





Infant mortality is an indicator of child health, and an explanatory variable to reflect the socioeconomic development of a country. We aimed to examine the changes and trends of infant mortality in the European Union (EU) and its 28 member states in the 1994–2015 period.
MethodsWe extracted data of deaths in children aged less than one year between 1994 and 2015 from the Eurostat database. We analysed secular variation in the EU overall, by country and by geographical region using joinpoint regression analysis. We conducted additional analyses to examine neonatal and early neonatal mortality trends.
ResultsInfant mortality in the EU has declined significantly from 8.3 to 3.6 per 1000 live births (annual percent change=−3.8%; 95% confidence interval, −4.1 to −3.6). Among EU countries, we found the highest mortality rates throughout the study period in Romania and Bulgaria, and the lowest rates in Scandinavian countries (Finland, Sweden). There were significant decreasing trends in every country of the EU, which were most pronounced in former Soviet Baltic states and Eastern European countries, and least pronounced in Western European countries. Mortality rates have increased significantly in Greece in the last years, and plateaued in the United Kingdom and Ireland.
ConclusionsOur findings, which are based on official data, provide consistent evidence that infant mortality has declined steadily in the EU and its member states in the past decades, most markedly in Eastern European countries and former Soviet Baltic states. However, rates have risen or levelled off in some western countries in the past few years.
La mortalidad infantil es un indicador de la salud infantil y una variable explicativa del desarrollo socioeconómico. Nuestro objetivo fue examinar los cambios y tendencias de la mortalidad infantil en la Unión Europea (UE) y sus 28 países miembros en el período 1994-2015.
MétodosSe recopilaron datos de muertes de niños menores de un año entre 1994 y 2015 de la base de datos Eurostat. Estudiamos las tendencias en la UE, por países y regiones, utilizando el análisis de regresión joinpoint. Se condujeron análisis adicionales para estudiar las tendencias de mortalidad neonatal y neonatal precoz.
ResultadosLa mortalidad infantil en la UE ha disminuido significativamente de 8.3 a 3.6 por 1.000 (porcentaje de cambio anual=−3.8%, intervalos de confianza del 95% −4.1; −3.6). Las tasas de mortalidad más altas se registraron en Rumanía y Bulgaria, y las tasas más bajas en países escandinavos (Finlandia, Suecia). Se encontraron tendencias descendentes significativas en los países de la UE, más pronunciadas en los países bálticos exsoviéticos y países de Europa oriental, mientras que los países de Europa occidental mostraron los descensos menos pronunciados. La mortalidad infantil ha aumentado significativamente en Grecia en los últimos años, mientras que en el Reino Unido e Irlanda las tasas se han estabilizado.
ConclusionesLa mortalidad infantil ha disminuido en la UE y sus países en las últimas décadas, más pronunciadamente en los países de Europa oriental y los países bálticos exsoviéticos, mientras que en varios países de Europa occidental las tasas aumentaron o se han estabilizado en los últimos años.
Infant mortality rate (IMR) is defined as the number of deaths in children under 1 year of age per 1000 live births in the same year.1 The IMR is not only an important indicator of child health, but it is also used as an endpoint to be explained or as an explanatory variable to reflect the socioeconomic development of a country.2
Globally, infant mortality has declined steadily in the past decades, except in the region of sub-Saharan Africa. Maternal mortality and lack of access to sanitation have been identified as the main risk factors related to infant mortality.3 By country, the IMR has declined significantly in Egypt in the past decades, from 63 to 22 per 1000 live births, although socioeconomic disparities in childhood mortality remain.4 In Latin American countries, such as Argentina and Brazil, there have also been marked decreases in IMR.5,6 In Japan, the mean IMR decreased from 3.4 per 1000 live births in 1999 to 2.5 per 1000 live births in 2007, with regional variations.7 In South Korea, there has been a pronounced decreasing trend in recent years, from 9.9 per 1000 births in 1993 to 3.2 per 1000 live births in 2009.8 In the United States, trends have declined in the past decades for all deprived groups, from 19.2 per 1000 births in the 1969–1974 period to 7.5 per 1000 births in 1995–2000, while absolute socioeconomic disparities in infant mortality narrowed during the same period.9
The decrease in IMR has also been observed in some European countries.10–12 However, to date, no studies have examined infant mortality trends in the European Union using standardised methodologies. Therefore, the aim of our study was to use official data to analyse the trends in IMR in the entire European Union (EU) and its member states from 1994 to 2015.
MethodsWe used data from infant mortality rates from the 28 member states of the EU for the 1994–2015 period extracted from the European Statistical Office (Eurostat).13 Adhering to Eurostat's methodology, we defined infant mortality rate as the quotient of the number of deaths (due to all causes) of infants under 1 year of age during the year and the number of live births in the same year, expressed per 1000 live births. The database was updated on April 25, 2018.
The study population comprised the 28 member states of the EU: Belgium, Bulgaria, Czech Republic, Denmark, Germany, Estonia, Ireland, Greece, Spain, France (metropolitan), Croatia, Italy, Cyprus, Latvia, Lithuania, Luxembourg, Hungary, Malta, the Netherlands, Austria, Poland, Portugal, Romania, Slovenia, Slovakia, Finland, Sweden and the United Kingdom. There were data available for each country for every year in the 1994–2015 period. For France, we only used data from mainland France and the island of Corsica, and did not considered overseas departments and regions because we were unable to retrieve data for some of those territories for several years. We collected data and made calculations for the entire EU for the whole study period taking into account its current composition (the 28 member states).
We analysed regional infant mortality trends dividing the EU into 4 geographical regions: Northern (Denmark, Estonia, Finland, Ireland, Latvia, Lithuania, Sweden and the United Kingdom), Southern (Croatia, Cyprus, Greece, Italy, Malta, Portugal, Slovenia and Spain), Eastern (Bulgaria, Czech Republic, Hungary, Poland, Romania and Slovakia), and Western (Austria, Belgium, France, Germany, Luxembourg and the Netherlands). We calculated the average infant mortality rate in each region for each calendar year during the study period, and then examined the trend of the whole region.
We conducted additional analyses to examine neonatal and early neonatal mortality trends. The neonatal mortality rate is defined as the number of deaths of newborns aged less than 28 days in a year divided by the number of live births in the same year. The early neonatal mortality rate is defined as the number of deaths of newborns aged less than 1 week in a year divided by the number of live births in the same year. We excluded 4 countries (Belgium, Cyprus, Italy and Malta) from these analyses due to the lack of data for 7 or more years. We did not impute or extrapolate missing data.
We used the Joinpoint regression software (version 4.6.0.0, USA National Cancer Institute) to analyse significant changes in mortality trends. These analyses identified inflection points (called ‘joinpoints’) at which there were significant changes in the slope of the linear trend.14 The number and location of significant joinpoints for each country were determined using a log-linear model. We computed the estimated annual percent change (APC) and corresponding 95% confidence intervals (95% CI), which described the magnitude of the change for each of the identified trends. In this model, infant mortality rates were used as the dependent variable and the year of death as the independent variable. We defined statistical significance as a p-value of less than 0.05 in all of the analyses.
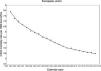
ResultsData on the IMRs in the EU and its member states is shown in Supplemental file 1. Between 1994 and 2015, the highest infant mortality rate in the EU corresponded to 1994 (8.3 per 1000). On the other hand, the lowest mortality rate was recorded in 2015 (3.6 per 1000).
Among the EU countries, the highest infant mortality rate was recorded in Romania in every year under study, peaking in 1994 (23.9 per 1000). In contrast, the lowest rates were found in Finland, Cyprus, Luxembourg, Slovenia and Sweden. We found the lowest rate in Slovenia in 2012 and 2015 and in Cyprus in 2013 (1.6 per 1000).
During the study period, there was an overall decrease in IMRs in the EU region (APC=−3.8%; 95% CI, −4.1 to −3.6), with two identifiable joinpoints. Between 1994 and 1996, infant mortality declined sharply (APC=−7.2%; 95% CI, −10.6 to −3.6). In the following years (1996–2008), rates also exhibited a significant decreasing trend, though less pronounced (APC=−4.2%; 95% CI, −4.5 to −4.0). Finally, in the last years (2008–2015), mortality rates exhibited an even milder declining trend, which was nevertheless still statistically significant (APC=−2.4%; 95% CI, −2.9 to −1.9) (Fig. 1).
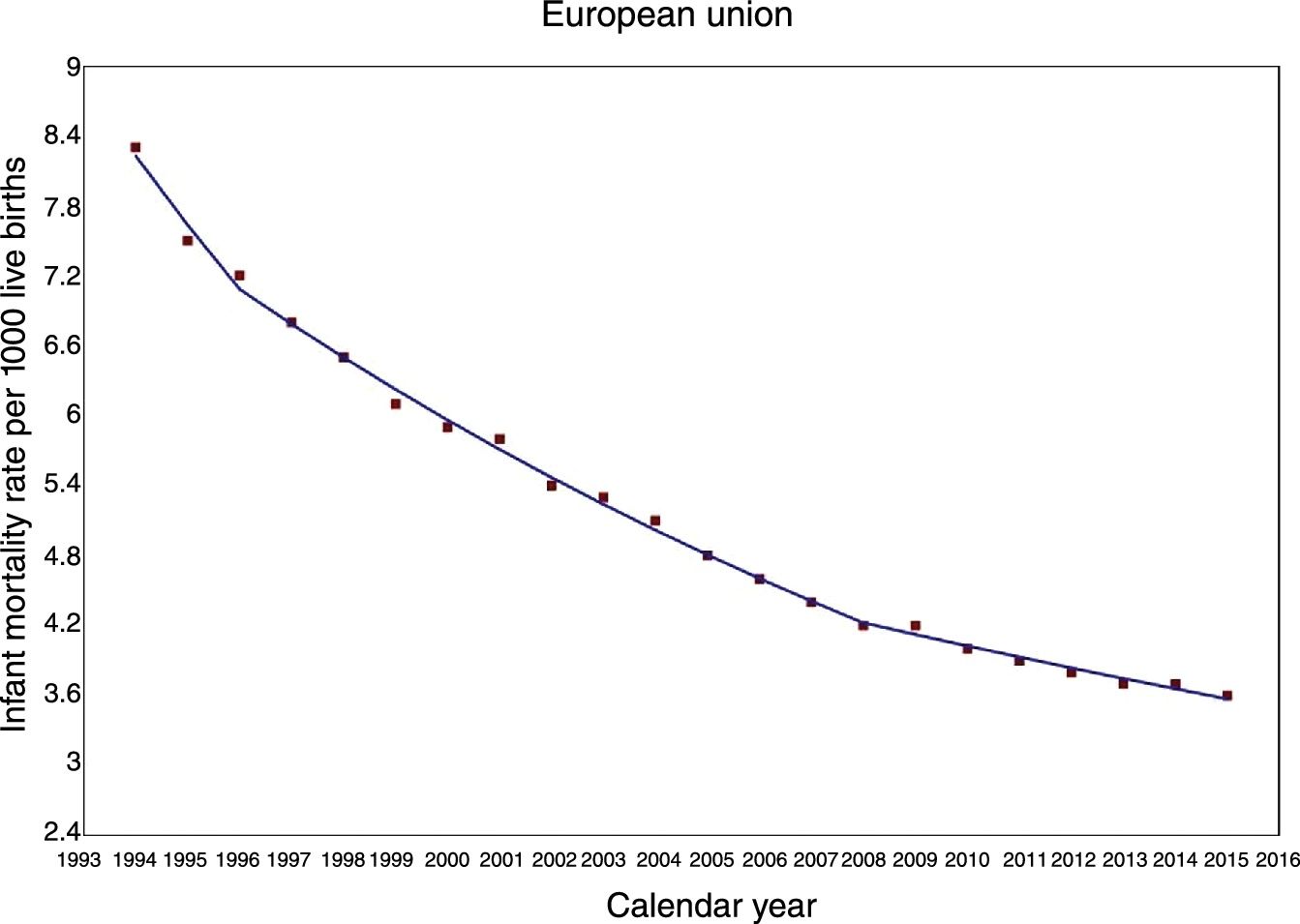
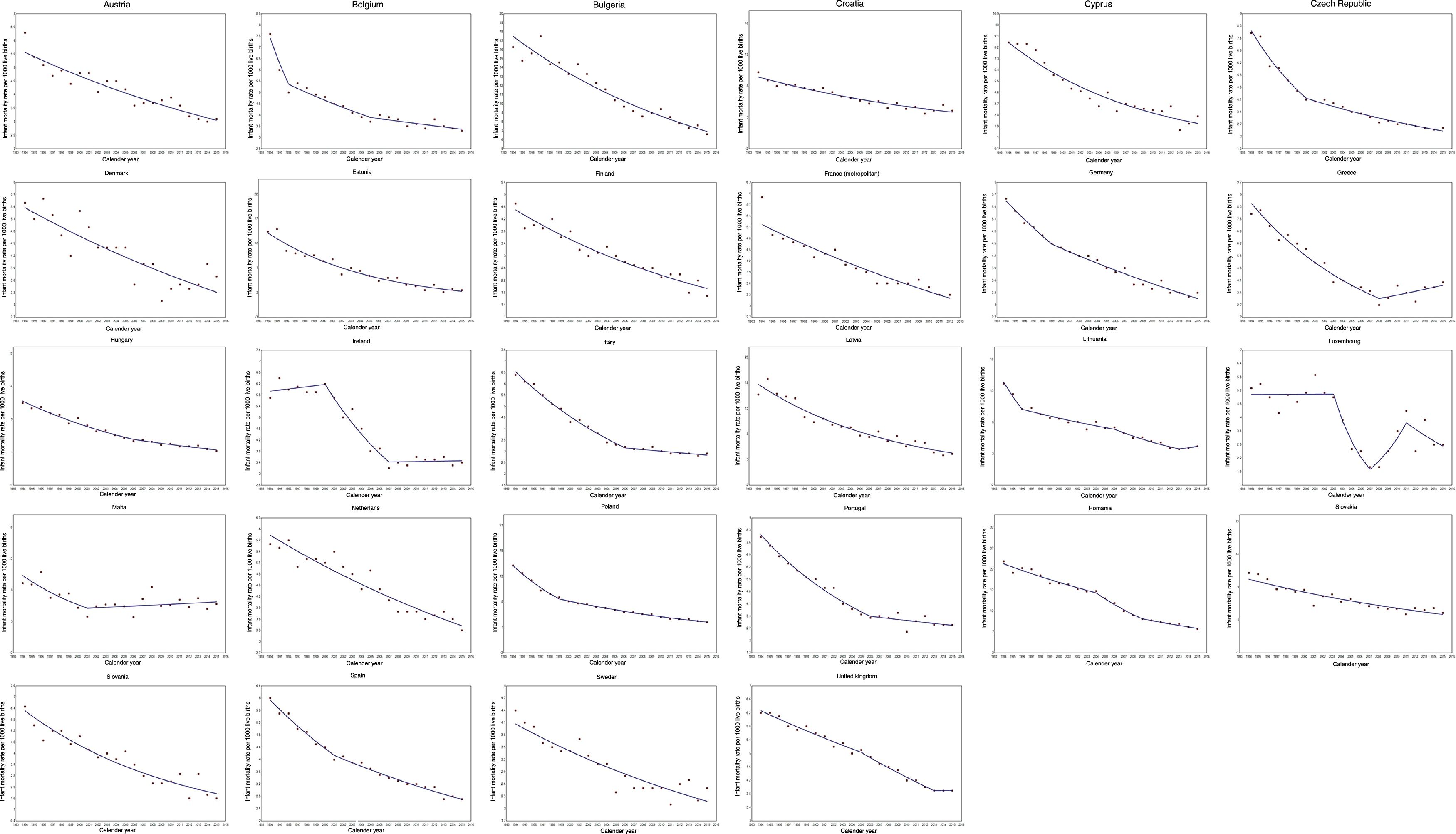
In the past 2 decades, IMRs decreased in every country in the EU. The largest decreases corresponded to Estonia (APC=−8.4%; 95% CI, −9.2 to −5.4), Latvia (APC=−6.6%; 95% CI, −7.3 to −5.8) and Cyprus (APC=−6.4%; 95% CI, −7.5 to −5.4), while the smallest decreases were observed in Malta (APC=−1.8%; 95% CI, −3.4 to −0.1), Denmark (APC=−2.3%; 95% CI, −2.9 to −1.6), Germany (APC=−2.5; 95% CI, −2.7 to −2.3) and the Netherlands (APC=−2.5%; 95% CI, −2.9 to −2.2).
In 8 countries (Belgium, Czech Republic, Germany, Hungary, Italy, Poland, Portugal and Spain), marked decreases in the IMR were recorded in the first years under study, followed by less pronounced descending trends. In contrast, the progressive decline of the IMR in Romania was less pronounced in an earlier period (1994–2004) with the steepest decreases occurring in the latter years under study. In the United Kingdom, mortality exhibited clear declining trends in the entire period under study except the last few years, when the IMR levelled off. Three countries (Greece, Malta and Lithuania) that had initially exhibited significant decreasing trends had an increasing trend in the past few years, although this trend was only significant in Greece. In Ireland and Luxembourg, mortality trends fluctuated (Table 1 and Fig. 2).
Joinpoint analysis of infant mortality trends in the European Union, 1994–2015.
| Total study period | Period 1 | Period 2 | Period 3 | Period 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Years | APCa (95% CIb) | Years | APCa (95% CIb) | Years | APCa (95% CIb) | Years | APCa (95% CIb) | Years | APCa (95% CIb) | |
| European Union | 1994–2015 | −3.8* (−4.1, −3.6) | 1994–1996 | −7.2* (−10.6, −3.6) | 1996–2008 | −4.2* (−4.5, −4.0) | 2008–2015 | −2.4* (−2.9, −1.9) | – | – |
| Austria | 1994–2015 | −2.8* (−3.3, −2.4) | – | – | – | – | – | – | – | – |
| Belgium | 1994–2015 | −3.0* (−3.6, −2.4) | 1994–1996 | −14.9* (−22.7, −6.3) | 1996–2005 | −3.5* (−4.5, −2.5) | 2005–2015 | −1.4* (−2.2, −0.7) | – | – |
| Bulgaria | 1994–2015 | −4.3* (−4.8, −3.9) | – | – | – | – | – | – | – | – |
| Croatia | 1994–2015 | −4.2* (−4.8, −3.6) | – | – | – | – | – | – | – | – |
| Cyprus | 1994–2015 | −6.4* (−7.5, −5.4) | – | – | – | – | – | – | – | – |
| Czech Republic | 1994–2015 | −5.2* (−5.9, −4.6) | 1994–2000 | −10.3* (−12.3, −8.3) | 2000–2015 | −3.9* (−4.4, −3.3) | – | – | – | – |
| Denmark | 1994–2015 | −2.3* (−2.9, −1.6) | – | – | – | – | – | – | – | – |
| Estonia | 1994–2015 | −8.4* (−9.2, −7.5) | – | – | – | – | – | – | – | – |
| Finland | 1994–2015 | −3.9* (−4.4, −3.4) | – | – | – | – | – | – | – | – |
| France | 1994–2012 | −2.6* (−3.0, −2.2) | – | – | – | – | – | – | – | – |
| Germany | 1994–2015 | −2.5* (−2.7, −2.3) | 1994–1999 | −4.1* (−5.8, −2.4) | 1999–2015 | −2.2* (−2.5, −1.9) | – | – | – | – |
| Greece | 1994–2015 | −4.4* (−5.5, −3.2) | 1994–2008 | −7.0* (−8.0, −6.0) | 2008–2015 | 3.2* (0.1, 6.3) | – | – | – | – |
| Hungary | 1994–2015 | −4.7* (−5.1, −4.3) | 1994–2006 | −5.6* (−6.2, −4.9) | 2006–2015 | −3.4* (−4.5, −2.3) | – | – | – | – |
| Ireland | 1994–2015 | −3.6* (−4.3, −2.9) | 1994–2000 | 0.7 (−1.9, 3.3) | 2000–2007 | −8.1* (−10.4, −5.7) | 2007–2015 | 0.2 (−1.5, 1.8) | – | – |
| Italy | 1994–2015 | −4.0* (−4.6, −3.5) | 1994–2006 | −5.9* (−6.3, −5.4) | 2006–2015 | −1.2* (−1.9, −0.5) | – | – | – | – |
| Latvia | 1994–2015 | −6.6* (−7.3, −5.8) | – | – | – | – | – | – | – | – |
| Lithuania | 1994–2015 | −5.6* (−6.1, −5.0) | 1994–1996 | −16.4 (−30.6, 0.6) | 1996–2006 | −3.7* (−5.3, −2.1) | 2006–2013 | −8.3* (−11.1, −5.4) | 2013–2015 | 5.2 (−12.6, 26.7) |
| Luxembourg | 1994–2015 | −3.6* (−5.6, −1.7) | 1994–2003 | 0.0 (−3.8, 4.0) | 2003–2007 | −23.8* (−38.4, −5.7) | 2007–2011 | 22.0 (−1.4, 51.0) | 2011–2015 | −7.7 (−19.4, 5.6) |
| Malta | 1994–2015 | −1.8* (−3.4, −0.1) | 1994–2001 | −9.5* (−15.9, −2.7) | 2001–2015 | 1.3 (−1.3, 3.9) | – | – | – | – |
| Netherlands | 1994–2015 | −2.5* (−2.9, −2.2) | – | – | – | – | – | – | – | – |
| Poland | 1994–2015 | −5.6* (−6.1, −5.1) | 1994–1999 | −10.7* (−12.1, −9.3) | 1999–2015 | −4.6* (−4.8, −4.3) | – | – | – | – |
| Portugal | 1994–2015 | −4.9* (−5.7, −4.2) | 1994–2006 | −6.9* (−8.2, −5.7) | 2006–2015 | −1.8 (−3.9, 0.2) | – | – | – | – |
| Romania | 1994–2015 | −5.5* (−5.9, −5.0) | 1994–2004 | −3.5* (−4.2, −2.8) | 2004–2009 | −9.1* (−11.7, −6.4) | 2009–2015 | −4.2* (−5.7, −2.7) | – | – |
| Slovakia | 1994–2015 | −3.5* (−4.1, −2.9) | – | – | – | – | – | – | – | – |
| Slovenia | 1994–2015 | −5.6* (−6.6, −4.7) | – | – | – | – | – | – | – | – |
| Spain | 1994–2015 | −3.6* (−3.8, −3.3) | 1994–2001 | −5.0* (−6.0, −4.1) | 2001–2015 | −3.0* (−3.4, −2.7) | – | – | – | – |
| Sweden | 1994–2015 | −2.9* (−3.5, −2.3) | – | – | – | – | – | – | – | – |
| United Kingdom | 1994–2015 | −2.4* (−2.6, −2.3) | 1994–2005 | −2.0* (−2.3, −1.6) | 2005–2013 | −3.1* (−3.8, −2.5) | 2013–2015 | 0.0 (−4.9, 5.2) | – | – |
In the 1994–2015 period, all 4 EU regions showed significant downward trends. The most pronounced declining trends were observed in Northern (APC=−4.9%; 95% CI, −5.2 to −4.7) and Eastern Europe (APC=−4.8%; 95% CI, −5.0 to −4.6). Conversely, Western Europe exhibited slightest decreasing trend (APC=−2.8%; 95% CI, −3.1 to −2.4).
Aside from Northern Europe, the remaining 3 regions exhibited significant changes in trends through the study period. In Eastern and Southern Europe, we found a pronounced decreasing trend in an initial period, and a milder declining trend thereafter. In Western Europe, we found fluctuating trends throughout the study period (Table 2).
Joinpoint analysis for infant mortality trends by European regions, 1994–2015.
| Total study period | Period 1 | Period 2 | Period 3 | Period 4 | Period 5 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Years | APCa (95% CIb) | Years | APCa (95% CIb) | Years | APCa (95% CIb) | Years | APCa (95% CIb) | Years | APCa (95% CIb) | Years | APCa (95% CIb) | |
| Eastern Europe | 1994–2015 | −4.8* (−5.0, −4.6) | 1994–2009 | −5.1* (−5.4, −4.9) | 2009–2015 | −3.7* (−4.8, −2.6) | – | – | – | – | – | – |
| Northern Europe | 1994–2015 | −4.9* (−5.2, −4.7) | – | – | – | – | – | – | – | – | – | – |
| Southern Europe | 1994–2015 | −4.2* (−4.7, −3.7) | 1994–2006 | −5.7* (−6.2, −5.2) | 2006–2015 | −1.8* (−2.6, −1.0) | – | – | – | – | – | – |
| Western Europe | 1994–2015 | −2.8* (−3.1, −2.4) | 1994–1997 | −7.3* (−11.3, −3.0) | 1997–2001 | 0.4 (−4.0, 5.0) | 2001–2007 | −5.4* (−7.3, −3.5) | 2007–2011 | 0.7 (−3.7, 5.3) | 2011–2015 | −2.8 (−5.5, 0.0) |
For both neonatal and early neonatal mortality, the data showed downward trends with values similar to the IMRs found in most European countries, except in Luxembourg, where the decline in early neonatal mortality was not statistically significant (APC=−2.9; 95% CI, −6.1 to 0.5). Joinpoint regression results are shown in Supplemental files 2 and 3.
In Austria, Latvia and Luxembourg, we found more pronounced decreases in neonatal mortality compared to early neonatal mortality. On the contrary, in France, Greece, Hungary, Portugal and Slovakia, early neonatal mortality exhibited more pronounced declines compared to neonatal mortality. We did not observe substantial differences in any of the remaining countries between neonatal and early neonatal mortality rate trends (differences between the APCs of 0.5 or less).
DiscussionTo the best of our knowledge, this is the first study analysing the trends in IMRs in the EU based on official data. Our results indicate that in the 1994–2015 period, the IMR for the EU overall and for its member states showed significant downward trends. Our analysis by region found the most pronounced declines in Northern and Eastern Europe. We also found similar declining trends in most European countries in the neonatal and early neonatal mortality rates.
Previous studies have examined trends in infant mortality in some European countries. An Irish study found a non-linear downward trend in infant mortality between 1984 and 2005, with a mean annual decline in the IMR of 0.27 per 1000 live births.10 In Hungary, the annual IMR in infants under 1 year decreased from a maximum of 42.9 per 1000 live births in 1963 to a minimum of 4.9 per 1000 live births in 2012.11 In Greece, after a long-term decline in infant mortality, the trend reversed, with the IMR increasing substantially (by 43% between 2008 and 2010).15 Altogether, these findings are consistent with the results presented in this study.
Several reasons may explain the overall downward trend recorded in the whole EU and its countries. One main factor is the development and use of vaccines, which have played a role in reducing infant mortality by infectious causes.16–18 McGovern and Canning19 reported that the relative risk of death is 27% lower in fully vaccinated children compared to unvaccinated children. Moreover, the inclusion of new vaccines in routine infant immunization schedules, such as pneumococcal conjugate vaccines, might have contributed to lower mortality rates.20,21 Although the European region (out of the 6 World Health Organization regions) has been found to be the region with the highest levels of scepticism about the importance, safety and effectiveness of vaccination,22 a recent report showed that coverage vaccination for DTP (diphtheria, tetanus, pertussis) in Europe ranged from 89.1% in Romania to over 98% in Scandinavian countries.23 Therefore, we speculate that high vaccination coverages for basic vaccines might explain, to some extent, the descending trends observed.
The improvement of economic and social conditions in the past decades could provide another reasonable explanation for our findings. In this line, prior studies have stressed the crucial role of the welfare state (percentage of public health care expenditure, percentage of the population with medical care coverage, reduction in income inequalities) in reducing infant mortality.24–26 In addition, other authors have pointed out the impact of income distribution on infant health. Findings of a preliminary systematic review suggested that higher income inequalities were associated with high rates of infant mortality.27 Olson et al.28 found a positive correlation between income inequality (as measured with the Gini coefficient) and infant mortality. However, other studies have not found this adverse association,29,30 and thus the relationship between income inequalities and infant mortality has yet to be fully elucidated.
Thus, the reviewed evidence suggests that the clear overall declining trends observed across European countries could be attributed to advances in the welfare state and social welfare policies. However, it should be noted that welfare and welfare policies differ notably among European countries. This might explain why we found the lowest IMRs throughout the study period in Scandinavian countries, characterized by universal governmental support and small income inequalities. On the other hand, Central and Eastern European countries and former Soviet Baltic states, which had the highest IMRs, experienced an epidemiological shift31 after 1990. The political and social transformations and the economic development in these countries may have led to changes in public health policies and social protection that could explain the pronounced declining trends from this moment. In the same line, Asandului et al.32 concluded that socioeconomic and demographic factors, which are intimately related to health factors, may explain the reduction in IMRs observed in Central and Eastern European countries.
In Greece, we found a clear decreasing trend between 1994 and 2008, followed by a significant upward trend thereafter. We hypothesize that this remarkable finding could be a consequence of the economic world crisis. An ecological study found that the unemployment rate was the socioeconomic determinant that exhibited the strongest correlation with infant mortality.33 Also, the authors of another study that evaluated the medium-term impact of the economic crisis in Greece reported that the proportion of Greek adults that declared having unmet healthcare needs had increased significantly.34 Therefore, the context of the economic downturn, when Greek unemployment rate skyrocketed leading to a deterioration of the welfare state and public health services, provides a plausible explanation to our findings.
One issue that deserves further discussion is the underreporting of infant mortality in some countries. Prior studies have suggested that official statistics from Eastern European countries, such as Bulgaria or Romania, may not represent actual mortality rates accurately, while in Central European countries and the Baltic countries, official statistics corresponded to actual rates.35 However, Eurostat assesses the comparability of the data collected from national statistical offices, and ensures internal consistency using different validation processes. Thus, we do not expect our findings to be substantially affected by this issue.
According to the WHO, 17–42% of infant deaths in Europe can be attributed to congenital anomalies.36 Prenatal congenital malformation screening programmes that may be associated with an increase in voluntary terminations of pregnancy due to foetal anomalies may have an impact on infant mortality statistics by decreasing the number of infants at high risk of dying early, artificially reducing the infant mortality rate. Nevertheless, given the differences in national policies and recommendations for prenatal screening between countries,37 and the different attitudes towards termination of pregnancy (at both the socialand individual levels), we speculate that the impact of these policies on the marked decrease in infant mortality rates observed in our study is probably limited and remains to be determined.
On the other hand, the mean maternal age at first birth has gradually increased in European countries.38 Advanced maternal age has been associated with higher perinatal mortality rates,39,40 although this association was not reflected in our findings. We hypothesize that societal changes and occupational factors could have led women with higher educational attainment and socioeconomic status to postpone childbearing. Nonetheless, these advantageous socioeconomic conditions might ameliorate adverse perinatal outcomes when these women have a child at advanced ages.
It is worth noting that the results for Cyprus, Malta and Luxembourg should be interpreted with caution. These countries have the smallest populations in the EU, and which could have a substantial impact on infant mortality trends.
This study presents a novel and updated analysis of infant mortality trends in the whole EU and its 28 member states. The use of official data, reviewed and validated by the European Statistical Office, ensures the validity of our findings. Still, we should highlight some limitations of our study. An intrinsic limitation in a study aiming to examine infant mortality trends across 28 countries is the marked differences in welfare, healthcare systems, and public health policies between nations. We are fully aware of this limitation and duly acknowledge it. Another limitation was our inability to perform additional analyses to study trends in the main causes of infant mortality in the EU due to the lack of data in Eurostat for the whole study period.
In conclusion, infant mortality in the entire EU and its member states has consistently declined in the past decades. Scandinavian and Western European countries exhibited low mortality rates that declined progressively in the past two decades. In Eastern European countries and Baltic states, political changes and socioeconomic development were associated with pronounced decreasing trends in infant mortality. The fact that mortality rates have risen in recent years in Greece or levelled off in the United Kingdom and Ireland evince the importance of continuing to promote public health strategies to reduce infant mortality. The long-term effects of the economic crisis in European countries deserve further study.
Conflicts of interestThe authors declare that they have no conflicts of interest.
The following are the supplementary data to this article:



Please cite this article as: Onambele L, Martin-Rodríguez LS, Niu H, Alvarez-Alvarez I, Arnedo-Pena A, Guillen-Grima F, et al. Mortalidad infantil en la Unión Europea: análisis de tendencias en el período 1994-2015. An Pediatr (Barc). 2019;91:219–227.
