


Basic life support training in school age is a topical issue because, with adequate training, any person can help save a life.
MethodsCluster clinical trial with data collection through an ad hoc self-administered, semi-structured questionnaire. The target population encompassed the students aged 4–6 years enrolled in 49 educational centres. The centres were randomly allocated to the intervention or control group. The intervention group was trained with the RCParvulari® methodology, consisting of theoretical and practical training on the first link of the chain of survival. The control group only received theoretical training. We evaluated participants before and immediately after the intervention and between 3 and 12 months post intervention by means of the questionnaire. We assessed the acquisition and retention over time of the knowledge and skills covered in the training compared to previous trainings in both groups.
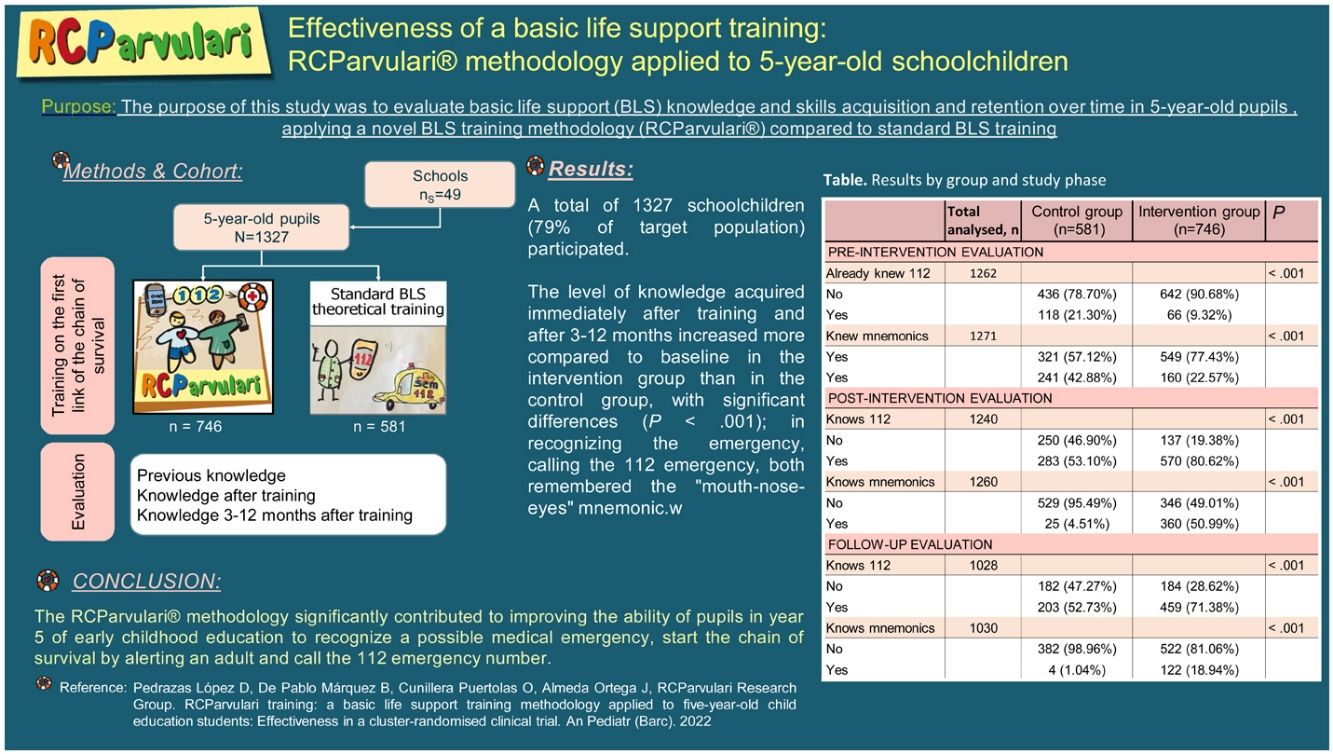
ResultsA total of 1327 schoolchildren (79% of the target population) participated. The level of knowledge acquired immediately after training and after 3–12 months compared to baseline was significantly better (P < .001) in the intervention group than in the control group, both in early recognition and contacting of emergency services (112) and in remembering the “mouth-nose-eyes” mnemonic.
ConclusionsThe RCParvulari® methodology significantly contributed to an improved ability to recognize a possible medical emergency, start the chain of survival by alerting an adult and call the 112 emergency number in students in the last year of preschool education.
La formación en soporte vital básico en edad escolar es un tema de actualidad, ya que, con una formación adecuada, todo individuo puede ayudar a salvar una vida.
MétodosEnsayo clínico por conglomerados basado en un cuestionario ad hoc, autoadministrable y semiestructurado. La población diana fueron alumnos de entre 4 y 6 años de 49 centros educativos. Los centros se aleatorizaron en grupo intervención y control. El grupo intervención recibió la metodología RCParvulari®, consistente en una formación teórico-práctica sobre el primer anillo de la cadena de supervivencia. El grupo control solo recibió una formación teórica. Los sujetos de estudio fueron evaluados pre-intervención, post-intervención y entre 3 y 12 después mediante un cuestionario. Se valoró adquisición y retención a lo largo del tiempo de la información recibida, en comparación con la formación previa en ambos grupos.
ResultadosParticiparon un total de 1327 escolares (79% de la población diana). El nivel de conocimientos adquiridos inmediatamente después de la formación y pasados 3–12 meses aumentó más respecto al basal en el grupo intervención que en el grupo control con diferencias significativas (P < ,001), tanto al reconocer y llamar al número de emergencias 112, como al recordar la mnemotecnia “boca-nariz-ojos”.
ConclusionesLa metodología RCParvulari® contribuyó de forma significativa a mejorar la capacidad del alumnado de 5° curso de educación infantil para reconocer una eventual emergencia médica, poner en marcha la cadena de la supervivencia alertando a un adulto y llamando al número de emergencias 112.
Out-of-hospital cardiac arrest (OHCA) is the third-leading cause of death in developed countries1 and it is witnessed by relatives, friends or other bystanders in up to 70% of cases.2 Early cardiopulmonary resuscitation is a determining factor for survival and neurological otucomes.3 The basic cornerstone of responding to OHCA is training in basic life support (BLS) and, in this regard, training schoolchildren is one of the most effective strategies.4,5
The chain of survival (CS) was proposed by the American Heart Association (AHA) in 1991 and has been evolving to this day with the collaboration of the AHA and the European Resuscitation Council (ERC).1,2 It consists of a series of actions aimed at saving the lives of victims of cardiac arrest. These actions range from early recognition and activation of emergency services (the first link of the chain of survival) to delivery of adequate cardiopulmonary resuscitation and early use of the defibrillator.
Despite the fact that the Kids Save Lives statement3 issued by the ERC and endorsed by the World Health Organization recommends teaching cardiopulmonary resuscitation (CPR) to schoolchildren for 2 h per year from age 12,4 there is evidence that shows that the chain of survival sequence can be learned from age 6 years.5 In general, BLS training programs are not included in the early childhood education or primary education curricula in Spain.1,6–8
Although randomized controlled trials have investigated the effect of a BLS workshop in primary school9 and medical school,10 there is less evidence for children aged 5–8 years. Several studies suggest that schoolchildren aged 5–8 years retain what they have learned well, and evaluation results are not inferior to those in older children or adults.1,8 Some studies have even shown that children aged 5–8 years are able to understand the chain of survival and how to activate it,1,11–13 although the impact of BLS training at these ages has not been evaluated. In fact, to date, there is no validated questionnaire developed to assess knowledge on BLS in young children.
The purpose of our study was to assess the acquisition and retention over time of BLS knowledge and skills (mainly the first link in the chain of survival) in schoolchildren in the last year of preschool education trained with a novel CPR education methodology (RCParvulari®) compared to standard BLS training.14
MethodsStudy designWe conducted a cluster randomised controlled clinical trial.
Study populationThe target population comprised the 1680 students of year P-5 (last year of preschool education, with an age range of 4–6 years) enrolled in the 49 early childhood and primary education schools based on the municipal population census of 2016.15
Schools whose administrators agreed to participate in the study were randomly assigned to the intervention or control group (cluster randomization with a random number table).
The inclusion criteria were current enrolment in the participating early childhood and primary education schools during the study period and signed informed consent to the child’s participation from the parents or legal guardians.
InterventionThe intervention group (IG) was trained with the RCParvulari® methodology, in which knowledge and skills related to the first link of the chain of survival are taught with different modalities (drawings, photographs, songs, role play activities with giant mobile phone models) with brief, changing, participatory and repetitive activities (Fig. 1), with an overall duration of approximately 45 min. This intervention has been described in a previous article.14
 and role play games (right) in the RCParvulari® training method.")
The control group (CG) received only theoretical training on the concepts and skills in the first link of the chain of survival. The training was structued around a PowerPoint® presentation that included theoretical concepts, algorithms and images that explained that in the event of an emergency, one had to call the emergency number 112, and the mnemonic: mouth-nose-eyes. The training lasted approximately 30 min.
Study variablesTo assess the variables under study, we developed an ad hoc self-administered and semi-structured questionnaire. The questionnaire was drafted and underwent validity assessment and a pilot test in 5 students in the age range of interest to ensure that the test was appropriate for that age group.14
All participants, whether they were in the IG or CG, completed the same questionnaire in the classroom at 3 time points: preintervention (just before the training), post-intervention (immediately after the training) and follow-up (3–12 months after the training). Fig. 2 presents a flow chart with the distribution into groups and the phases of the study.

The variables under study were:
- •
Dependent variables: learning (or lack thereof) and understanding the first link in the chain of survival, recognising (or not) emergency number 112 and associating it (or not) with the mouth-nose-eyes mnemonic.14
- •
Independent variables: age, sex, previous BLS training and “gossip effect”.
Gossip effect: when the questionnaire was administered, some children copied from the person sitting next to them. This event was supervised and recorded by both teachers during the time that students were filling out the questionnaire.
Sample sizeWe calculated that it would take 453 in the intervention group and 453 individuals in the control group to detect a difference greater or less than 10% in the proportion of correct answers expected in the control group (0.5, with a minimum relative risk of 1.2) with an alpha risk of 0.05 and a beta risk of 0.2. We assumed an attrition of 10% using a Poisson approximation.
Cluster randomization produced a larger sample than required, ensuring a design effect of 2. In other words, the final number of participants per group was 906, adding to a total sample of 1816.
We performed the calculations with the GRANMO® sample size calculator, version 7.12 (April 2012).
Statistical analysisWe performed comparative, univariate and bivariate analyses of preintervention data in the intervention and control groups. We also conducted a bivariate analysis of outcome variables based on the group. Quantitative variables were expressed as mean and standard deviation (SD) or median and interquartile range, and qualitative variables as absolute and relative frequencies. To compare groups, we used the Mann-Whitney U test and the Student t-test were used for quantitative variables and the χ2 test for qualitative variables. We defined statistical significance as a two-tailed P value of less than .05. We fitted 4 multivariate logistic regression models for each of the outcome measures at the different time points; in these models, knowledge was the dependent variable to be explained based on the intervention group, sex, age, previous training, previous knowledge of the 112 number and the mnemonic rule (separately) and the baseline and follow-up ‘gossip’ effects. The models were developed through backward stepwise regression, starting with the saturated model and removing variables until only those that explained the variance in the outcome were left, applying the Akaike information criterion.
The analyses were performed with the statistical software R, version 4.0.5.
Ethical considerationsThe study protocol was approved by the competent ethics committee.
The clinical trial was registered in ClinicalTrials.gov with identifier NCT03443167.
We obtained signed informed consent for participation and for dissemination of study images from the parents or legal guardians of all participants.
Once the study was completed, the RCParvulari® training was offered to all schools that participated in the control group and provided to those that requested it.
ResultsForty-one early childhood and primary education schools in Baix Llobregat agreed to participate in the study, with a cumulative student body of 1327 P-5 students; 20 schools were assigned to the IG and 21 to the CG (Fig. 2). The resulting sample included 1327 schoolchildren (79% participation rate: 746 participants in IG and 581 in CG). Of this total, 75.2% were 5 years old, and 51% (n = 648) were female.
In the preintervention evaluation, 14.6% of the sample already knew the 112 emergency number, and 10 children (0.8%) reported knowing the mouth-nose-eyes mnemonic. In the control group, a much higher proportion knew the 112 number (21.3% compared to 9.3% in IG; P < .001). In the total sample 31.6% of children had received previous training on BLS from the local/regional police or fire department: 241 in the control group and 160 in the intervention group (42.9% of CG vs 22.6% of IG; P < .001) (Table 1).
Summary of results by group and study phase.
| Children in analysis, n | Missing | Total | Control group (n = 581) | Intervention group (n = 746) | P | |
|---|---|---|---|---|---|---|
| PRE-INTERVENTION EVALUATION | ||||||
| Knew 112 | 1262 | 65 | <.001 | |||
| No | 1078 (85.4%) | 436 (78.7%) | 642 (90.7%) | |||
| Yes | 184 (14.6%) | 118 (21.3%) | 66 (9.3%) | |||
| Knew mnemonic | 1261 | 66 | .946 | |||
| No | 1251 (99.2%) | 549 (99.1%) | 702 (99.3%) | |||
| Yes | 10 (0.8%) | 5 (0.9%) | 5 (0.7%) | |||
| Previous training | 1271 | 56 | <.001 | |||
| No | 870 (68.5%) | 321 (57.1%) | 549 (77.4%) | |||
| Yes | 401 (31.5%) | 241 (42.9%) | 160 (22.6%) | |||
| Gossip effect | 1260 | 67 | <.001 | |||
| No | 1069 (84.8%) | 407 (73.6%) | 662 (93.6%) | |||
| Yes | 191 (15.2%) | 146 (26.4%) | 45 (6.4%) | |||
| POST-INTERVENTION EVALUATION | ||||||
| Knew 112 | 1240 | 87 | <.001 | |||
| No | 387 (31.2%) | 250 (46.9%) | 137 (19.4%) | |||
| Yes | 853 (68.8%) | 283 (53.1%) | 570 (80.6%) | |||
| Knew mnemonic | 1260 | 67 | <.001 | |||
| No | 875 (69.4%) | 529 (95.5%) | 346 (49%) | |||
| Yes | 385 (30.6%) | 25 (4.5%) | 360 (51%) | |||
| Gossip effect | 1267 | 60 | <.001 | |||
| No | 954 (75.3%) | 256 (46.2%) | 698 (97.9%) | |||
| Yes | 313 (24.7%) | 298 (53.8%) | 15 (2.1%) | |||
| FOLLOW-UP EVALUATION | ||||||
| Knew 112 | 1028 | 299 | <.001 | |||
| No | 366 (35.6%) | 182 (47.3%) | 184 (28.6%) | |||
| Yes | 662 (64.4%) | 203 (52.7%) | 459 (71.4%) | |||
| Knew mnemonic | 1030 | 297 | <.001 | |||
| No | 904 (87.8%) | 382 (98.9%) | 522 (81.1%) | |||
| Yes | 126 (12.2%) | 4 (1.1%) | 122 (18.9%) | |||
| Gossip effect | 1034 | 293 | .056 | |||
| No | 1028 (99.4%) | 382 (98.7%) | 646 (99.8%) | |||
| Yes | 6 (0.6%) | 5 (1.3%) | 1 (0.2%) | |||
| Time of follow-up interview | 1012 | 315 | <.001 | |||
| <4 months | 520 (51.4%) | 223 (58.5%) | 297 (47.1%) | |||
| 4–7 months | 208 (20.5%) | 57 (15%) | 151 (23.9%) | |||
| 8–12 months | 120 (11.9%) | 25 (6.6%) | 95 (15.2%) | |||
| >1 year | 164 (16.2%) | 76 (19.9%) | 88 (13.9%) | |||
In the post-intervention evaluation, both groups exhibited significant changes in the knowledge of the 112 number and the mnemonic, with greater improvement in the IG (P < .001) (Table 1), differences that were sustained in the follow-up evaluations at 3–12 months, where 71.4% still remembered the 112 number and 19.0% the mnemonic rule in the intervention group, compared to 52.7% and 1.0%, respectively, in the control group (P < .001) (Table 1).
In the original study design, the follow-up evaluation had to be carried out 6 months after the intervention.14 In some schools, the follow-up evaluation was delayed to up to 1 year post intervention due to organizational challenges. In spite of this, the results showed that students in the intervention group remembered the 112 number and the mnemonic not only for a few months, but even after 1 year.
The results of the multivariate regression models showed that the intervention had a statistically significant effect on knowledge of the 112 number and the mnemonic rule immediately after the training and in the follow-up (P < .001) (Tables 2 and 3), with a more than 20-fold increase in the odds of knowing the 112 number and the mnemonic rule, with the exception of knowing the 112 number in the follow-up (the odds ratio of knowing the 112 number in the follow-up in the intervention group was 3.22).
Variables associated with post-intervention results. Multivariate logistic regression models on 2 separate outcome measures: knowing the 112 number and remembering the mnemonic. Results for the full model are presented first, followed by results for the model obtained through backward stepwise regression using the Akaike information criterion.
| 112 | Mnemonic | |||||||
|---|---|---|---|---|---|---|---|---|
| Full model | Maximum likelihood model | Full model | Maximum likelihood model | |||||
| OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P | |
| Independent term | 0.05 (0.01−0.4) | .004 | 0.10 (0.06−0.15) | <.001 | 0.01 (0.00−0.05) | <.001 | 0.01 (0.00, 0.06) | <.001 |
| Intervention Group | 38 (24.3−62) | <.001 | 37.5 (24−61) | <.001 | 28.2 (16.2−52.9) | <.001 | 22.2 (14.5−35.4) | <.001 |
| Male sex | 1.1 (0.8−1.6) | .418 | 1.3 (1−1.7) | .065 | 1.3 (1−1.7) | .065 | ||
| Age | 1.1 (0.8−1.6) | .583 | 1.3 (0.9−1.8) | .139 | 1.3 (0.9−1.8) | .126 | ||
| Previous training | 1 (0.7−1.5) | .838 | 1 (0.7−1,5) | .809 | ||||
| Baseline gossip effect | 0.7 (0.4−1.3) | .223 | 0.5 (0.2−0.9) | .028 | 0.5 (0.3−1) | .043 | ||
| Knew 112 previously | 3.4 (1.8−6.6) | <.001 | 2.8 (1.6−5.1) | <.001 | 2 (1.1−3.5) | .012 | 2 (1.2−3.5) | .011 |
| Knew mnemonic previously | 0.6 (0.1−3.3) | .504 | 4.4 (0.9−22.8) | .074 | 4.6 (0.9−23.6) | .064 | ||
| Post-intervention gossip effect | 65.8 (36.9−122.3) | <.001 | 59.9 (34.9−107.2) | <.001 | 1.6 (.8−3.1) | .188 | ||
CI, confidence interval; OR, odds ratio.
Variables associated with the results in the follow-up. Multivariate logistic regression models on two separate outcome measures: knowing 112 and remembering the mnemonic. The model adjusted for all the variables is presented first and then the model resulting from the “stepwise backwards” variable selection process based on “Akaike Information Criteria”.
| 112 | Mnemonic | |||||||
|---|---|---|---|---|---|---|---|---|
| Full model | Maximum likelihood model | Full model | Maximum likelihood model | |||||
| OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P | |
| Independent term | 0.1 (0.01−0.5) | .006 | 0.1 (0.01−0.4) | .005 | 0.01 (0.00, 0.08) | <.001 | 0.01 (0.00−0.01) | <.001 |
| Intervention group | 3.2 (2.4−4.4) | <.001 | 3.2 (2.4−4.4) | <.001 | 24.6 (10−81.9) | <.001 | 24 (9.9−79.3) | <.001 |
| Male sex | 0.9 (0.7−1.1) | .329 | 0.9 (0.6−1.3) | .616 | ||||
| Age | 1.3 (0.9−1.9) | .116 | 1.3 (0.9−1.9) | .117 | 1.0 (0.6−1.6) | .985 | ||
| Previous training | 1.4 (1−2.2) | .067 | 1.4 (1−2.1) | .072 | 1.3 (0.8−2.3) | .315 | ||
| Baseline gossip effect | 2.6 (1.3−5.3) | .008 | 2.3 (1.4−4) | .001 | 1 (0.4−2.3) | .923 | ||
| Knew 112 previously | 0.9 (0.5−1.6) | .693 | 2 (1−3.7) | .034 | 2.1 (1.2−3.7) | .008 | ||
| Knew mnemonic previously | 0.9 (0.04−24.5) | .969 | 0.0 (0.00, Inf) | .991 | ||||
| Interview period (ref. 6 months) | ||||||||
| <4 months | 3.8 (2.6−5.5) | <.001 | 3.7 (2.5−5.4) | <.001 | 1.4 (0.8−2.7) | .234 | 1.6 (0.9−2.9) | .114 |
| 4−7 months | (ref.) | – | (ref.) | – | (ref.) | – | (ref.) | – |
| 8−12 months | 2.8 (1.7−4.7) | <.001 | 2.8 (1.7−4.6) | <.001 | 3.5 (1.8−7) | <.001 | 3.4 (1.8−6.7) | <.001 |
| >1 year | 2.3 (1.4−3.8) | .001 | 2.22 (1.4−3.7) | .002 | 1.5 (0.7−3.1) | .323 | 1.6 (0.7−3.2) | .229 |
| Post-intervention gossip effect | Inf (0.00, Inf) | .968 | Inf (0.00, Inf) | .968 | 0.00 (0.0−85) | .982 | ||
CI, confidence interval; OR, odds ratio.
Other variables, such as prior knowledge and the gossip effect, were also significantly associated with acquired knowledge in the multivariate models, depending on the outcome measure and the timing of the evaluation.
DiscussionThe RCParvulari® method is a novel training approach aimed at children in the last year of preschool to make them able to activate the chain of survival in the event of a medical emergency. This is achieved by adapting existing tools to the age of the students to facilitate their learning: a Power Point® presentation, a screening of drawings, cartoons, photographs, a song and role play with giant mobile phone models (Fig. 1).14
The results showed that a training lasting 30−50 min, with an eminently practical and participatory approach, significantly improved knowledge and practices related to the first link of the chain of survival in children in the last year of preschool education.
To our knowledge, there have been no previous studies in the preschool setting that made a quantitative assessment of the learning capacity for BLS (theoretical and practical) of children aged 4–6 years.
There have been previous works, such as the study by Martinez-Isasi et al.,16 which showed that, after a period of training implemented during school hours, students in years 3 and 5 of primary education and year 1 of compulsory secondary education (aged 8–12 years) were able to activate the chain of survival and initiate CPR. Similar to what we did in our study, other authors, such as Otero-Agra et al.,1 have applied their own training methodology, validating the content and suitability of the material used in the process, to train older schoolchildren on the chain of survival.
All these works show that BLS training in the school setting improves knowledge on the subject in the different age groups targeted in the research. This type of training can have a great impact on public health, as individuals of any age can save lives if they receive proper training.3 In addition, early childhood education students are open to be trained on BLS and can serve as CPR multipliers by teaching their friends and families.16
Thus, in the long-term, BLS training strategies can increase survival rates and quality of life in victims of cardiac arrest.18 Currently, in Europe, the highest bystander CPR rates are found in Scandinavian countries where education of schoolchildren in CPR has been mandatory for decades.3
Basic life support training in early childhood is a strategy that can help reduce the mortality associated to out-of-hospital cardiac arrest. Schools are the ideal setting to teach BLS if the objective is to train the entire population, as it would ensure that nearly 100% of the population in developed countries would receive the training.18,19
Educating and training children in CPR also brings social benefits, since they learn to help other people. Students and teachers are also important multipliers and can increase the proportion of individuals trained in CPR in the long term.3,17
One finding of this study concerned the variable adapted from the previous literature that we referred to as the “gossip effect”. The students answered the questionnaire in their usual environment, seated in their chairs at their desk in the classroom. We noticed that at the time of completing the questionnaire before the intervention, children who did not know how to answer copied from peers who did. This exchange of information is another way of learning, as they no longer copied answers when completing the questionnaire immediately after the intervention or in the follow-up.
There are studies, such as the one by Seki et al.,20 that, although carried out in a different setting and in adults, describe “gossip” as a way of promoting cooperation, altruism and knowledge retention.
LimitationsOne of the strengths of our study, the creation and evaluation of a method for BLS training in an age group in which no research had been conducted to date, is also one of its limitations: the RCParvulari® methodology has been created and tested in children in the last year of preschool education, so we do not know whether it would be valid for other age groups. We also could not assess whether training at an early age would facilitate the consolidation of knowledge about BLS at later ages, or whether acquisition of this knowledge in this age group would improve long-term survival in victims of OHCA.
Another possible limitation of the study is the significant differences we found in prior knowledge and training between the intervention and control groups. Although the results support the conclusions, they could not be fully explained in randomised groups. It is possible that this would not have been an issue if the initial groups had more homogeneous characteristics, but the study design was based on the principle of randomization.
ConclusionTheoretical/practical training using an age-appropriate methodology helps students in the last year of early childhood education learn and retain knowledge about the first link in the chain of survival. The results of our study show that basic life support training could be started in early childhood with good results.
Conflict of interestThe authors declare that they have no conflict of interest.
We thank all the children enrolled in year 5 of early childhood education in early childhood and primary education schools in Baix Llobregat Nord for their daily work and for selfless participation in the project. We also thank the parents of all participating students for believing and trusting in the project.
Our appreciation also extends to the administrative staff at participating schools for the logistical support provided during the months of fieldwork.
Lastly, we thank the staff of the Costa de Ponent Primary Care Administration for the translation and the staff of the Institut Universitari d’Investigació en Atenció Primària Jordi Gol IDIAP for their support. Also, Sara Torres for the photographs that she took disinterestedly for the project materials, and Edu Pérez for designing the logos and posters created specifically for the RCParvulari ® project.
Grupo de Investigación RCParvulari: Campíñez Navarro, Manuel (Orewa, Nueva Zelanda), del Castillo Giraldez, Ana (Sant Vicenç dels Horts, España), Díaz Carrasco, Francesc Xavier (Abrera, España), Espinach García, Nèstor (Badalona, España), Fernández Carod, Noèlia (Sant Joan Despí, España), García Font, David (Abrera, España), Flores Carrillo, Anna (Esparreguera, España), Roda Diestro, Jovita (Sant Andreu de la Barca, España), Vergès Macario, Isabel (Abrera, España).
