

We present the case of a male infant aged 10 months brought to the emergency department with fever and abdominal pain of 3 days’ duration. The salient findings of the physical examination were jaundice, abdominal distension with prominent superficial venous collateralization and hypoventilation in the right hemithorax.
The evaluation included a thoracic radiograph (Fig. 1) that evinced pleural effusion and mediastinal shift and a blood panel that detected conjugated hyperbilirubinemia and transaminase elevation.

The workup was completed with ultrasound and CT scans that evinced the presence of right diaphragmatic hernia (RDH) with incarceration of the right lobe (RL) of the liver and ascites, dilation of the biliary tract and collapse of the hepatic veins and suprarenal inferior vena cava with collateral venous circulation (Fig. 2).

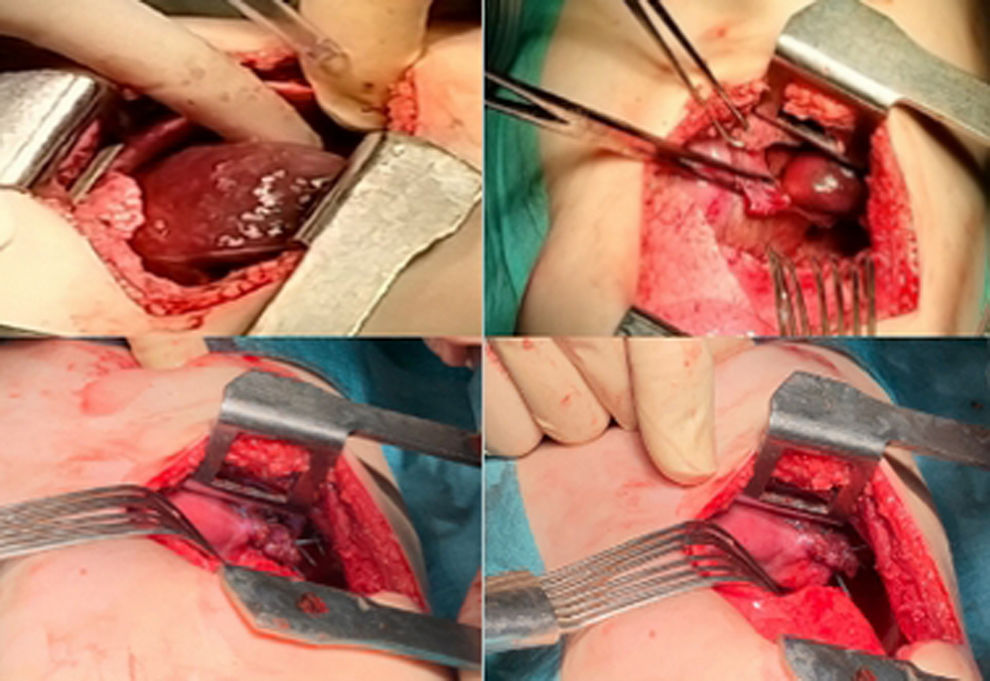
The patient underwent urgent surgery via right thoracotomy, which required extension of the diaphragmatic defect to reduce the incarcerated RL followed by primary closure of the hernia with nonabsorbable sutures (Fig. 3).
. Enlargement of defect (top right). Suturing of the hernia (bottom).")
The patient did not experience any postoperative complications, and venous patency was verified in the ultrasound examination performed at 1 month post surgery, with full normalization of transaminase levels 3 months after the procedure.
Budd-Chiari syndrome is characterized by the obstruction of hepatic vein flow and can be due to multiple causes, chief of which are thrombosis or extrinsic venous compression, and is rarely secondary to RDH incarceration.1,2

