
A previously healthy boy aged 13 years was admitted with sudden acute abdominal pain. The family reported weekly nocturnal vomiting episodes over a 6-month period.
At admission, the patient was in shock, with a distended and rigid abdomen, respiratory failure and decreased level of consciousness due to global hypoperfusion secondary to abdominal compartment syndrome. This prompted intubation and initiation of fluid resuscitation and vasoactive drugs. The abdominal radiograph showed massive gastric distension with small and large bowel displacement. An emergency exploratory laparotomy revealed multiple gastric perforations, leading to performance of partial gastrectomy (Fig. 1). The antimicrobial spectrum was broadened, with administration of carbapenems, metronidazole, vancomycin and antifungals. The patient underwent progressive deterioration with multiple organ failure, including acute kidney injury requiring continuous renal replacement and acute liver failure requiring therapeutic plasma exchange.

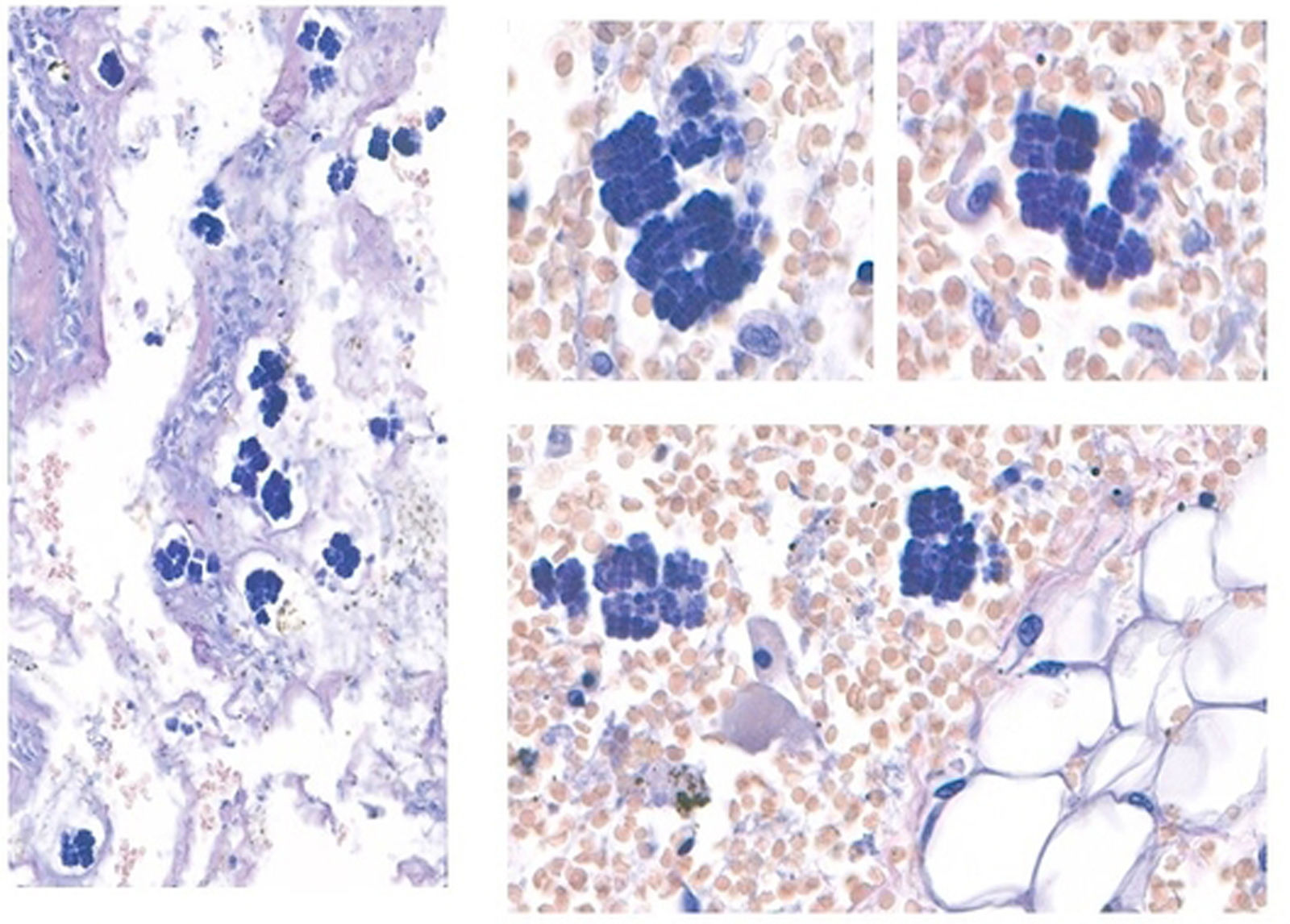
The histological examination of gastric specimen revealed pathogenic colonization by Clostridium ventriculi (Fig. 2). In spite of the care provided, the patient died.
, each measuring 1.8 to 3&#¿;μm, arranged in tetrads or octets forming cuboid structures.")
Histological examination of the surgical gastric specimen. Standard haematoxylin-eosin staining revealed diffuse haemorrhagic areas with extensive ischaemic necrosis of the mucosa and submucosa and the presence of C ventriculi bacteria with characteristic microscopic features: spherical basophilic bacteria (cocci), each measuring 1.8 to 3&#¿;μm, arranged in tetrads or octets forming cuboid structures.
Clostridium ventriculi (also known as Sarcina ventriculi) is an anaerobic gram-positive coccus mainly transmitted through ingestion of contaminated soil present in food.1 The main risk factor is delayed gastric emptying. Intramural gas accumulation from bacterial fermentation byproducts results in emphysematous gastritis, with a mortality of 75%.2 Very few paediatric cases have been reported to date,3 and the one we present here is the first with a fatal outcome.
The diagnosis can be made with the observation of the tetrad packet arrangement of C ventriculi with haematoxylin-eosin staining (Fig. 2).

