of our hospital designed a 2-day face-to-face workshop that we will be describing in this article.
Day 1 of the workshop focuses on learning and practicing (through role play techniques) the Bridge model of interpersonal relations.2 This model describes 4 relational styles based on 2 axes (active/reflexive and rational/emotional). The goal is to adapt our communication style to the style used by the person we are speaking to. On day 2, students participate in simulated scenarios acted out by professional actors. Each scenario is designed based on the profession and work setting of each participant to approximate their real-world experience and with the purpose of addressing one or more specific challenges. After each scenario, participants hold a group discussion (debriefing) led by experienced facilitators to reflect not only on the outcomes of their actions, but also on the underlying cognitive rules and reasoning that lead to them.3
We conducted a descriptive and inferential study with the aim of assessing the perceived impact of this training. We followed the model described by Kirkpatrick4 to evaluate the effect of the training. We obtained anonymous written assessments from the participants at 3 time points. The assessment before the training evaluated the baseline of each participant. The assessment immediately following the training assessed how participants perceived the training (Kirkpatrick level 1) and the degree of learning in the training (level 2). The assessment 6 months after the training evaluated the perceptions of participants after having communicated bad news in real life (level 3). The study was approved by the Clinical Research Ethics Committee of the hospital.
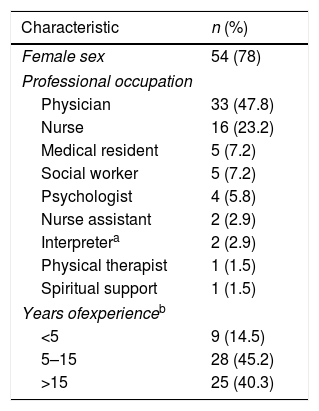
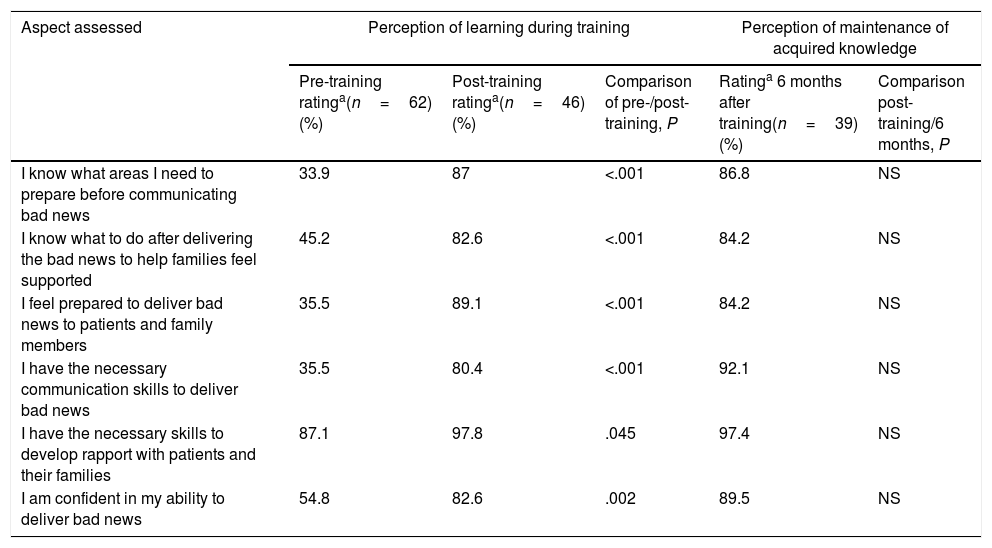
The study sample included the questionnaires of 69 professionals that participated in the training in 4 workshops delivered between September 2017 and July 2018 (Table 1). Participants expressed a high level of satisfaction with the training (Kirkpatrick level 1), with ratings of more than 4 points (out of 5) in every assessed aspect. As can be seen in Table 2, participants considered that they had acquired knowledge on how to deliver bad news in the training, and that this knowledge persisted 6 months later (level 2). When it came to real-world experience (level 3), more than 70% of participants reported they were able to apply 3 key behaviours: preparing the setting, identifying the interpersonal communication style and supporting the family.
Main characteristics of the 69 participants in the training.
| Characteristic | n (%) |
|---|---|
| Female sex | 54 (78) |
| Professional occupation | |
| Physician | 33 (47.8) |
| Nurse | 16 (23.2) |
| Medical resident | 5 (7.2) |
| Social worker | 5 (7.2) |
| Psychologist | 4 (5.8) |
| Nurse assistant | 2 (2.9) |
| Interpretera | 2 (2.9) |
| Physical therapist | 1 (1.5) |
| Spiritual support | 1 (1.5) |
| Years ofexperienceb | |
| <5 | 9 (14.5) |
| 5–15 | 28 (45.2) |
| >15 | 25 (40.3) |
Kirkpatrick Level 2 assessment of participants before, immediately after and 6 months after the in-person training, and comparison of knowledge before and immediately after training (learning during training) and immediately after training versus 6 months after training (maintenance of acquired knowledge).
| Aspect assessed | Perception of learning during training | Perception of maintenance of acquired knowledge | |||
|---|---|---|---|---|---|
| Pre-training ratinga(n=62) (%) | Post-training ratinga(n=46) (%) | Comparison of pre-/post-training, P | Ratinga 6 months after training(n=39) (%) | Comparison post-training/6 months, P | |
| I know what areas I need to prepare before communicating bad news | 33.9 | 87 | <.001 | 86.8 | NS |
| I know what to do after delivering the bad news to help families feel supported | 45.2 | 82.6 | <.001 | 84.2 | NS |
| I feel prepared to deliver bad news to patients and family members | 35.5 | 89.1 | <.001 | 84.2 | NS |
| I have the necessary communication skills to deliver bad news | 35.5 | 80.4 | <.001 | 92.1 | NS |
| I have the necessary skills to develop rapport with patients and their families | 87.1 | 97.8 | .045 | 97.4 | NS |
| I am confident in my ability to deliver bad news | 54.8 | 82.6 | .002 | 89.5 | NS |
NS not significant.
We would like to highlight 3 elements of this training. First, a high appreciation of training in small groups including professionals in different fields and with different professional roles was expressed both in the debriefings and in the questionnaires. The shared reflection on situations that could happen in real life allowed participants a better understanding of the role played by each professional and facilitates the coordination of work.
Secondly, the scenarios played out by actors allowed a life-like experience that is very powerful for the purposes of reflection and learning. Other authors have reported beneficial effects of using actors, mostly based on the degree of realism achieved in the performance, the contribution of actors to the debriefing from the perspective of the family, how they conveyed emotions and their adaptability and ability to improvise.5 Meyer et al. found that participants reported feeling better equipped to have difficult conversations, improved relational skills and decreased anxiety.6
Lastly, we want to highlight the novel approach of incorporating relational styles to communication in the health care setting. Although there are many psychometric tools to assess personality profiles, we opted for this model because it is easy to assimilate in a short period of time, specifically addresses individual relational styles, could be useful in other contexts and facilitates the integration of the concepts of individualised and family-centred care.
The main limitations of this study were that not all participants submitted every assessment and that the assessments of learning and changes in behaviour were subjective, based on the perceptions of the participants, and not on an objective evaluation.
In conclusion, we describe a training programme based on simulated scenarios that provides professionals with tools to facilitate the initial communication of bad news. Professionals expressed a high level of satisfaction after the training and considered that they had acquired relevant knowledge and that they were able to apply this knowledge to real-world situations.
Please cite this article as: Claret Teruel G, Quintillá Martínez JM, Nadal Miquel D, Aláez Vasconcellos C, Pérez Payarols J. Construyendo buenas conversaciones mediante simulación: impacto percibido tras una formación sobre la comunicación de malas noticias. An Pediatr (Barc). 2020;92:372–374.
Previous presentations: This study was presented in part at the III Congress of the Sociedad Española de Paliativos Pediátricos (March 2019), the 7th Congress of the Sociedad Española de Simulación Clínica y Seguridad del Paciente (April 2019) and the 25th Annual Meeting of the Society in Europe for Simulation Applied to Medicine, SESAM (June 2019).

Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals