


Antimicrobial resistance is a worldwide threat to public health. Acute respiratory tract infections are the main reason for antibiotic prescription in the Spanish paediatric population. The aim of the study was to describe the frequency of antibiotic prescription and their pattern of use in acute respiratory tract infections diagnosed in children in primary care in Aragón (Spain).
MethodologyA study was conducted over a 1-year period on children between 0 and 14 years-old, recording all episodes of acute otitis, acute pharyngotonsillitis, non-specific upper respiratory infection, and acute bronchitis. The proportion of episodes within each diagnosis receiving an antibiotic prescription was calculated, and the prescribing pattern was determined.
ResultsHalf (50%) of the children in Aragón were diagnosed with a respiratory tract infection during the study period. Non-specific upper respiratory infection was the most frequent diagnosis. An antibiotic was prescribed in 75% of pharyngotonsillitis episodes, 72% of otitis, 27% of bronchitis, and 16% of non-specific upper respiratory infections. Broad spectrum antibiotics, mainly amoxicillin and amoxicillin-clavulanic, were predominantly prescribed.
ConclusionsAntibiotic prescription in respiratory tract infections in children was generally high, and the choice of antibiotics was probably inappropriate in a high percentage of cases. Therefore, an improvement in antibiotic prescription in children appears to be needed.
La resistencia a antimicrobianos representa una amenaza para la salud pública mundial. Las infecciones respiratorias agudas son el principal motivo de prescripción antibiótica en la población pediátrica española. El objetivo del estudio fue describir la frecuencia de prescripción y el patrón de utilización de antibióticos en infecciones respiratorias agudas, diagnosticadas en atención primaria, en la población pediátrica de Aragón.
Material y métodoSe incluyeron los episodios de otitis aguda, faringoamigdalitis aguda, infección respiratoria superior inespecífica y bronquitis aguda, registrados durante un año, en niños de 0-14 años. Se calculó la proporción de episodios que recibieron antibiótico, por diagnóstico y grupo de edad, y describió el patrón prescriptor.
ResultadosEl 50% de los niños fueron diagnosticados de infección respiratoria aguda durante el periodo de estudio, siendo la infección respiratoria superior inespecífica la más frecuente. Se prescribió un antibiótico en el 75% de las faringoamigdalitis, 72% de otitis, 27% de bronquitis y 16% de infecciones respiratorias superiores inespecíficas. Los antibióticos más prescritos fueron los de amplio espectro, principalmente amoxicilina y amoxicilina-clavulánico.
ConclusionesEl uso de antibióticos en infecciones respiratorias agudas pediátricas fue, en general, elevado, y la elección del tipo de antibiótico podría ser inadecuada en un porcentaje elevado de casos. Se considera necesaria una mejora en la práctica prescriptora de antibióticos en niños.
Antimicrobial resistance is a global health problem and is believed to be related to community use of antibiotics.1 There is evidence of a high rate of antimicrobial use in the Spanish paediatric population, and acute respiratory tract infections (ARTIs) are the main reason for their prescription,2 even though it has been demonstrated that antimicrobials typically provide little benefit in the treatment of these conditions.3 In Spain, the strategies that aim to address the problem of bacterial resistance include the recent development of several consensus guidelines on the management of paediatric infections.4,5 Yet a recent study showed that there is poor compliance with the recommendations in the choices of antibiotics for empirical treatment made by paediatricians in some autonomous communities like Aragón and La Rioja, which were evaluated together.4
The main aim of this study was to determine the frequency of antibiotic prescription and the pattern of use of these drugs for the treatment of ARTIs diagnosed in primary care in the paediatric population of Aragón.
Materials and methodsWe conducted a retrospective observational study of antibiotic prescription in cases of ARTI diagnosed in primary care in the paediatric population of Aragón between September 1, 2009 and August 31, 2010.
We collected diagnostic and prescription data from the OMI-AP database, which holds the electronic medical records of all individuals served by the Aragón public health system (98.6% of the population of Aragón).
We selected the records corresponding to patients 0–14 years of age diagnosed with one of the following ICPC codes: acute otitis media (H71), strep throat (R72), nonspecific upper respiratory tract infection (R74), acute tonsillitis (R76) and acute bronchitis/bronchiolitis (R78). We combined the diagnoses coded R72 and R76 under the label “acute pharyngotonsillitis” because during the period under study, paediatricians in Aragón did not regularly use rapid tests allowing the differential diagnosis of streptococcal and viral pharyngotonsillitis.
Each record corresponded to a single episode or diagnosis, and included the anonymous code for the patient, the sex, date of birth, ICPC code and, if a prescription was made, the code corresponding to the prescribed antibiotic in the Anatomical Therapeutic Chemical (ATC) classification. We considered that a prescription was associated to an episode of disease if it was issued within 15 days after the diagnosis.
We classified the antibiotics according to the ATC/DDD 2010 Index of the World Health Organization (OMS).6
We described the frequency of ARTI and antibiotic prescription in the paediatric population during the year of the study. We also calculated the proportion of episodes treated by type of diagnosis and age group (<2 years, 2–4 years, 5–9 years and 10–14 years) to determine the existing pattern of prescription.
ResultsDuring the period under study, a total of 89800 children, with a mean age of 4.3 years and 48% of whom were female, were diagnosed with ARTI. The overall prevalence of diagnosis with ARTI in children in Aragón was 50%, and the prevalence was 75% in children younger than 2 years and 35% in children 10–14 years of age.
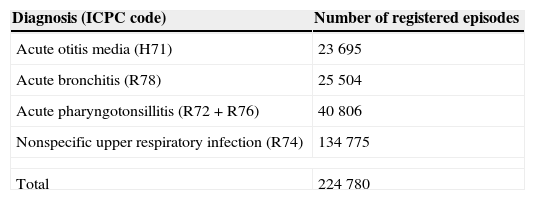
There were a total of 224780 episodes of ARTI. Table 1 shows the frequency of the diagnoses under study. Nonspecific upper respiratory tract infection (URTI) was the most frequent diagnosis (60% of the total recorded episodes), followed by pharyngotonsillitis (18%), otitis (11%) and acute bronchitis (11%).
Frequency of acute respiratory tract infections in children in primary care in Aragón during the period under study (September 2009–August 2010).
| Diagnosis (ICPC code) | Number of registered episodes |
|---|---|
| Acute otitis media (H71) | 23695 |
| Acute bronchitis (R78) | 25504 |
| Acute pharyngotonsillitis (R72+R76) | 40806 |
| Nonspecific upper respiratory infection (R74) | 134775 |
| Total | 224780 |
Antibiotics were prescribed in 34% of the total episodes of ARTI, and this proportion varied by diagnosis, with prescriptions given in 75% (n=30556) of pharyngotonsillitis, 72% (n=1730) of otitis, 27% (n=6962) of bronchitis and 16% (n=21297) of URTI episodes. The proportion of episodes treated in children younger than 2 years was lower for every diagnosis except otitis, for which antibiotics were prescribed in 75% of the episodes (Fig. 1). The percentage of acute pharyngotonsillitis episodes treated with antibiotics increased significantly with age, reaching 81% in children 10–14 years old. When it came to the antibiotics prescribed, amoxicillin and amoxicillin-clavulanic acid comprised over 70% of the total prescriptions (Fig. 2). Amoxicillin was prescribed in approximately half of the treated episodes of acute pharyngotonsillitis and URTI, while amoxicillin-clavulanic acid was frequently used to treat otitis and acute bronchitis. Narrow-spectrum penicillin was prescribed for 13% of the episodes of acute pharyngotonsillitis, and second and third generation cephalosporins were mostly used to treat cases of otitis (15% of the total episodes). Almost one fifth of the episodes of nonspecific URTI and acute bronchitis were treated with a macrolide.


Pattern of antibiotic prescription in treated episodes. The vertical axis represents the proportion of episodes of each diagnosis for which one of the antibiotics under study was prescribed. AP, acute pharyngotonsillitis; ns URTI, nonspecific upper respiratory tract infection; NS, narrow spectrum.
One-third of the episodes of acute otitis media, acute pharyngotonsillitis, nonspecific URTI or acute bronchitis diagnosed over a one-year period in the paediatric population of Aragón were treated with an antibiotic. There is evidence that Spain has one of the highest rates of antibiotic use in Europe, fundamentally of broad-spectrum antibiotics,7 and consequently it also has higher rates of antimicrobial resistance.8 The paediatric population, which is also affected by the situation, provides an excellent medium for the selection of resistant bacteria following the recent use of antibiotics,1 and their frequent contact with other children through attendance to child care centres facilitates the transmission of these pathogens. The rate of antibiotic prescription for treatment of ARTI in Spanish children has declined in recent years,4,9,10 probably due to the many interventions enacted across different settings. Nevertheless, the data we obtained suggests that the appropriateness of prescriptions still needs improving. The frequent antibiotic treatment of acute otitis and pharyngotonsillitis cases in children older than 2 years seen in this study suggests overprescription. Furthermore, the high proportion of nonspecific URTI and acute bronchitis episodes for which antibiotics were prescribed does not seem to be justified, as these frequently are self-limiting viral processes.5
The compliance of the prescribed treatments with the recommendations is generally low. Only 41% of the otitis cases were treated with amoxicillin, the first-line antibiotic for acute otitis media except for cases occurring in children younger than 6 months or with severe symptoms.4,5 The episodes of acute pharyngotonsillitis treated with penicillin V, the first-line treatment, amounted to 13% of the total. If we consider amoxicillin an alternative option because penicillin V in solution is not always well tolerated, the proportion of episodes that were treated correctly rises to 67%. It is worth noting that one-fourth of all treated episodes were managed with amoxicillin-clavulanic acid, an antibiotic that is only recommended as the first-line treatment of acute otitis media under specific circumstances,4 which does not justify the frequent use that we observed.
It is believed that the prescription of antibiotics to children is associated with parental satisfaction, fear of future complications, the paediatrician's communication skills and the paediatrician's perception of parental expectations.11,12 The pressure of the pharmaceutical industry or the scarcity or lack of preparations of particular drugs in the market, which could be interpreted as a commercial strategy, can also influence the decisions of clinicians.
Given the circumstances, we need to launch interventions aimed at reducing the rate of unnecessary prescriptions and improving the appropriateness of prescribed antibiotics. Some possible examples are the adoption of approaches like watchful waiting and delayed prescribing due to the uncertainty that characterises ARTIs, or the use of rapid testing to diagnose bacterial pharyngotonsillitis in every paediatric setting.13 We also need to promote continuing education and foster the awareness of healthcare professionals of their responsibility as prescribers and suppliers, and to involve parents in the process, correcting the false and widespread myths about respiratory diseases and the benefits of antibiotic prescription.
The main limitation of our study is that we did not have data on microbiological diagnoses or on comorbidities, which made it difficult to categorise prescriptions as appropriate or inappropriate. At any rate, it seems unlikely that these problems would account for the degree of noncompliance with current recommendations that we observed. On the other hand, the decision to determine the association of a prescription with an episode of disease based on prescription occurring within 15 days after the diagnosis may have biased our results, leading to under- or overestimation of the proportion of episodes treated with antibiotics. Still, we needed to define a criterion to associate dates of diagnosis with subsequent antibiotic prescriptions, so we decided on the described criterion taking into account the epidemiology of the diseases under study. Last of all, there is a certain time lag in the data we are presenting, and it is likely that the measures adopted in Spain in recent years to promote the sensible and appropriate use of antibiotics have had a positive effect on the pattern of prescription. Despite its potential limitations, there are strengths to our study, such as the usefulness of the information it contributes, as well as the value of the information source we used, which allowed us to simultaneously know the medical diagnosis and prescription given to the patient. We must underscore that conducting a study on the appropriateness of antibiotic prescription like the one we have performed in Aragón would be difficult in other Spanish autonomous communities, mostly due to the unavailability of data sources of these characteristics.
Reducing the problem of bacterial resistance in Spain calls for the development and implementation of measures for antibiotic stewardship. These measures should involve a greater allocation of human and material resources, time, and effort, engaging the collaboration of all the involved parties.
FundingThis study was funded by the Proyecto del Fondo de Investigación Sanitaria (Health Research Fund Project), Instituto de Salud Carlos III, FIS (PI10/01048).
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Malo S, Bjerrum L, Feja C, Lallana M, Poncel A, Rabanaque M. Prescripción antibiótica en infecciones respiratorias agudas en atención primaria. An Pediatr (Barc). 2015;82:412–416.
