
Neurofibromatosis type 1 (NF1) is a genetic disorder with various clinical manifestations that affect the peripheral and central nervous system, as well as the skin, bones and endocrine and vascular system. There is still insufficient knowledge of neuropsychological effects of NF1 on children, and there is some controversy about the cognitive deficits that defines the cognitive profile of patients affected by this disorder.
AimsIn this study an analysis is made of the neuropsychological performance of a group of patients affected by NF1, compared with a control group of healthy children.
Subjects and methodA comparison was made between the neuropsychological performance of a group of 23 boys and girls with a mean age of 8.7 years (+/−1.39) and diagnosed with NF1, and a control group consisting of 21 healthy children, with mean age of 8.9 years (+/−1.41) and with similar socio-demographic characteristics. The Wechsler Intelligence Scale for Children (WISC) was applied to evaluate the subjects of both groups.
ResultsThe group of patients affected with NF1 showed a lower performance in every primary index of WISC IV: Verbal Comprehension Index, Fluid Reasoning Index, Working Memory Index, Processing Speed Index, and full scale IQ. Only in two subscales were no statistically significant differences observed: similarities and coding.
ConclusionThe results show subtle and generalised neuropsychological alterations in the sample of children affected with NF1, which affect most of cognitive domains that have been evaluated. Proper specific and early neuropsychological treatment should be provided in order to prevent the high risk for these children of presenting learning difficulties and school failure.
La neurofibromatosis tipo 1 (NF1) es un trastorno genético con manifestaciones clínicas muy variables que pueden expresarse en el sistema nervioso central y periférico, así como en piel, hueso, sistema endocrinológico y vascular. Los aspectos neuropsicológicos de la NF1 en la infancia continúan sin ser suficientemente conocidos, existiendo controversia acerca de los posibles déficits que definen el perfil cognitivo de estos niños.
ObjetivoEstudiar el rendimiento neuropsicológico de un grupo de pacientes con NF1 en comparación con un grupo de control de niños sanos.
Sujetos y métodoSe estudia el rendimiento neuropsicológico de un grupo de 23 niños y niñas con diagnóstico de NF1, con una edad media de 8,7 años ± 1,39 comparado con otro grupo formado por 21 niños sanos con una edad media de 8,9 años ± 1,41 con características sociodemográficas similares. A todos los sujetos se les aplicó la Escala de Inteligencia de Wechsler infantil (WISC-IV).
ResultadosSe observa en el grupo con NF1 un rendimiento menor que el grupo control en los índices globales del WISC-IV: comprensión verbal, razonamiento perceptivo, memoria de trabajo, velocidad de procesamiento y cociente intelectual global. Únicamente en los subtest de claves y semejanzas no se han apreciado diferencias estadísticamente significativas entre ambos grupos.
ConclusiónLos resultados reflejan la existencia de alteraciones neurocognitivas sutiles y generalizadas en la muestra de niños con NF1, que afectan a la mayoría de los dominios cognitivos evaluados. Se subraya la necesidad de que reciban una atención neuropsicológica específica precoz para prevenir el mayor riesgo de presentar dificultades de aprendizaje y fracaso escolar.
Neurofibromatosis (NF) is a hereditary autosomal dominant disease with a variable expression, although half of the cases result from de novo mutations. It affects the tissues that support the central and peripheral nervous systems. It is a neurocutaneous disorder that causes changes in skin pigmentation (“café au lait” macules), the cranial nerves and the spinal cord. It can also manifest with additional features, such as neurofibromas (cutaneous, subcutaneous or intraspinal tumours), pain in affected nerves, epileptic seizures, blindness or deafness secondary to gliomas in the optic or vesticulocochlear nerves, or hydrocephalus due to aqueductal stenosis.
There are two distinct forms of NF based on clinical, genetic and pathophysiological features, both of which belong to the broader category of neurocutaneous syndromes or phakomatoses. One is the peripheral form, known as NF type 1 (NF1), formerly von Recklinghausen disease. The other is the central form, also known as NF type 2 (NF2).1 Like NF1, it is a hereditary autosomal dominant disease, which in this case is caused by a gene located in chromosome 22q21.
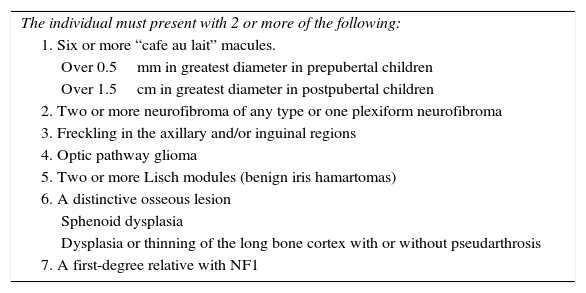
The incidence of NF1 is of 1 per 3000–4000 individuals. The disease is caused by mutations in the NF1 gene located in chromosome 17q11.2. Approximately half of the cases are de novo mutations.2 The clinical diagnosis of NF1 requires the presence of at least 2 of the criteria established at the National Institute of Health Consensus Development Conference3 held in 1988 (Table 1).
Diagnostic criteria for neurofibromatosis type 1.
| The individual must present with 2 or more of the following: |
| 1. Six or more “cafe au lait” macules. |
| Over 0.5mm in greatest diameter in prepubertal children |
| Over 1.5cm in greatest diameter in postpubertal children |
| 2. Two or more neurofibroma of any type or one plexiform neurofibroma |
| 3. Freckling in the axillary and/or inguinal regions |
| 4. Optic pathway glioma |
| 5. Two or more Lisch modules (benign iris hamartomas) |
| 6. A distinctive osseous lesion |
| Sphenoid dysplasia |
| Dysplasia or thinning of the long bone cortex with or without pseudarthrosis |
| 7. A first-degree relative with NF1 |
Source: National Health Institute.3
Neurofibromatosis type 1 can affect early developmental processes, increasing the risk of learning difficulties in childhood. Approximately 80% of children with NF1 have cognitive comorbidities, with marked impairment in one or more cognitive functions, which has a negative impact on academic achievement and quality of life. In the past, these children received diagnoses of mental retardation, but more recent studies have confirmed that only 4%–8% of individuals with NF1 have an intellectual quotient (IQ) of less than 70. A study by Hyman et al.4 tested the IQ of 81 children with NF1 and compared it to the IQ of their siblings. Sixty-one percent of children with NF1 had IQ scores that were at least 10 points lower than their siblings. The study concluded that in more than 70% of children with NF1, academic performance is inferior to what would be expected based on their intellectual ability.
Individuals with NF1 usually have neuropsychological deficits in various cognitive domains: executive function, visual perception, memory etc. However, there is no widespread agreement on the definition of the cognitive profile of NF1, as 2 different criteria are currently in use. Some authors believe that the differential factors that distinguish NF1 are deficits in visual-spatial skills and problems in attention and executive functioning.5 Others emphasise the usual presence of language deficits combined with problems in visual-spatial skills, attention and executive functioning. There is evidence in the literature that due to the associated neuropsychological changes, between 30% and 65% of children with NF1 have learning difficulties in school in the areas of reading, writing, spelling, mathematics and language.6,7
The aim of our study was to assess the global intellectual ability of children with NF1 and their performance in different cognitive domains assessed by means of the Wechsler Intelligence Scale for Children (WISC-IV).
Participants and methodsSampleExperimental group with neurofibromatosis type 1 (NF1G)This group comprehended 23 children (8 boys and 15 girls) with a NF1 diagnosis. The mean age was 8.7±1.39 years. We selected the participants from the patients that received care at the Department of Paediatric Neurology of the Hospital Universitario La Paz in Madrid. The inclusion criteria for the NF1G were: confirmed diagnosis of NF1; age 6–10 years; absence of sensory, neurologic or psychiatric comorbidities; not being under psychopharmacological treatment at the time of assessment.
Control groupIt consisted of 21 healthy children (8 boys and 13 girls). The mean age was 8.9±1.41 years. We selected these children from two schools in the northern area of the city of Madrid. The inclusion criteria were: age 6–10 years; sociodemographic characteristics similar to those of patients in the NF1 group; absence of sensory, neurologic or psychiatric disorders; and not being under psychopharmacological treatment at the time of assessment.
Tests performedWe administered the full version of the Spanish adaptation of the WISC-IV8 to each participant in the study separately. This scale allows the evaluation of overall IQ as well as performance in different cognitive domains: verbal comprehension, perceptual reasoning, working memory and processing speed.
ProtocolParticipants in the NF1G were assessed in the facilities of the Department of Paediatric Neurology of the Hospital Universitario La Paz of Madrid in the course of previously scheduled appointments. The study had been approved by the Clinical Research Ethics Committee of the Hospital Universitario La Paz. The CG was assessed in the school counselling department offices of 2 schools located in northern Madrid (Colegio Nuestra Señora del Buen Consejo and Colegio Internacional Pinosierra); all assessments were performed in individual morning sessions. The Department of Biostatistics of the Instituto de Investigación (Research Institute) of the Hospital Universitario La Paz (IdiPAZ) performed the statistical analysis. Data were processed in a Microsoft Excel database that was subsequently exported for statistical analysis with the SPSS software version 11.5.
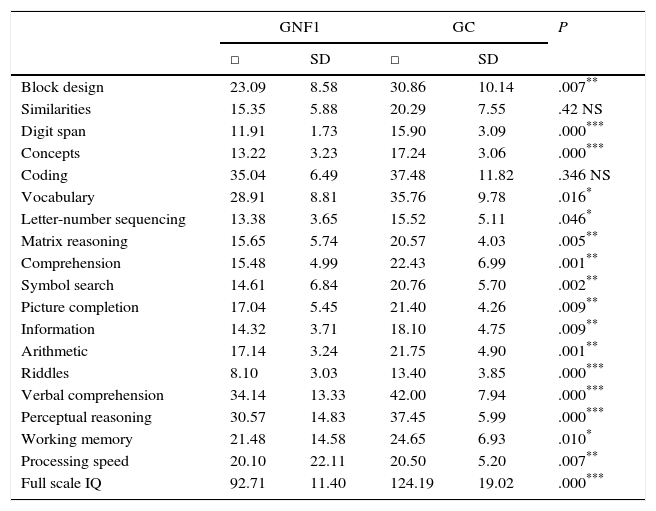
ResultsCognitive performance in children with NF1 was inferior to that of children in the CG for the 5 composite indices of the WISC-IV: verbal comprehension, perceptual reasoning, working memory, processing speed and the full scale IQ. The NF1G scored lower than the CG in every WISC-IV subtest save for the coding and similarities subtests, in which we observed no significant differences between groups. Table 2 summarises the results.
Scores in the Wechsler Intelligence Scale for Children (WISC-IV).
| GNF1 | GC | P | |||
|---|---|---|---|---|---|
| □ | SD | □ | SD | ||
| Block design | 23.09 | 8.58 | 30.86 | 10.14 | .007** |
| Similarities | 15.35 | 5.88 | 20.29 | 7.55 | .42 NS |
| Digit span | 11.91 | 1.73 | 15.90 | 3.09 | .000*** |
| Concepts | 13.22 | 3.23 | 17.24 | 3.06 | .000*** |
| Coding | 35.04 | 6.49 | 37.48 | 11.82 | .346 NS |
| Vocabulary | 28.91 | 8.81 | 35.76 | 9.78 | .016* |
| Letter-number sequencing | 13.38 | 3.65 | 15.52 | 5.11 | .046* |
| Matrix reasoning | 15.65 | 5.74 | 20.57 | 4.03 | .005** |
| Comprehension | 15.48 | 4.99 | 22.43 | 6.99 | .001** |
| Symbol search | 14.61 | 6.84 | 20.76 | 5.70 | .002** |
| Picture completion | 17.04 | 5.45 | 21.40 | 4.26 | .009** |
| Information | 14.32 | 3.71 | 18.10 | 4.75 | .009** |
| Arithmetic | 17.14 | 3.24 | 21.75 | 4.90 | .001** |
| Riddles | 8.10 | 3.03 | 13.40 | 3.85 | .000*** |
| Verbal comprehension | 34.14 | 13.33 | 42.00 | 7.94 | .000*** |
| Perceptual reasoning | 30.57 | 14.83 | 37.45 | 5.99 | .000*** |
| Working memory | 21.48 | 14.58 | 24.65 | 6.93 | .010* |
| Processing speed | 20.10 | 22.11 | 20.50 | 5.20 | .007** |
| Full scale IQ | 92.71 | 11.40 | 124.19 | 19.02 | .000*** |
NS: difference is not significant.
In this study, we analysed the cognitive performance of a group of children with NF1 compared to another group of healthy children of similar socioeconomic characteristics. We observed significant differences in all composite indices and in 12 of the 14 subtests of the WISC-IV, with children with NF1 obtaining lower scores than children in the CG.
The IQ of the NF1G was below the normal psychometric threshold, and was significantly lower than the IQ of the CG, with a difference of 31 points. But obtaining an IQ score within the normal range does not suffice to determine that cognitive performance is at a comparable level. Intellectual ability and cognitive performance are not always equivalent, as there may be weak areas in the individual's cognitive profile that hinder performance. On the other hand, there is widespread agreement that in addition to intelligence understood as a global parameter, there are different specific intellectual abilities that develop to different degrees, which is referred to as multiple intelligences.9,10
The first publications on the cognitive ability of children with NF1 described levels of cognitive impairment that were significantly greater than those found in recent studies. Thus, Mulvihill reported an average IQ of 45 for a sample of 20 patients with NF1.11 Studies conducted more recently have not corroborated those differences, but placed the IQ of children with NF1 closer to the normal range. For instance, one study found that only 6% of children with NF1 had IQ scores significantly below average.12
In our study, the performance of children with NF1 was inferior to that of the CG for every cognitive domain assessed by the WISC-IV, with the exception of the coding and similarities subtests. These results are not exactly consistent with those of other studies; Cutting and Levine assert that the cognitive profile of NF1 fits the pattern of a “nonverbal” disorder, as most individuals with NF1 exhibit visual-perceptual abnormalities (specifically in visual-spatial skills).13 However, difficulties in verbal language, learning, reading and writing are also frequent in NF1.14 In our study, we found both verbal and nonverbal impairments that had a generalised impact on cognitive performance in children with a NF1 diagnosis.
Other cognitive domains, such as executive functioning, which encompasses the performance of more complex reasoning processes and the organisation of goal-directed behaviour, are also usually affected in children with NF1. The results of our study are consistent with those of other authors, who also found difficulties in reasoning and abstract concept formation in children with NF1; assessment with the WISC-IV has shown performance deficits in the comprehension, similarities, incomplete pictures, arithmetic or picture arrangement subtests.15 In our study, the perceptual reasoning and working memory indices in the NF1G were lower than those of the CG. Both indices are intimately associated with the efficiency of executive functioning.
Most children with NF1 score lower in many cognitive functioning tests compared to controls.16 However, there are studies that challenge this conclusion. For instance, some authors have not found differences in the performance of children with NF1 in the picture arrangement subtest of the WISC.4 Others have reported on the results of the arithmetic subtest, in which children with NF1 did not have deficits compared to a children unaffected by the disease. Thus, the results of the latter study contradict ours, as we did find a statistically significant difference in the arithmetic subtest.17
Attention is one of the cognitive domains that have been studied most extensively in NF1. The work of Watt et al.18 has confirmed that affected children have difficulties performing tasks that require sustained attention. Our study corroborated this finding, as children in the NF1 group scored lower in the subtests that required a higher degree of sustained attention (incomplete pictures, digits and symbol search). We need to take into account that attention is the mechanism involved in accessing the information stored in the nervous system, so that problems with attention hinder learning and memory consolidation. Other cognitive domains, such as memory and language, are not as affected by NF1.19,20
In conclusion, our study revealed the presence of generalised cognitive deficits in the NF1 group. Along with impaired cognitive performance, assessed by the full scale IQ, we observed significant deficits in every assessed cognitive domain. Based on these findings, it would be advisable to offer individualised attention to children with NF1 during their schooling, as they are at higher risk of having learning difficulties. Early identification of children with NF1, along with their neuropsychological assessment and the development of cognitive stimulation programmes, could improve their academic outcomes and reduce the risk of school failure.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Hernández del Castillo L, Martínez Bermejo A, Portellano Pérez JA, Tirado Requero P, Garriz Luis A, Velázquez Fragua R. Rendimiento neuropsicológico en la neurofibromatosis tipo 1. An Pediatr (Barc). 2017;87:73–77.
