




With appointment schedules usually fully booked, unscheduled visits pose a significant problem. The phenomenon of urgent visits has been described both in primary care health care centres1 and hospitals.2 Some authors have suggested that this trend is partly due to social factors (excess fear and information of parents, familial stress, work schedules, or convenience), even discussing it in terms of “24h clinics,” “social habit” or “pseudo-emergencies.”1–3 Our aim was to describe the characteristics of appointments requested as urgent to assess their impact on health care delivery and the characteristics of patients and their presenting problems, searching for other possible determinants.
We designed an observational, descriptive prospective study. It was conducted over ten months (November 29, 2014 to September 30, 2015) in a clinic of the Centro de Salud Ponferrada IV (four morning shifts and one afternoon shift with a patient load of 900–1000). This is an urban health care centre that has two paediatrician offices and one paediatric nursing office. Patients are not triaged.
We defined an urgent appointment as one that was requested when none were available due to the calendar being full at the time. These appointments are squeezed in by the administrative staff, who are not authorised to inquire into the reason for the visit. We collected information regarding the visit (day and time; month and week; visit to the clinic, after-hours clinic or hospital emergency department in the week prior), the patient (age, preterm birth, past medical history) and the consultation (reason for visit, diagnosis, referral to hospital, complications).
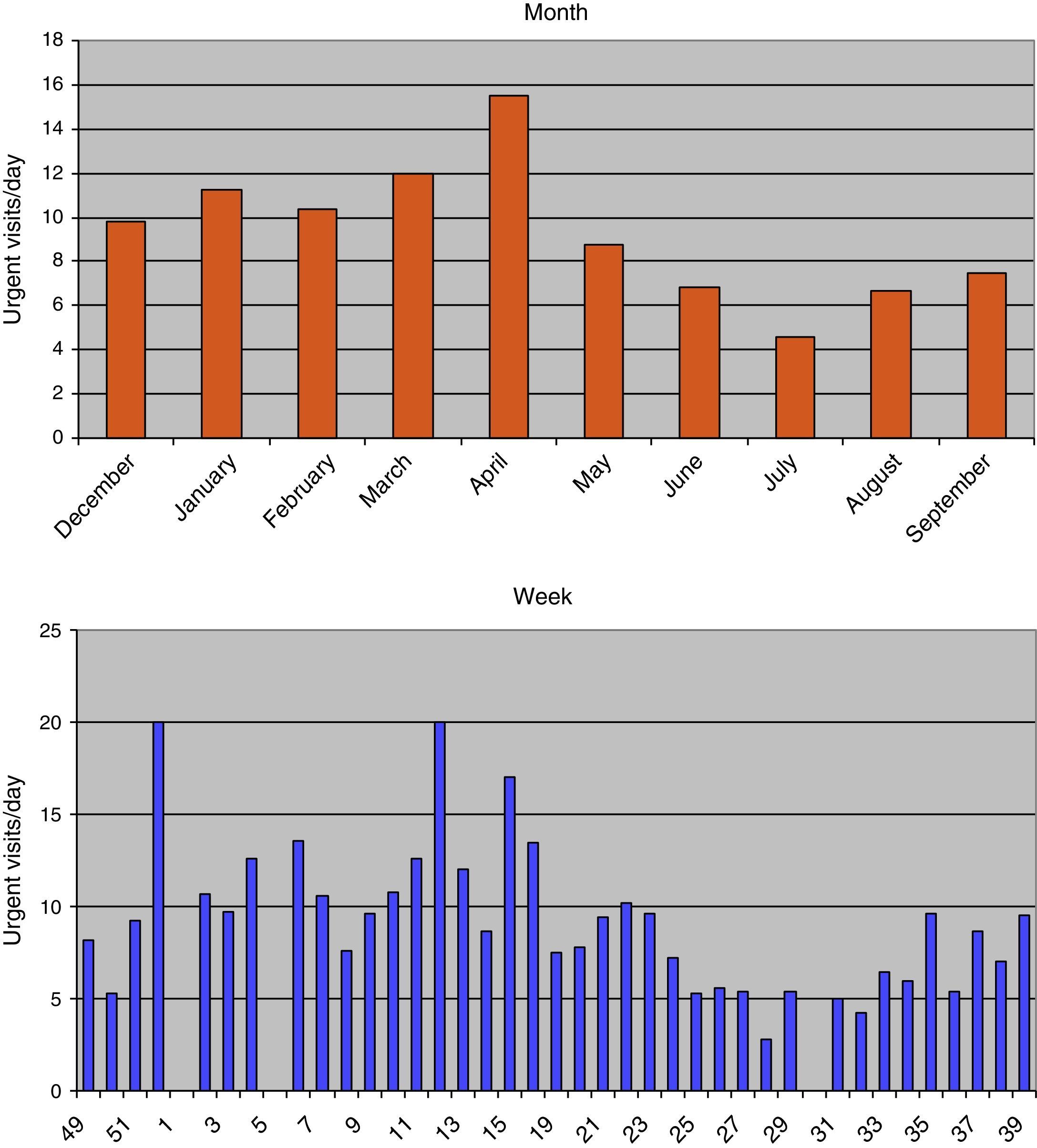
There were 1469 appointments requested as urgent among the total of 5366 appointments held (27%). The mean number of urgent appointments per day was 8.8±4.8 (range, 27; interval 2–29). Urgent appointments were most frequent in the month of April (15.5 emergencies/day) and weeks 52 and 12 (20 emergencies/day) (Fig. 1). When it came to weekdays, they occurred most frequently on Mondays and Tuesdays (10.7 and 10.8 emergencies/day). The most common hours were 9AM to 12PM for the morning shift and 4 PM to 6 PM for the afternoon shift.
Of the patients seen urgently, 319 (22%) had received care previously: 143 at the clinic, 136 at the after-hours clinic and 40 at a hospital emergency department. By sex, 738 were male and 731 female, and their mean age was 47.5±4.4 months (0–11 months, 355; 12–35 months, 401; 36–71 months, 347; 72–167 months, 366).
Of all the patients, 1234 (84%) did not have a chronic disease. The most frequent one consisted of recurrent episodes of wheezing in infants (151). There were also cases of allergic asthma (13), celiac disease (6), complete heart block (6) or diabetes (5), among others. Forty-six patients had been born preterm. The most frequent reasons for consultation were fever (334) and coughing (278), and the most frequent diagnoses were upper respiratory tract infection (269), pharyngotonsillitis (184) and laryngitis (115) (Table 1). Only 26 patients were referred to the hospital (2%). There were no complications.
Reasons for the visit and subsequent diagnoses.
| Reason for visit | Diagnosis | ||
|---|---|---|---|
| Fever | 334 | URTI | 269 |
| Cough | 278 | Pharyngotonsillitis | 184 |
| Rash | 100 | Laryngitis | 115 |
| Request for checkup | 93 | Request for checkup | 93 |
| Nasal discharge | 75 | Gastroenteritis | 85 |
| Prescriptions | 74 | Prescriptions | 74 |
| Vomiting | 53 | No disease | 66 |
| Checkup | 43 | Acute otitis media | 61 |
| Administrative | 39 | Conjunctivitis | 52 |
| Ear pain | 37 | Checkup | 43 |
| Fall | 35 | Administrative | 39 |
| Diarrhoea | 33 | Bronchitis | 36 |
| Eye discharge | 28 | Atopic dermatitis | 30 |
| Red eye | 27 | Influenza | 24 |
| Painful swallowing | 25 | Pneumonia | 21 |
| Concussion | 22 | Constipation | 16 |
| Mass | 21 | Hives | 13 |
| Abdominal pain | 20 | Hay fever | 13 |
| Irritability | 14 | Puncture wound | 10 |
| Headache | 9 | Bronchiolitis | 8 |
| Limping | 9 | Physiological reflux | 8 |
| Painful urination | 9 | Balanitis | 5 |
| Joint pain | 8 | Adenopathy | 5 |
| Behavioural change | 6 | Stye | 4 |
| Hearing loss | 3 | Cerumen | 1 |
With urgent appointments amounting to nearly one third of the total, we continue to observe the increasing trend in the frequency of appointments requested as urgent relative to previous studies.1 Also consistent with the literature, the demand tends to concentrate on specific days and hours around the middle of the day. Furthermore, while seasons influenced the frequency, provider leaves or vacations seemed to have a greater impact. A large number of patients had received care prior to the visit, a recurrence that has been described in other settings.2 We observed that urgent visits were more frequent the younger the patients, with infants constituting the group with the most urgent appointments, consistent with other studies.1,4
We categorised the factors that lead to these appointments into predisposing, facilitating or of necessity.3 A previous history of disease could be included in the latter. However, we found that the prevalence was the same as in the general population.
The symptoms and signs that generated the demand were common and well known, and similar to those found in previous studies. They usually corresponded to nonsevere diseases that rarely required referral to the hospital, with evidence of a decrease in the number of hospital admissions concurrent to the increase in urgent visits.2 One remarkable finding was the use of urgent appointments for issues unrelated to health (prescription requests, administrative procedures or requesting other appointments), as was the fact that no disease was detected in the patient in many instances. In the first case, we propose that such visits be prevented in cooperation with the administrative department.
Measures to control the frequency of unscheduled appointments have been proposed and put into practice. They have been efficacious at times, although they are difficult to implement and involve the use of resources.5 The literature has also emphasised the importance of the family as an active agent in health care processes and decision making, including specific interventions such as urgent visits.6
Based on our observations, there is no clinical justification for the magnitude of the phenomenon of urgent appointments, and our study corroborated the impact that such visits have in health care delivery.
Please cite this article as: Mata Zubillaga D, Fernández Miaja M, Cobo Pacios MV. Citas solicitadas como urgentes: impacto en la consulta y características clínicas. An Pediatr (Barc). 2016;85:213–214.
