






Congenital heart disease is a major cause of infant mortality in developed countries. In Spain, there are no publications at national level on mortality due to congenital heart disease. The aim of this study is to analyse mortality in infants with congenital heart disease, lethality of different types of congenital heart disease, and their variation over a 10-year period.
MethodsA retrospective observational study was performed to evaluate mortality rate of children under one year old with congenital heart disease, using the minimum basic data set, from 2003 to 2012. Mortality rate and relative risk of mortality were estimated by Poisson regression.
ResultsThere were 2,970 (4.58%) infant deaths in a population of 64,831 patients with congenital heart disease, with 73.8% of deaths occurring during first week of life. Infant mortality rate in patients with congenital heart disease was 6.23 per 10,000 live births, and remained constant during the 10-year period of the study, representing 18% of total infant mortality rate in Spain. The congenital heart diseases with highest mortality rates were hypoplastic left heart syndrome (41.4%), interruption of aortic arch (20%), and total anomalous pulmonary drainage (16.8%). Atrial septal defect (1%) and pulmonary stenosis (1.1%) showed the lowest mortality rate.
ConclusionsCongenital heart disease was a major cause of infant mortality with no variations during the study period. The proportion of infants who died in our study was similar to other similar countries. In spite of current medical advances, some forms of congenital heart disease show very high mortality rates.
Las cardiopatías congénitas suponen una de las principales causas de mortalidad infantil en países desarrollados. En España no hay publicaciones sobre mortalidad de las cardiopatías congénitas a nivel nacional. El objetivo del estudio es determinar la tasa de mortalidad infantil de las cardiopatías congénitas, así como la letalidad de las distintas cardiopatías, durante un periodo de 10 años.
Material y métodosEstudio observacional retrospectivo utilizando el conjunto mínimo básico de datos de 2003 a 2012 en niños ingresados con diagnóstico de cardiopatía congénita. Se realiza un análisis descriptivo de los pacientes y se calcula la tasa de mortalidad y los riesgos relativos de mortalidad mediante regresión de Poisson.
ResultadosFallecieron 2.970 menores de un año sobre una población de 64.831 pacientes con cardiopatías congénitas (4,58%). El 73,8% fallecieron la primera semana de vida. La tasa de mortalidad infantil en niños con cardiopatías congénitas fue de 6,23 por 10.000 nacidos vivos, cifra que se mantuvo constante a lo largo de los 10 años estudiados y que supone el 18% de la mortalidad infantil total. Las cardiopatías con mayor letalidad fueron el síndrome del corazón izquierdo hipoplásico (41,4%), la interrupción del arco aórtico (20%) y el drenaje venoso pulmonar anómalo total (16,8%), y las de menor letalidad la comunicación interauricular (1%) y la estenosis pulmonar (1,1%).
ConclusionesLas cardiopatías congénitas constituyen una causa importante de mortalidad infantil, que no ha presentado variaciones importantes durante el tiempo de estudio. La proporción de niños que fallecen es similar a la de los países de nuestro entorno. Pese a los actuales avances, algunas cardiopatías presentan letalidad elevada.
Congenital heart diseases are the most frequent type of congenital anomaly,1 with an estimated incidence of 8‰, and are associated with significant social and health care costs. The spectrum of congenital heart disease is broad, ranging from complex heart diseases that can cause death in early childhood to defects found by chance during adulthood. Despite advances in surgery and perioperative care, they remain the leading cause of death due to birth defects in infants2 and a leading cause of death in the paediatric population in developed countries.3–5 The mortality of congenital heart diseases varies based on the timing of the study and the level of care: a mortality among children of 4.14 per 10,000 live births has been reported in the United States,6 and of 4.73 per 10,000 live births in Europe.7
In Spain, studies have been conducted to assess the mortality associated with congenital heart diseases in the autonomous communities of Murcia8 and Navarre,9 but nationwide data are not yet available.
The aim of our study was to determine the mortality of congenital heart diseases in infants aged less than 1 year, the outcomes of these diseases, the differences in mortality based on the type of defect and their contribution to overall mortality in this age group.
Materials and methodsWe conducted a retrospective observational study by collecting data from the minimal basic dataset (MBDS) population health care register. The study period comprehended 10 years, with collection of data on patients discharged between January 1, 2003 and December 31, 2012 in all of Spain.
We obtained information from the Ministry of Health and Consumption on the hospital discharges recorded in the MBDS register of patients aged less than 1 year with a primary or secondary diagnosis of congenital heart disease, coded according to the International Classification of Diseases, Ninth revision, Clinical Modification (ICD-9-CM): 745 (bulbus cordis anomalies and anomalies of cardiac septal closure), 746 (other congenital anomalies of heart) or 747 (other congenital anomalies of circulatory system), which comprehend all the codes for congenital heart diseases.
We excluded cases with clinical conditions that may be physiological or with circulatory system anomalies that did not necessarily involve a congenital heart defect, such as patent ductus arteriosus in preterm newborns, single umbilical artery, heart block or unspecified congenital anomalies.
The diagnoses were coded with the ICD-9-CM system following the regulations established by the Technical Reference Unit for the ICD-9-CM of the National Health System of Spain.10
To assess mortality, we selected those cases where the patient died in the first year of life. To calculate rates, we used the birth data reported by the Instituto Nacional de Estadística (National Institute of Statistics) as the reference population.11
We performed a descriptive analysis of the patients. We have summarised qualitative variables as frequency distributions and compared them by means of the Chi-square test or, if the assumptions for this test were violated, the Fisher exact test. We calculated the infant mortality rate (MR) associated with congenital heart disease as the number of deaths in infants aged less than 12 months with a diagnosis of congenital heart disease per 10,000 live births in a given year. We calculated infant mortality by age group: early neonatal (0–7 days), late neonatal (8–28 days) and postneonatal (29–365 days). We analysed trends in mortality in comparison with the first year under study by means of the relative risk of mortality (RRM), calculated as the ratio between the mortality due to congenital heart diseases in 2003 and the same mortality in each of the other years under study (2004–2012). We also estimated the yearly RRM by Poisson regression with the corresponding 95% confidence interval (CI). We defined lethality as the percentage of children with congenital heart diseases that died, and calculated overall lethality overall and lethality by type of heart disease.
ResultsTemporal trends in mortality among children with congenital heart diseases and rate of mortalityThe number of infants aged less than 1 year diagnosed with congenital heart diseases according to the criteria defined in the study was 64,831 out of a cohort of 4,766,325 live newborns, with an incidence of 13.6‰. During the 10-year study period, 2,970 of these infants died, corresponding to a lethality of 4.58%.
Of the 2,970 patients that died, 2191 (73.8%) died in the first week post birth, 161 (5.4%) between 8 and 28 days post birth, and 618 (21.8%) between 29 days and 1 year post birth.
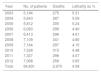
Table 1 shows the number of patients with congenital heart diseases, the number of deaths and the lethality rate (%) for each year.
Number of patients with congenital heart diseases, number of deaths and lethality per year.
| Year | No. of patients | Deaths | Lethality as % |
|---|---|---|---|
| 2003 | 5,184 | 275 | 5.31 |
| 2004 | 5,643 | 287 | 5.09 |
| 2005 | 5,812 | 305 | 5.24 |
| 2006 | 6,083 | 298 | 4.90 |
| 2007 | 6,413 | 296 | 4.61 |
| 2008 | 7,109 | 341 | 4.80 |
| 2009 | 7,164 | 297 | 4.15 |
| 2010 | 7,028 | 315 | 4.48 |
| 2011 | 7,327 | 298 | 4.07 |
| 2012 | 7,068 | 258 | 3.65 |
| Total | 64,831 | 2,970 | 4.58 |
Lethality: percentage of children with congenital heart diseases that died.
We found a decreasing trend in the proportion of deaths during the 10 years under study, with lethality decreasing from 5.31% in 2003 to 3.65% in 2012, although the absolute frequency of deaths remained within a narrow range save for a slight descent in the last year. During the period under study, there was a progressive increase in the number of patients and of cases of congenital heart disease. This increase was mainly due to an increase in the number of diagnosed cases of atrial septal defect (ASD), corresponding to ICD-9-CM code 745.5.
Fig. 1 shows the evolution of the absolute frequencies of cases of congenital heart disease overall, ASD, and congenital heart disease excluding ASD.

Thus, while the cases of congenital heart disease grew from 7898 in 2003 to 10,202 in 2012 (an increase of 22.6%), newly diagnosed cases of ASD increased from 1941 in 2003 to 3865 in 2012 (an increase of 49.87%).
Temporal trends in mortality in children with congenital heart diseasesDuring the period under study, the MR of patients with congenital heart defects in Spain was 6.22 patients per 10,000 live births.
Fig. 2 shows the MR overall and by sex for each year under study.

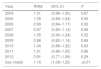
When we compared the yearly MR in children with congenital heart diseases with the baseline MR in 2003, we found no statistically significant differences. However, the analysis of mortality by sex showed that the risk of dying was 16% greater in male infants compared to female infants (RRM, 1.16; 95% CI, 1.08–1.25), and this difference was statistically significant (P<0.001) (Table 2).
Relative risks of mortality for each year (mortality in each year under study, starting in the second year, divided by the mortality in 2003).
| Year | RRM | 95% CI | P |
|---|---|---|---|
| 2004 | 1.01 | (0.86–1.20) | 0.87 |
| 2005 | 1.05 | (0.89–1.24) | 0.55 |
| 2006 | 0.99 | (0.84–1.17) | 0.92 |
| 2007 | 0.97 | (0.82–1.14) | 0.68 |
| 2008 | 1.05 | (0.90–1.24) | 0.52 |
| 2009 | 0.96 | (0.82–1.14) | 0.66 |
| 2010 | 1.04 | (0.88–1.22) | 0.63 |
| 2011 | 1.01 | (0.86–1.20) | 0.86 |
| 2012 | 0.91 | (0.77–1.08) | 0.29 |
| Sex (male) | 1.16 | (1.08–1.25) | <0.01 |
CI, confidence interval; RRM, relative risk of mortality.
Table 3 shows the overall number of births and overall MR in infants, the MR in patients with congenital heart diseases, and the percentage of infant deaths in each group for each year under study.
Infant mortality of all causes and due to congenital heart disease.
| Year | Births in Spaina | Deaths in <1 yeara | Infant MRb | Deaths in <1 year with CHD | % deaths in <1 year with CHD | MRb infants with CHD |
|---|---|---|---|---|---|---|
| 2003 | 441,881 | 1,733 | 39.22 | 275 | 15.87 | 6.22 |
| 2004 | 454,591 | 1,813 | 39.88 | 287 | 15.83 | 6.31 |
| 2005 | 466,371 | 1,765 | 37.85 | 305 | 17.28 | 6.54 |
| 2006 | 482,957 | 1,704 | 35.28 | 298 | 17.49 | 6.17 |
| 2007 | 492,527 | 1,704 | 34.60 | 296 | 17.37 | 6.01 |
| 2008 | 519,779 | 1,741 | 33.50 | 341 | 19.59 | 6.56 |
| 2009 | 494,997 | 1,609 | 32.51 | 297 | 18.46 | 6.00 |
| 2010 | 486,575 | 1,553 | 31.92 | 315 | 20.28 | 6.47 |
| 2011 | 471,999 | 1,505 | 31.89 | 298 | 19.80 | 6.31 |
| 2012 | 454,648 | 1,404 | 30.88 | 258 | 18.38 | 5.67 |
<1 year, infants aged less than 1 year; CHD, congenital heart disease; MR, mortality rate.
Source: Fenómenos demográficos. Movimiento Natural de la Población. Estadística de Nacimientos Instituto Nacional de Estadística. Available at: http://www.ine.es/.
Although there was a decreasing trend in the infant MR in the 10 years under study, we found that the contribution of congenital heart diseases to overall mortality was of 18% on average, with an increasing trend, as it grew from 15.87% in 2003 to 18.87% in 2012.
Lethality by type of heart diseaseWe calculated the percentage of deaths due to each type of congenital heart disease (lethality) when the disease presented in isolation and when it presented in association with other heart diseases.
Table 4 shows the diseases with the highest lethality. Hypoplastic left heart syndrome (HLHS) was the most lethal disease, followed by interrupted aortic arch.
Congenital heart diseases with the highest lethality.a Number of cases (N) and percentage of deaths for each disease in isolation and in association to other heart diseases.
| ICD-9-CM code | Congenital heart disease | n | % deaths, isolated disease | % deaths, associated with other diseases |
|---|---|---|---|---|
| 746.7 | Hypoplastic left heart syndrome | 614 | 41.4 | 48.4 |
| 747.11 | Interrupted aortic arch | 207 | 20.0 | 34.5 |
| 747.41 | Total anomalous pulmonary venous connection | 394 | 16.8 | 23.2 |
| 746.01 | Pulmonary atresia | 442 | 14.3 | 22.0 |
| 746.2 | Ebstein anomaly | 223 | 12.4 | 25.4 |
| 745.3 | Common ventricle | 380 | 8.0 | 23.1 |
| 746.5 | Congenital mitral stenosis | 257 | 5.6 | 25.4 |
ICD-9-CM, International Classification of Diseases, Ninth Edition, Clinical Modification; n, absolute frequency of cases.
The least lethal isolated congenital heart diseases were ASD, pulmonary valve stenosis and ventricular septal defect.
Table 5 shows the proportion of deaths corresponding to the most frequent congenital heart diseases, in isolation and in association to other heart diseases.
Lethalitya of the most frequent heart diseases. Absolute frequency (n) of deaths and percentage of deaths when the defect occurred in isolation and when it appeared in association with other heart diseases.
| ICD-9-CM code | Congenital heart disease | n | % deaths, isolated disease | % deaths, associated with other diseases |
|---|---|---|---|---|
| 745.5 | Atrial septal defect | 30,059 | 1.0 | 4.8 |
| 745.4 | Ventricular septal defect | 16,573 | 1.2 | 7.3 |
| 747.0 | Patent ductus arteriosus | 12,893 | 2.7 | 7.1 |
| 747.10 | Coarctation of the aorta | 2,619 | 4.5 | 13.0 |
| 746.02 | Pulmonary valve stenosis | 2,378 | 1.1 | 4.6 |
| 745.1 | Transposition of the great vessels | 2,356 | 10.2 | 16.5 |
| 745.6 | Endocardial cushion defects | 2,152 | 7.1 | 13.8 |
| 745.2 | Tetralogy of Fallot | 1,931 | 6.3 | 11.8 |
| 745.0 | Common truncus | 820 | 11.4 | 12.3 |
ICD-9-CM, International Classification of Diseases, Ninth Edition, Clinical Modification.
When we analysed the risk of death by the number of associated heart diseases, we found a statistically significant association between the number of deaths and the number of associated heart diseases, with lethality increasing with the number of associated heart diseases (P<0.001) (Table 6).
DiscussionIn this study, we assessed the mortality of infants admitted to hospital and discharged due to death with a diagnostic code for congenital heart disease in the discharge summary. Any comparison of the data on mortality due to congenital heart diseases reported in the literature must take into account the medical and surgical care available in the geographical area and time that studies were conducted. Tellingly, the lowest mortality rates are found in the most recent reports from Western countries. In 2009, Moons et al.12 reported a 4% lethality in infants aged less than 1 year born in Belgium in 2002 with congenital heart diseases, and Dilber and Malcic13 reported a lethality of 3.8% in Croatian children in 2010. In 2012, Khoshnood et al.7 published a population-based cohort study of French infants born between 2005 and 2008 with congenital heart disease diagnosed at age up to 1 year, and reported a lethality of 6.4%.
The proportion of deaths, or lethality, in our study (4.58%) was similar to the proportions reported in neighbouring countries taking into account differences in methodology. Thus, the 4% lethality in the study of Moons et al.12 corresponded to a 5-year follow-up period (although most patients died in the first 6 months of life), while our study only covered the first year of life and did not reflect any deaths that may have occurred at a later point.
In Spain, Guía et al. carried out a study, which cannot be compared to ours due to the distance in time, with a retrospective analysis of the 1978–1983 and 1984–1990 periods to compare the outcomes of congenital heart disease cases in a tertiary referral hospital in the autonomous community of Murcia.8 The study found that lethality decreased between the 2 periods from 28% to 21.7%. This decreasing trend is well established in the literature and is attributed to improvements in the diagnosis and management of congenital heart diseases.6
The 4.58% lethality found in our study was significantly lower than the one reported by Martínez Olorón et al.9 in a study conducted in Navarre between 1989 and 1998 and published in 2005. That study analysed a cohort of 47,783 infants in which 428 received diagnoses of congenital heart disease (incidence, 8.96‰), and found a lethality of 10% during the followup, which lasted between 5 and 14 years. We cannot compare our data to these findings due to differences in the methods used to collect the data and in the duration of followup.
During the 10 years under study, we found a decreasing trend in the percentage of infants with congenital heart disease that died. Thus, the proportion of infants that died in the first year of life decreased from 5.3% (2003) to 3.7% (2012), and the probability of dying in 2012 was 9% lower compared to 2003. However, and given that mortality depends both on the incidence of disease and the associated lethality rate, it is important that we analyse changes in either or both components and their impact in mortality. Recent studies14 have described an increase in the incidence of congenital heart diseases attributable to increases in mild diseases with a low lethality, while the incidence of severe defects remained stable.
In our study, we observed a significant increase in the detection of ASD cases in the last years. This increase is probably due to multiple factors. One of them may be the increasing availability of paediatric cardiologists and ultrasound technicians in health care facilities that offer maternity services, and the growing practice of performing an ultrasound examination of all newborns with nonspecific heart murmurs in the first days post birth and before discharge from hospital. In this population, small ASDs can be detected incidentally, and while a significant proportion of them close spontaneously before age 2 years, this may lead to overestimation of the incidence of ASD due to the code appearing in the discharge summary. Another reason may be the ICD-9-CM coding system in itself, as code 745.5, “ostium secundum type atrial septal defect” includes patent foramen ovale. That is, ostium secundum type ASD is coded the same as patent foramen ovale (code 745.5). The foramen ovale usually closes soon after birth, although in some cases functional closure may delay, with transient detection of a small interatrial shunt on colour Doppler. Thus, cases of patent foramen ovale where patients receive the diagnosis in the first days of life may be counted as ASDs.
Some authors have suggested that this increase in the incidence of mild congenital heart diseases may be due to advances in diagnostic methods and the implementation of screening programmes leading to increased detection, rather than an increase in the actual frequency of disease.15
Since the lethality of ASD is very low, the increase in the proportion of this particular disease in the group of congenital heart diseases may have contributed to the overall decrease in lethality.
Male infants were at increased risk of dying, a difference that was statistically significant. This finding may be due to the higher prevalence of severe and very severe heart defects in male newborns compared to the higher prevalence of milder forms in female newborns described in the literature.16
When we compared mortality in the early neonatal, late neonatal and postneonatal periods, we found that the highest mortality occurred in the early neonatal period, that is, in the first 7 days of life. In the study by Khoshnood et al. that we already mentioned,7 neonatal mortality made up 60% of infant deaths. In our study, it amounted to 79%: most deaths clustered in the first week of life. This finding may have been influenced by other comorbidities that were not taken into account in our analysis, such as preterm birth or the presence of additional malformations.
In the analysis by type of heart defect, we found that HLHS and interrupted aortic arch corresponded to the highest lethality, and ASD to the lowest. When we compared lethality by type of defect in recent years, we found a striking improvement in survival. Thus, the study by Guía et al.8 cited above found a 100% lethality for HLHS compared to 41.4% in our study, and a lethality of 85.7% for total anomalous pulmonary venous connection compared to 16.8% in our study, differences that probably reflect technical advances and improvements in perioperative care in recent years.
When it came to studies comparable to ours, such as the one conducted by Moons et al.,12 we found that the lethality found in our population was similar when it came to very severe congenital heart defects, such as HLHS (50% in Moons study vs 41.4% in our study) and lower when it came to moderate defects, such as tetralogy of Fallot (17% in Moons study vs 6.3% in our study).
We found an overall infant MR in patients hospitalised with congenital heart diseases of 6.23 per 10,000 live births, higher than the rates reported in the literature; however, comparisons are limited by methodological constraints.
Thus, Gilboa et al.6 found an infant MR of 4.14 per 10,000 live births based on the death certificates filed in the United States in the 1999–2006 period. Their results may have been affected by the accuracy and thoroughness of the information included in the certificates; one of the main limitations of their study was the very source of the data, which is frequently imprecise, as in 34% of cases, the cause of death was recorded as unspecified congenital heart defect.
In a significant number of cases in our study, congenital heart diseases may have been the immediate cause of death, but in other cases they may have only contributed to it, which would represent a death associated with heart disease. This uncertainty could only be resolved by analysing the death certificates of every patient, assuming they were all filed with absolute scientific rigour, entering the underlying disease as the immediate cause of death and associated diseases as significant conditions that contributed to the death, but we did not have access to this information.
In a cohort of 111,225 children born in 2002 in Belgium, Moons et al.12 found 921 children with congenital heart diseases and a lethality of 4%, which corresponds to a MR of 3.3 per 10,000 live births, lower than the one found in our study. This may be partly due to the small sample size in the Belgian study (37 deaths). In France, Khoshnood et al.7 found an infant MR of 4.73 per 10,000 live births.
It is worth noting that the MR associated to congenital heart diseases remained all but constant through the 10 years under study, save in 2012, when there was a slight decline.
Of all the infants aged less than 1 year that died in Spain in the 10 years under study, an average of 18% had congenital heart diseases. This proportion showed an increasing trend: it grew from 15.87% in 2003 to 18.87% in 2012.
Since we found a decreasing trend in infant mortality of all causes in the period under study (1,733 deaths per 10,000 live births [39.22%] in 2003 vs 1,404 deaths per 10,000 live births [30.88] in 2012), the decrease was probably not due to a decrease in mortality related to heart disease, but rather in mortality due to other causes in infants aged less than 1 year.
However, we must take into account that our study did not assess the presence of comorbidities with a potential impact on mortality, such as other congenital malformations.
LimitationsOne of the limitations of using the MBDS for clinical studies is that the data is obtained from medical records, so that there is variability in the documentation based on the thoroughness of the reporting physician and the skill of the medical coder. Congenital heart diseases constitute a broad spectrum of anomalies with wide variability in anatomical features, severity, and clinical and surgical implications. The specificity of the ICD-9-CM codes for congenital heart diseases may pose challenges to clinicians as well as medical coders.
Our study did not include data on foetal death due to severe cardiac defects or voluntary termination of pregnancy due to a cardiac malformation in the foetus.
The study analysed the 2003–2012, so its results may not be representative of the current situation.
Conclusions- 1.
The proportion of infants with congenital heart diseases that died in our study was within the range reported by neighbouring countries. Most of these patients died in the first week of life.
- 2.
Congenital heart diseases are a significant cause of death in infants, with an increased risk of dying in the male sex.
- 3.
The reduction in the overall infant mortality observed during the period under study did not seem to be due to a decrease in congenital heart disease mortality.
- 4.
Despite advances in care and surgical technique, the lethality of some heart diseases continues to be high.
The authors have no conflicts of interest to declare.
Please cite this article as: Picarzo JP, González MM, Zamalloa PL, Marcos DC. Mortalidad de las cardiopatías congénitas en España durante 10 años (2003-2012). An Pediatr (Barc). 2018;88:273–279.
