


A male infant aged 9 months was brought to the emergency department with irritability, food refusal and fluctuating level of consciousness. The physical examination revealed irritability, a tense fontanel and nuchal rigidity.
The transfontanellar ultrasound examination revealed a voluminous anechoic multiseptated lesion with contralateral midline shift (Fig. 1A). This finding prompted additional imaging of the brain with CT and MRI (Fig. 1B–D). These tests allowed visualization of a hypodense multiseptated lesion in the left frontoparietal region with a mass effect on the left lateral ventricle resulting in midline shift and the obliteration of the suprasellar and perimesencephalic cisterns with signs of subfalcine and descending transtentorial herniation.

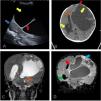
(A) Transfontanellar ultrasound with a 5–8MHzmicro-convex array transducer (sagittal plane) showing an anechoic lesion (yellow arrow), multiseptated (red arrow), with a cystic appearance, compressing the adjacent cerebellar parenchyma (blue arrow). (B) CT scan, axial view, showing a supratentorial multiseptated lesion with a large cystic component (yellow arrow). It exerted a mass effect on the metopic suture, which was bulging (red arrow), with midline shift (brown arrow), dilatation of the temporal and occipital horns of the right lateral ventricle (green arrow) and transependymal oedema secondary to hydrocephalus. (C) T2-weighted MRI of the brainstem, coronal plane, evincing descending transtentorial herniation (brown arrow). (D) Gadolinium-enhanced FLAIR MRI of the brainstem, coronal plane, showing a large cystic lesion with an enhanced peripheral solid component (blue arrow), midline shift (brown arrow) and ventricular dilatation with transependymal oedema (green arrow).
The patient underwent surgery and the histological examination of the specimen yielded the diagnosis of desmoplastic infantile ganglioglioma.
Desmoplastic infantile ganglioglioma is a low-grade mixed neuronal-glial tumour that usually appears between 1.5 and 18 months post birth.1 It is usually located in the supratentorial region and involves more than one cerebral lobe, most frequently the parietal and frontal lobes.2 Radiologically, it has a characteristic appearance, presenting as a large supratentorial mass with mixed cystic and solid components and predominance of the cystic component. The clinical signs include an increase in head circumference and bulging of the anterior fontanelle. It is treated surgically, and the prognosis is good after full resection of the tumour.3
