

Lymphatic malformations (LMs) are a type of vascular anomaly characterised by dysplasia of lymphatic vessels leading to formation of cystic cavities filled with lymph. Their incidence is of 1 case per 2000–4000 births, and up to 80% of cases involve the head and neck.1,2 Although these malformations are benign, they can have functional or cosmetic repercussions, depending on their location, and even be life-threatening if they are located in critical areas. For many years, the mainstay of treatment of LMs was full surgical resection due to the misconception that they were malignant tumours; however, due to the risk of complications in these procedures and the development of immunotherapy and interventional radiology, the first-line treatment at present is conservative.3 We describe a series of cases in children aged less than 15 years with sequelae from the surgical management of LMs, operated between 2002 and 2022 in various hospitals and followed up in our vascular anomaly unit, which manages an average of 150 patients with LMs, isolated or as part of a larger syndrome, each year.
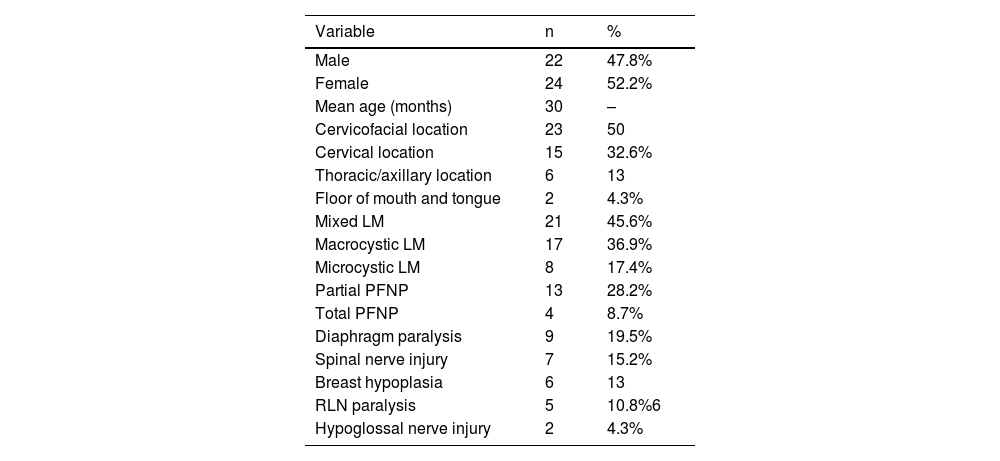
We included 46 patients (52% female) with a mean age at of 30 months at the time of surgery (range, 1–57), of who 80% were operated between 2002 and 2012, and the indication for surgery in every case was failure of sclerotherapy and absence of pharmacological treatment. Fifty percent of LMs were located in the cervicofacial region, 15 were restricted to the neck, 6 were in the thoracic/axillary region and 2 patients had LM in the floor of the mouth with involvement of the tongue. The most frequent type of malformation was mixed LM (n=21/46), followed by macrocystic LM (n=17) and microcystic LM (n=8). Of all complications, 87% were neurologic (40/46), most frequently peripheral facial nerve palsy (n=17), partial in most cases, caused by damage to the mandibular branch (13/17), and full in 4 cases (Fig. 1A). Nine patients had unilateral diaphragmatic paralysis due to phrenic nerve damage and 7 had sequelae due to spinal nerve injury, of who 3 required orthopaedic treatment for scapular winging (Fig. 1B). Five patients had unilateral recurrent laryngeal nerve injury and 2 patients impaired tongue motility due to hypoglossal nerve damage. The remaining complications (6/46; 13%) were physical deformities resulting from severe unilateral breast hypoplasia eligible for reconstruction (Fig. 1C). Table 1 summarises the characteristics of the case series.
, winged scapula resulting from spinal nerve injury (B) and right breast hypoplasia with significant loss of soft tissue (C).")
Characteristics of the patients under study (n=46).
| Variable | n | % |
|---|---|---|
| Male | 22 | 47.8% |
| Female | 24 | 52.2% |
| Mean age (months) | 30 | – |
| Cervicofacial location | 23 | 50 |
| Cervical location | 15 | 32.6% |
| Thoracic/axillary location | 6 | 13 |
| Floor of mouth and tongue | 2 | 4.3% |
| Mixed LM | 21 | 45.6% |
| Macrocystic LM | 17 | 36.9% |
| Microcystic LM | 8 | 17.4% |
| Partial PFNP | 13 | 28.2% |
| Total PFNP | 4 | 8.7% |
| Diaphragm paralysis | 9 | 19.5% |
| Spinal nerve injury | 7 | 15.2% |
| Breast hypoplasia | 6 | 13 |
| RLN paralysis | 5 | 10.8%6 |
| Hypoglossal nerve injury | 2 | 4.3% |
LM, lymphatic malformation; PFNP, peripheral facial nerve palsy; RLN, recurrent laryngeal nerve.
Most LMs are caused by changes in the PIK3CA gene and tend to be localised in the cervicofacial region.4 For years, surgery was the mainstay of LM treatment, but due to the high frequency of complications, of up to 33%, especially neurologic ones (4%–7%), and of residual disease after surgery, of 53%, at present sclerotherapy, rapamycin and alpelisib are used as more effective and safer treatment options.5 Surgery is reserved for cases that require resolution within a short timeframe, such as those causing airway obstruction and other particular situations. When urgent debulking is not required, conservative stepwise treatment has proven to be the best approach to reduce morbidity and mortality.6 The choice of treatment is based on the age of the patient, the location of the malformation, the severity of the symptoms, the size and type of LM and the treatment goals established in shared decision-making. No treatment option is superior to the others, as they are complementary and each particular case will require a specific approach or a combination thereof. In short, the complications observed in this case series are similar to those described in the previous literature and remind us that LMs are a benign, non-malignant diseases that require multidisciplinary management with the primary goal of preserving functional integrity and the secondary goal of maintaining harmony in physical features. With this in mind, we propose 10 key recommendations for the management of LMs:
- 1
Lymphatic malformations do not proliferate, they are malformations and not tumours
- 2
The concept of recurrence does not apply, they expand due to the accumulation of lymphatic fluid if there is residual disease.
- 3
Evaluation of the lymphatic system by means of magnetic resonance lymphangiography is recommended to rule out lymphatic conduction disorders (such as central conducting lymphatic anomaly).
- 4
Genetic testing should be performed if possible, as there are causative genetic variants (KRAS, PIK3CA genes) for which targeted therapy is available.
- 5
There are multiple treatment options: sclerotherapy, pharmacotherapy and surgery. We recommend a stepwise approach in that very order whenever possible.
- 6
If surgery is indicated, a radical approach should be avoided due to the risk of complications.
- 7
After surgery, residual lesions can be managed with sclerotherapy and pharmacotherapy
- 8
Recent advances in the knowledge of pathogenic pathways have allowed the use of novel drugs such as alpelisib.
- 9
Multidisciplinary treatment is associated with improved outcomes
- 10
The establishment of vascular anomaly care teams improves outcomes and facilitates decision-making.
This research did not receive any external funding.
Conflicts of interestThe authors have no conflicts of interest to declare.
Informed consentAll patients and/or their legal guardians provided their consent, verbally and in writing, to the publication of photographs and clinical information.
