








Childhood excess weight is a growing public health problem. The aim of this study was to assess temporal trends in the prevalence of overweight, obesity and central obesity in schoolchildren aged 6–9 years in Spain between 2011 and 2019 based on demographic and socioeconomic characteristics.
MethodologyThe analysis included data from the 2011, 2015 and 2019 rounds of the cross-sectional observational and descriptive ALADINO study in schoolchildren of both sexes aged 6–9 years. We conducted a descriptive analysis of the trends in the prevalence of overweight and obesity (defined according to the criteria of the World Health Organization and the International Obesity Task Force) and of central obesity, in addition to associated demographic and socioeconomic variables.
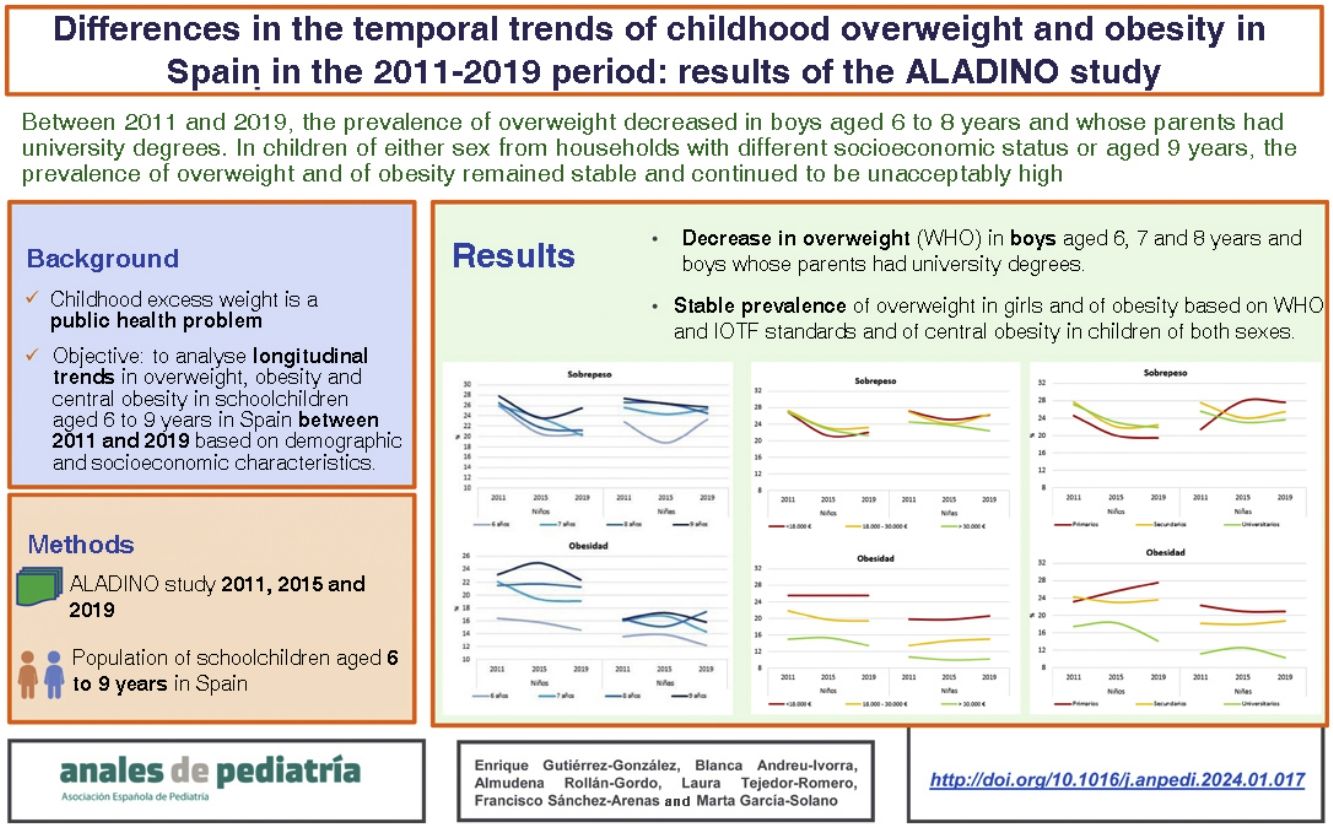
ResultsBetween 2011 and 2019, the prevalence of overweight (WHO criteria) decreased in boys aged 6, 7 and 8 years (by −5.4%, −5.7% and −5.3%, respectively) and boys whose parents had a higher educational attainment (by −5.3%). In relation to the socioeconomic level, overweight in boys declined at all income levels. However, between 2011 and 2019, both the prevalence of overweight in girls and the prevalence of obesity (applying the WHO and IOTF criteria) and the prevalence of central obesity in both sexes remained stable.
ConclusionsThe prevalence of overweight and the prevalence of obesity in schoolchildren aged 6–9 years in Spain remain high. Between 2011 and 2019, the prevalence of overweight in children aged 6–8 years and in children whose parents had university degrees decreased, whereas obesity in boys, overweight and obesity in girls and central obesity in both sexes remained stable.
El exceso de peso infantil es un problema de salud pública creciente. El objetivo del trabajo es estudiar la evolución de la prevalencia de sobrepeso, obesidad y obesidad central en escolares de 6 a 9 años en España entre 2011 y 2019 según características demográficas y socioeconómicas.
MetodologíaSe incluyeron las rondas 2011, 2015 y 2019 del estudio observacional, descriptivo y transversal ALADINO en escolares de ambos sexos de 6 a 9 años. Se realizó un análisis descriptivo de la evolución de la prevalencia de sobrepeso y obesidad según los criterios de la Organización Mundial de la Salud (OMS) y la International Obesity Task Force (IOTF), así como obesidad central, y las variables demográficas y socioeconómicas asociadas.
ResultadosEntre 2011 y 2019 se redujo la prevalencia de sobrepeso (critrerios OMS) en niños de 6, 7 y 8 años (−5,4, −5,7 y −5,3 puntos porcentuales respectivamente) y niños cuyos progenitores tenían estudios superiores (−5,3 puntos porcentuales). Por renta, el sobrepeso en niños se redujo en todos los niveles de ingresos. Sin embargo, entre 2011 y 2019, se mantuvieron estables tanto la prevalencia de sobrepeso en niñas como la prevalencia de obesidad según las referencias OMS e IOTF y la de obesidad central en ambos sexos.
ConclusionesLas prevalencias de sobrepeso y obesidad en escolares de 6 a 9 años en España siguen siendo altas. Entre 2011 y 2019 disminuyó la prevalencia de sobrepeso en niños de 6 a 8 años y aquellos cuyos progenitores tienen estudios universitarios, mientras que la obesidad en niños, el sobrepeso y la obesidad en niñas, y la obesidad central en ambos sexos han permanecido estables.
Childhood overweight and obesity, which combined are referred to as excess weight, constitute a public health problem1 and are associated with an increased risk of type 2 diabetes, hypertension, metabolic syndrome and psychosocial disorders2 in addition to cardiovascular disease and some types of cancer in adulthood.3 As regards its magnitude and temporal trends, the latest report Childhood Obesity Surveillance Initiative (COSI) of the World Health Organization (WHO) Regional Office for Europe from 2022 shows a prevalence of obesity of 14% in boys and 10% in girls aged 6–9 years,4 with higher proportions in Mediterranean countries, including Spain. In the European population aged 5–19 years, the prevalence of obesity has increased by 40% and the prevalence of excess weight by 20% between 2007 and 2016.2,5
Childhood excess weight is a multifactorial problem that results from the interaction of various genetic, environmental and socioeconomic factors, which are in turn related to the family, community and school environments.2,5,6 To address this problem, several initiatives have been launched both at the national level in Spain (Estrategia para la Nutrición, Actividad Física y Prevención de la Obesidad [NAOS, Strategy for Nutrition, Physical Activity and Obesity Prevention]7; Plan Estratégico Nacional para la Reducción de la Obesidad Infantil [National Strategic Plan for the Reduction of Childhood Obesity] 2022-20308) and at the European level (European Union Action Plan on Childhood Obesity 2014–2020).9 In addition, nutrition and health are included among the Sustainable Development Goals10 of the 2030 Agenda for Development of the United Nations and the European Food and Nutrition Action Plan 2015–2020,11 in the context of which one of the key goals is to support surveillance, monitoring, evaluation and research in these fields. The study of trends in childhood obesity and overweight indicators is essential to assess the impact of these initiatives and to guide the design and implementation of future strategies.7
Two recent meta-analysis that include data for Spain and based on anthropometric data reported by parents disagree as to the increase or decrease of childhood obesity in Spain.12,13 At present, there are no studies in the literature analysing trends in overweight and obesity based on objective anthropometric measurements in the 6- to 9-years age group that can confirm or refute these hypotheses. The aim of our study was to assess the temporal trends in overweight, obesity and central obesity based on objective anthropometric data in schoolchildren aged 6–9 years in Spain between 2011 and 2019 and in relation to sex, household income and parental educational attainment.
MethodsDesign and participantsThe ALADINO study in Spain, developed in the framework of the Childhood Obesity Surveillance Initiative (COSI) of the World Health Organization (WHO), has already undergone four rounds (2011, 2013, 2015 and 2019).1,14,15 The ALADINO study is a cross-sectional observational and descriptive study in schoolchildren aged 6–9 years in Spain. Previous publications offer a detailed description of the study design.14,15 In the study presented in this article, we analysed the scrubbed and standardised datasets corresponding to the 2011, 2015 and 2019 rounds (with the approval of the Ethics Committee for Clinical Trials of the Hospital Clínico San Carlos de Madrid), obtained with comparable protocols and in comparable samples (schoolchildren aged 6–9 years).
The study sample and the sample size for each round were established in conformity with the COSI protocol and procedures.16,17 The sample was obtained through multistage cluster sampling (primary schools) stratified by autonomous community and municipality size, selecting centres from the primary school register of the Ministry of Education. A representative sample of schoolchildren aged 6–9 years in Spain was selected starting with the selection of schools, followed by the random selection of a classroom per year (from years 1–4 of Spanish primary education) and the inclusion of all the schoolchildren in the selected classrooms whose parents or legal guardians gave signed informed consent to participation and who attended school on the day the anthropometric assessment took place. The participation rate was 59.4% in 144 schools in 2011, 73.1% in 165 schools in 2015 and 63.9% in 276 schools in 2019.
VariablesIn each round, a team of trained professionals measured the weight, height and waist circumference with calibrated equipment. The body mass index was calculated (BMI = weight [kg]/height2 [m2)]) and weight status classified according to the WHO growth reference 18 and the criteria of the International Obesity Task Force (IOTF).19 Central/abdominal obesity was assessed through the calculation of the waist-to-height ratio (WHtR) and defined as a WHtR greater than 0.5.19 We analysed inequality factors disaggregating the data by sex, age and household socioeconomic variables—household income and parental educational attainment—obtained through self-report questionnaires20 designed according to the COSI recommendations.
Statistical analysisWe have summarised quantitative data using the mean, standard deviation, median and interquartile range. We summarised qualitative data as absolute frequencies, percentages and 95% confidence intervals. The association between qualitative variables was assessed with the χ2 test and the association between quantitative variables with the Student t test. Statistical significance was defined as P < .05. We present the results as absolute and relative differences in prevalence between the years under study. We used bootstrapping to improve the precision of estimates in the calculation of confidence intervals. The analysis was carried out with the Stata software package, version 16.
ResultsA cumulative total of 35 223 schoolchildren aged 6–9 years participated in the ALADINO 2011, 2015 and 2019 rounds of the ALADINO study, with a similar sex distribution in each round (Appendix B, Supplemental Table A1). We did not find significant differences between the sexes in the weight, height, waist circumference, BMI and WHtR values in any of the rounds (Table 1).
Anthropometric measurements by sex (mean, standard deviation and percentiles) en in the ALADINO study 2011, 2015 and 2019 rounds.
| Mean | SD | Median | IQR | Mean | SD | Median | IQR | |
|---|---|---|---|---|---|---|---|---|
| Boys 2011 | Girls 2011 | |||||||
| Weight (kg) | 30.7 | 7.5 | 29.4 | 9.7 | 30.1 | 7.5 | 28.8 | 9.9 |
| Height (cm) | 129.9 | 8.4 | 129.9 | 12.2 | 129 | 8.6 | 128.8 | 12.4 |
| BMI (kg/m2) | 18 | 2.9 | 17.3 | 3.5 | 17.8 | 2.9 | 17.2 | 3.7 |
| Waist (cm) | 61.1 | 7.6 | 59.7 | 9.6 | 60.2 | 7.7 | 58.7 | 9.6 |
| Waist-height ratio | 0.47 | 0.05 | 0.46 | 0.06 | 0.47 | 0.05 | 0.46 | 0.07 |
| Boys 2015 | Girls 2015 | |||||||
| Weight (kg) | 30 | 7.8 | 28.4 | 9.6 | 29.5 | 7.7 | 28 | 9.7 |
| Height (cm) | 129.4 | 8.8 | 129.3 | 12.5 | 128.5 | 8.8 | 128.1 | 12.4 |
| BMI (kg/m2) | 17.7 | 3.0 | 16.9 | 3.6 | 17.7 | 3.1 | 16.9 | 3.8 |
| Waist (cm) | 60.6 | 8.1 | 59 | 10 | 59.8 | 8 | 58.5 | 10.0 |
| Waist-height ratio | 0.47 | 0.05 | 0.46 | 0.06 | 0.47 | 0.05 | 0.46 | 0.07 |
| Boys 2019 | Girls 2019 | |||||||
| Weight (kg) | 30 | 7.7 | 28.4 | 9.7 | 29.6 | 7.7 | 28.0 | 9.7 |
| Height (cm) | 129.7 | 8.9 | 129.6 | 12.8 | 128.6 | 9.0 | 128.5 | 12.6 |
| BMI (kg/m2) | 17.6 | 3.0 | 16.8 | 3.5 | 17.7 | 3.0 | 17.0 | 3.8 |
| Waist (cm) | 60.5 | 8.0 | 59.0 | 9.4 | 59.7 | 8 | 58.1 | 10.0 |
| Waist-height ratio | 0.47 | 0.05 | 0.46 | 0.06 | 0.46 | 0.05 | 0.46 | 0.06 |
IQR, interquartile range; SD, standard deviation.
The prevalence of overweight (WHO reference) decreased by 18% (a reduction of 4.8 percent points) between 2011 and 2019 in boys aged 6–9 years and did not exhibit significant changes in girls. The prevalence of obesity and the prevalence of severe obesity remained stable in both sexes. Applying the IOTF criteria, the prevalence of overweight decreased by 14% in boys (reduction of 3.3 percent points), with no changes in girls and in the prevalence of obesity and of severe obesity in either sex. The prevalence of central obesity (WHtR > 0.5) did not change either in either sex between 2011 and 2019 (Table 2).
Prevalence of overweight, obesity, severe obesity (WHO and IOTF) and central obesity (IOTF) in schoolchildren by sex in the ALADINO study 2011, 2015 and 2019 rounds.
| 2011 | 2015 | 2019 | ||||
|---|---|---|---|---|---|---|
| % | [95% CI] | % | [95% CI] | % | [95% CI] | |
| Boys | ||||||
| WHO | ||||||
| Overweight | 26.7 | [25.2−28.2] | 22.4 | [20.9−23.9] | 21.9 | [20.9−23.0] |
| Obesity | 20.9 | [19.6−22.3] | 20.4 | [19.0−21.9] | 19.4 | [18.4−20.4] |
| Severe obesitya | 6.0 | [5.3−6.8] | 5.5 | [4.7−6.3] | 5.9 | [5.4−6.5] |
| IOTF | ||||||
| Overweight | 23.8 | [22.4−25.2] | 21.5 | [20.0−23.0] | 20.5 | [19.5−21.5] |
| Obesity | 10.9 | [9.9−11.9] | 10.6 | [9.6−11.8] | 10.5 | [9.7−11.2] |
| Severe obesitya | 2.5 | [2.0−3.0] | 2.7 | [2.2−3.3] | 3.0 | [2.6−3.5] |
| Obesity central | ||||||
| Obesity central | 23 | [21.5−24.3] | 22.4 | [20.7−23.5] | 22.4 | [21.1−23.2] |
| Girls | ||||||
| WHO | ||||||
| Overweight | 25.7 | [24.2−27.1] | 23.9 | [22.4−25.5] | 24.7 | [23.6−25.9] |
| Obesity | 15.5 | [14.4−16.8] | 15.8 | [14.5−17.2] | 15.0 | [14.1−15.9] |
| Severe obesitya | 2.2 | [1.7−2.7] | 2.3 | [1.8−2.9] | 2.3 | [20.0−2.7] |
| IOTF | ||||||
| Overweight | 24.6 | [23.2−26.1] | 22.2 | [20.7−23.7] | 23.6 | [22.5−24.7] |
| Obesity | 11.2 | [10.2−12.3] | 11.8 | [10.7−13.1] | 11.4 | [10.6−12.2] |
| Severe obesitya | 2.5 | [2.0−3.0] | 2.8 | [2.3−3.4] | 2.8 | [2.4−3.2] |
| Central obesity | ||||||
| Central obesity | 22.4 | [20.8−23.6] | 23.9 | [21.8−24.9] | 22.8 | [21.6−23.8] |
CI, confidence interval; IOTF, International Obesity Task Force; WHO, World Health Organization.
In every round, obesity and severe obesity (WHO reference) were more prevalent in boys, while overweight went from being more prevalent in boys in 2011 to being more prevalent in girls from 2015 (Table 2).
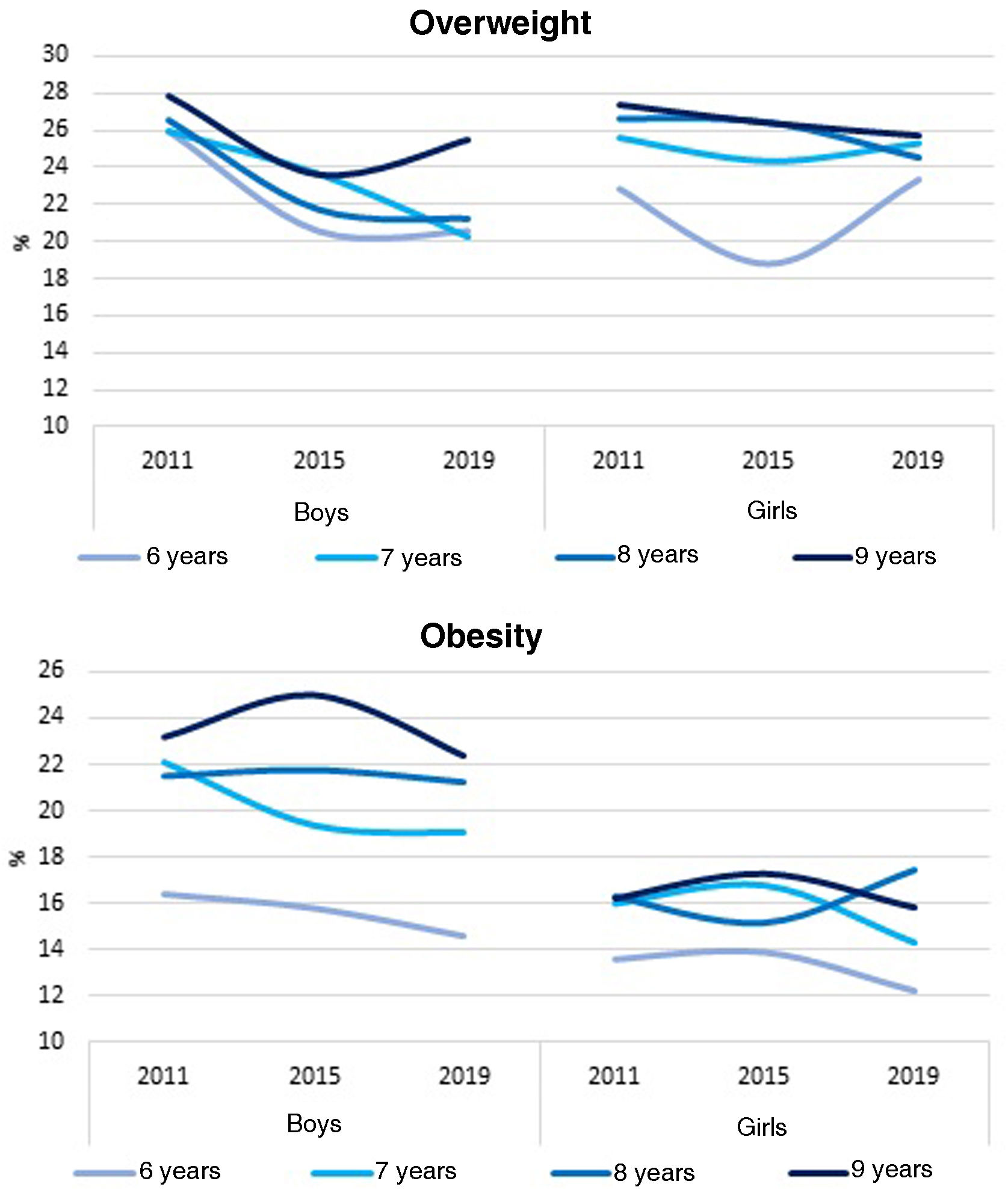
By age group, between 2011 and 2019 there was a significant decrease in the prevalence of overweight in boys aged 6, 7 and 8 years by –5.4, –5.7 and –5.3 percent points, respectively, based on the WHO reference data (Fig. 1; Appendix B Supplemental Table A2), while applying the IOTF criteria, there was only a reduction in boys aged 8 years (–5.8 percent points) (Appendix B Supplemental Table A2). In girls, the prevalence of overweight remained stable applying either standard (WHO/IOTF) The prevalence of obesity and of severe obesity remained stable applying either standard, and the prevalence of central obesity remained unchanged in both sexes and in every age group (Fig. 1, Appendix B Supplemental Table A2).
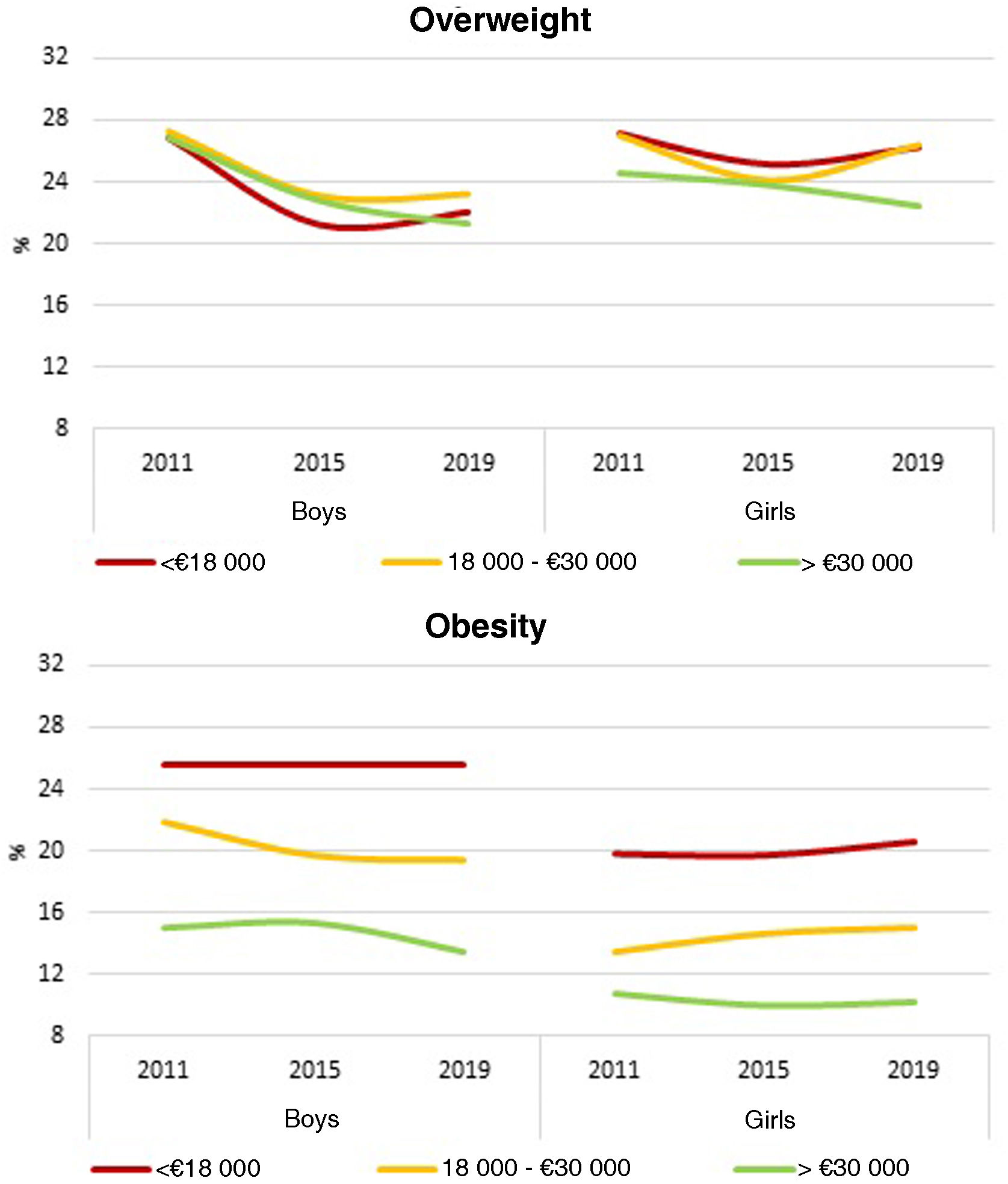
By income, between 2011 and 2019 there was a significant decrease in the prevalence of overweight (WHO reference) in boys from households with low as well as high incomes (changes of –4.8 and –5.5 percent points, respectively), whereas applying the IOTF criteria, the decrease was only significant in boys from high-income households (change of –4.7 percent points) (Fig. 2, Appendix B Supplemental Table A3). Among girls, there were no relevant changes in the prevalence of overweight between income levels (WHO and IOTF). The prevalence of obesity (WHO and IOTF) did not change significantly based on household income and sex, although it exhibited a sustained reverse income gradient in children of both sexes throughout the study period, as the prevalence of obesity in boys and girls from low-income households nearly doubled that in schoolchildren from higher-income households in every round of the study (Appendix B Supplemental Table A3).
In relation to parental educational attainment, the prevalence of overweight (WHO reference) decreased significantly in boys with parents who had completed secondary education and university degrees (–5.3 percent points in both groups) (Fig. 3, Appendix B Supplemental Table A4). Applying the IOTF criteria, overweight only decreased in boys with parents who had university degrees (–5.2 percent points). In girls, overweight (WHO and IOTF) remained stable independently of parental educational attainment. The prevalence of obesity (WHO) only decreased in boys with parents that had university degrees (–3.3 percent points), but this trend was not observed applying the IOTF criteria. In girls, there were no differences in the prevalence of obesity (WHO and IOTF) based on parental educational attainment. There were also no differences in the prevalence of obesity in either sex or based on parental educational attainment (Appendix B Supplemental Table A4).
Discussion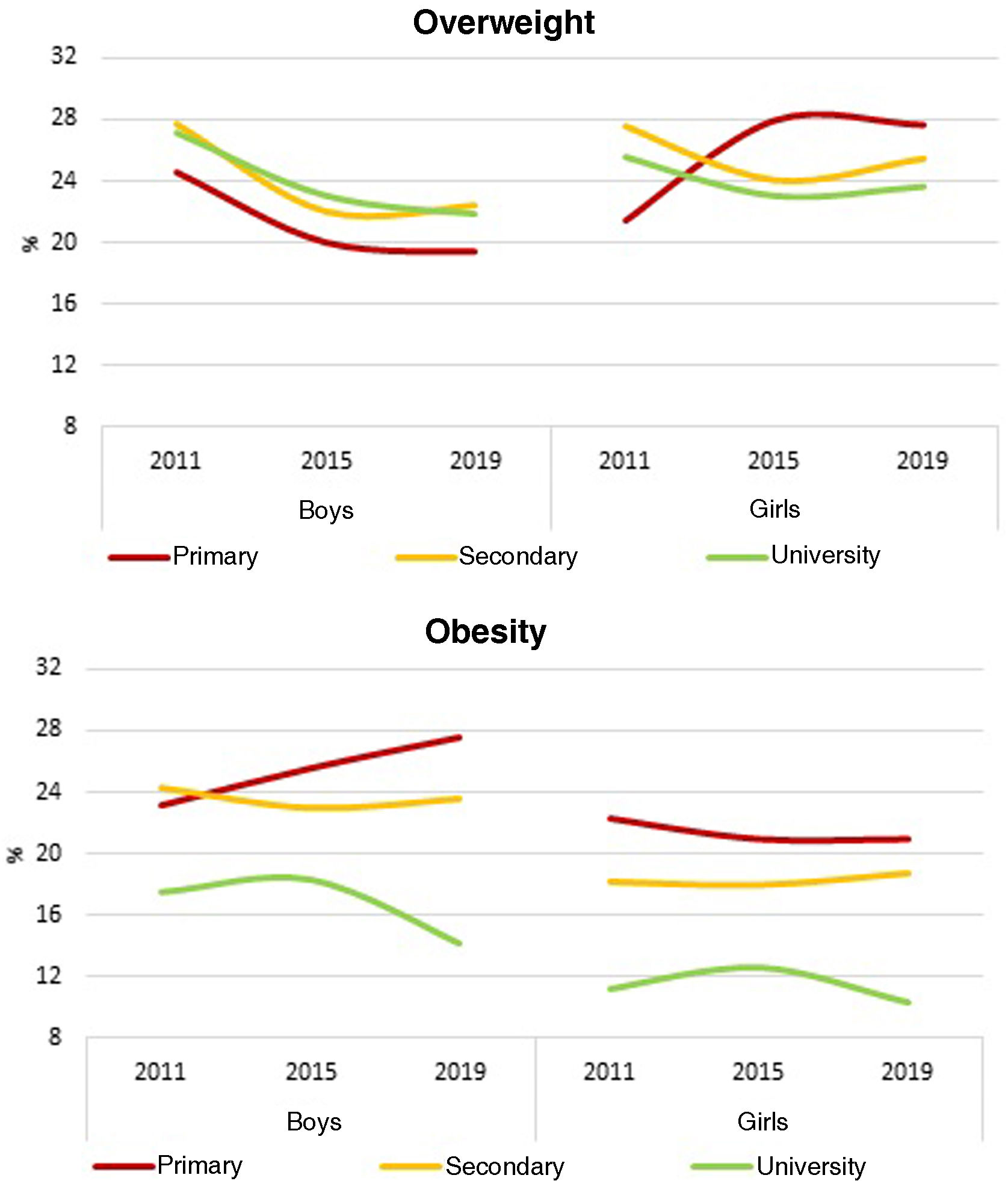
This study analyses the temporal trends in overweight, obesity and central obesity in a large and representative sample of schoolchildren aged 6–9 years in the 2011–2019 period in Spain based on objective anthropometric measurements. The trends were not homogeneous, as there were differences based on sex, age and socioeconomic variables. Between 2011 and 2019, there was only a decrease in the prevalence of overweight in boys aged 6, 7 and 8 years whose parents had university degrees. There were no changes in the prevalence of obesity or central obesity in boys and in any of the conditions (overweight, obesity, central obesity) in girls.
The disparities in overweight and obesity trends could be due, on one hand, to the association of obesity with socioeconomic status, a determinant that is difficult to modify.5 On the other hand, overweight is a lesser accumulation of body fat and is therefore easier to correct.
Different studies have evinced a stabilization in the prevalence trends of childhood overweight and obesity in Spain and other European countries,12,21 although a recent meta-analysis found an increase in Spain.13 However, a study conducted in the framework of the COSI initiative found a reduction in the prevalence of overweight in children of both sexes in countries in southern Europe, included Spain, in line with our findings, as well as in the prevalence of obesity, whereas the prevalence of both seemed to have stabilized in northern Europe.22
One of the relevant findings was the difference based on sex in the overweight prevalence trends, as overweight went from being more prevalent in boys in 2011 to being more prevalent in girls from 2015 onward, despite the latter not having increased, while obesity remained more prevalent in boys throughout the study period. The shift was due to the decrease in the prevalence of overweight in boys between 2011 and 2019, which did not take place in girls. These trends are similar to those observed in countries like Italy,23 while in Portugal significant decreases in excess weight were limited to girls.24 On the other hand, a study conducted in Catalonia, Spain, between 2006 and 2016 found a decrease in excess weight in both sexes, although the sampling and measurement methods differed from those of our study.25 It is known that the level of physical activity tends to be different in boys and girls in Spain, where girls tend to be more sedentary and less physically active than boys.26 A possible explanation is that there may be a greater volume of sports activities and therefore easier access for boys.27 However, at present there is no evidence on changes in physical activity trends during this period that could justify the sex-based differences in overweight trends found in our study.
In our study, the prevalence of overweight and of obesity varied depending on the applied reference standard (WHO or IOTF), especially in obesity (greater with the WHO reference), as had been described in other studies.28 These discrepancies occur because each standard is based on a different population and on different cut-off points for identification of risk groups.29 These differences notwithstanding, the identified trends in obesity and overweight were consistent, showing a decrease in overweight and stabilization of obesity in boys and stabilization of both in girls. We also analysed trends in central obesity, and found a greater prevalence than the prevalence calculated with the WHO reference, although stable throughout the study period, which was consistent with the obesity prevalence trends based on both the WHO and IOTF standards.
The analysis by age showed that the decrease in the overweight trend occurred chiefly in younger children (6–8 years) but not in children aged 9 years. A study conducted in the region of Andalusia in schoolchildren aged 8–15 years also found a decrease in excess weight in younger children (8–13 years) between 2011 and 2015, chiefly on account of a reduction in overweight.30 In addition, recent rounds of the ALADINO study have found an improved weight status in boys aged 6 years compared to previous rounds, perhaps on account of population-wide strategies to improve lifestyle habits in Spain, such as the NAOS,7 that encompass a variety of initiatives to promote healthy eating and physical activity in addition to raising awareness in families.31 If this trend were to persist in subsequent rounds it would constitute a substantial change compared to the longitudinal trends found between 1985 and 2019 in a large-scale study in 200 countries analysing BMI for age, according to which the increase in the BMI relative to the WHO reference was largest in young boys and girls in Spain.32
As regards longitudinal trends in relation to socioeconomic level, we found a decrease in overweight and obesity restricted for the most part to children of parents with higher educational attainment. The inverse association between household socioeconomic level and the prevalence of childhood obesity and central obesity.30,33,34 However, a different study based on data reported by parents in the national health surveys from 1997 to 2017 found a decrease in obesity in boys with parents of low socioeconomic status combined with an increase in girls.35 In contrast, the study of longitudinal trends between 2006 and 2016 in Catalonia found an overall decrease in the prevalence of obesity, although in disadvantaged areas, defined based on the MEDEA deprivation index, the prevalence increased.25 In our study, the differences in longitudinal trends based on socioeconomic level were most evident when parental educational attainment was used as the indicator compared to household income, an indicator whose impact and correlation to the living standards of the family could have varied in the period under study, which spanned 9 years of economic crisis and post-crisis recovery in Spain. Although both indicators are essential in the study of inequalities, based on our results, parental educational attainment may offer a higher specificity for the assessment of differences based on socioeconomic status,36 as it may be more strongly associated with lifestyle habits.37
Although the decrease in overweight and the improved weight status of the youngest schoolchildren across ALADINO rounds seemingly warrant an optimistic forecast for the near future, we must underscore that the described trends reflect the situation before the COVID-19 pandemic, and future rounds will have to assess its actual impact, as there are studies38 and data from countries such as the United Kingdom39 indicating that weight status trends in schoolchildren have worsened following the pandemic.
Some of the strengths of our study are the homogeneity of the methodology and design of the three study rounds included in the analysis and the large sample size (more than 35 000 schoolchildren) that guarantees that the results are representative of the national population. On the other hand, the fact that objective data from anthropometric measurements were used, as opposed to data reported by parents, increases the reliability of the results. The fact that the results obtained using different widely used growth standards (WHO, IOTF) were congruent consistent supports the consistency of the findings. In addition, the longitudinal analysis of central obesity, conducted in few previous studies, provides a foundation from which to advance in the knowledge and interpretation of waist circumference and the waist-to-height ratio as additional parameters to assess weight status in school-aged children. Lastly, the comparative analysis based on socioeconomic factors made it possible to identify and describe gender and socioeconomic inequalities in childhood obesity trends.
Among the limitations of the analysis, we ought to highlight the use of data obtained through cross-sectional studies, which does not allow inferences about causality. In addition, since the sample was restricted to children aged 6–9 years, the results may not be representative of other age groups. Another limitation is that we did not consider other key factors such as dietary habits, physical activity or family awareness, which could have contributed to the absence of differences based on income in the longitudinal overweight trends.
ConclusionBetween 2011 and 2019, the prevalence of overweight decreased in boys aged 6–8 years and in boys whose parents had university degrees. The prevalence of overweight in boys continued to be greater in households where parents had university degrees, contrary to the trend observed in girls, and the prevalence of obesity was greater in households in which parents had completed primary education alone. In children of either sex from households with different socioeconomic status or aged 9 years, the prevalence of overweight and of obesity remained stable and unacceptably high.
These findings highlight the importance of implementing policies for monitoring and fighting childhood obesity that take into account the underlying gender and socioeconomic inequalities, which contribute to less favourable overweight and obesity trends in girls and in disadvantaged groups, applying inclusive approaches to mitigate these health inequities. Surveillance in upcoming ALADINO rounds will make it possible to establish the changes in these indicators following the COVID-19 pandemic.
FundingThe ALADINO study is funded by the Agencia Española de Seguridad Alimentaria y Nutrición (Spanish Agency of Food Safety and Nutrition), who carries out rounds of the study at regular intervals in the framework of the Child Obesity Surveillance Initiative of the WHO Regional Office for Europe.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following is Supplementary data to this article:

