





Pseudohypoparathyroidism (PHP) is a spectrum of diseases characterized by insensitivity of target tissues to the action of parathyroid hormone and, consequently, by the presence of hyperphosphatemia and hypocalcaemia of varying severity. Early-onset obesity is a feature of PHP type 1A.
This article discusses the need to establish uniform criteria to guide the nutritional management of patients with PHP. A decrease in energy expenditure calls for an adjustment of the energy content of the diet. Reducing the intake of foods rich in inorganic phosphorus helps to manage hyperphosphataemia. Targeted nutrition should be part of the treatment plan of children and adolescents with PHP, since it contributes to modulating the calcium and phosphorus metabolism imbalances characteristic of these patients.
El seudohipoparatiroidismo (PHP) incluye entidades caracterizadas por la ausencia de respuesta tisular a la acción de la hormona paratiroidea y, en consecuencia, la presencia de hiperfosfatemia e hipocalcemia en grado variable. La obesidad de inicio temprano es una característica de los pacientes con PHP1A.
Este artículo plantea la necesidad de establecer unos criterios comunes que orienten el manejo nutricional de estos pacientes. La disminución de su gasto energético implica adaptar el contenido calórico de su alimentación. Reducir el consumo de alimentos ricos en fósforo inorgánico ayuda a manejar la hiperfosfatemia. El consejo nutricional dirigido debe formar parte de la estrategia terapéutica de los niños y adolescentes con PHP, ya que contribuye a modular los desequilibrios en el metabolismo fosfocálcico característicos de estos pacientes.
The term pseudohypoparathyroidism (PHP) (catalogued as OMIM#103580 for PHP type 1A [PHP1A], OMIM#603233 for PHP type 1B [PHP1B] and OMIM#612462 for PHP type 1C [PHP1C]) encompasses a group of rare diseases characterised by end-organ resistance to the action of parathyroid hormone (PTH). They generally share the presence of (epi)genetic abnormalities at the GNAS locus, whose main product is the α subunit of the stimulatory G protein (Gs). Defects in Gsα cause changes in the signalling pathway from the Gsα-coupled receptor to the intracellular environment, thus compromising different physiological actions. A new classification system terms these forms of PHP as iPPSD2, if there are genetic changes, and iPPSD3 if there are changes in methylation.1
Affected patients develop hyperphosphataemia and hypocalcaemia along with elevation of PTH. These features may be associated with a phenotype (Albright hereditary osteodystrophy) characterised by short stature, a round face, short neck, brachydactyly and ectopic ossifications.2
The management includes specific nutritional treatment to contribute to the modulation of the biochemical abnormalities characteristic of the disease and the regulation of energy metabolism. Thus, an evidence-based guideline is needed to establish the nutritional recommendations to be conveyed to patients and the caregivers of children with PHP.
Energy balanceThe α subunit of the Gs protein is involved in the transmission of signals from the melanocortin 4 receptor (MC4R) in the cells of the dorsomedial hypothalamus, and is part of the pathways that regulate energy expenditure and appetite.3 Reduced activity in this protein results in a positive energy balance due to a decrease in the basal energy expenditure4–6 and in dietary thermogenesis.1
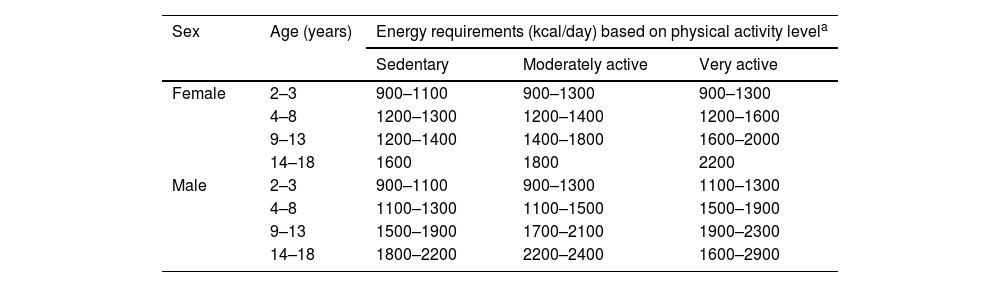
Weight gain starts early and is most pronounced during childhood and adolescence.2,7 Thus, ongoing nutritional management must be initiated early by restricting energy intake.8 Generally, when it comes to dietary intake, a reduction of 10% in the calculation of the basal energy expenditure for age and sex in the general population is recommended, as noted in Table 1.9 However, nutritional management must always be individualised, taking into account the characteristics of the patient and avoiding potential negative effects on growth and development.
Energy requirements based on age, sex and level of physical activity.
| Sex | Age (years) | Energy requirements (kcal/day) based on physical activity levela | ||
|---|---|---|---|---|
| Sedentary | Moderately active | Very active | ||
| Female | 2–3 | 900–1100 | 900–1300 | 900–1300 |
| 4–8 | 1200–1300 | 1200–1400 | 1200–1600 | |
| 9–13 | 1200–1400 | 1400–1800 | 1600–2000 | |
| 14–18 | 1600 | 1800 | 2200 | |
| Male | 2–3 | 900–1100 | 900–1300 | 1100–1300 |
| 4–8 | 1100–1300 | 1100–1500 | 1500–1900 | |
| 9–13 | 1500–1900 | 1700–2100 | 1900–2300 | |
| 14–18 | 1800–2200 | 2200–2400 | 1600–2900 | |
Adapted from: Palomo Atance et al.9
Recommendations for physical activity must be tailored to the body composition and fitness level of the individual child to facilitate adherence, increasing the level of activity as both of these aspects improve. The goal is to have the patient engage in moderate to vigorous physical activity for a minimum of 60 min a day, which can be divided in 2 or more sessions.10
MacronutrientsCarbohydratesChildren with PHP1A experience impairment of oral glucose tolerance, which may precede obesity11 and has been associated with loss of function of the Gsα protein in cells that express the MC4R receptor.3
As a general rule, carbohydrates must be part of the daily diet, contributing 50% of the daily energy intake. Intake of complex carbohydrates with a low glycaemic index should predominate.9 Consumption of 4–6 servings of cereal a day is recommended (bread, pasta, rice, flour), and, in this particular group of patients, reducing the intake of whole-grain cereals with a high phosphorus content.12 The diet should include at least 2 servings of vegetables and at least 3 servings of fruit per day.9 Dairy intake should limited to 2 or at most 3 servings a day, with a predominance of low-fat or fat-free products to control energy intake and provide a dietary source of calcium without an excessive amount of phosphorus.13
LipidsLipids will contribute 30% of the total energy intake, limiting saturated fats to 7%–10% of the total calories and cholesterol intake to 300 mg/day. The diet should include foods containing monosaturated and polyunsaturated fatty acids, avoiding consumption of trans fats (chiefly found in processed and precooked products) and reducing the intake of saturated fatty acids (butter, fatty meats, cold meats, palm and coconut oil). Olive oil should be used for cooking and for dressing raw foods.9
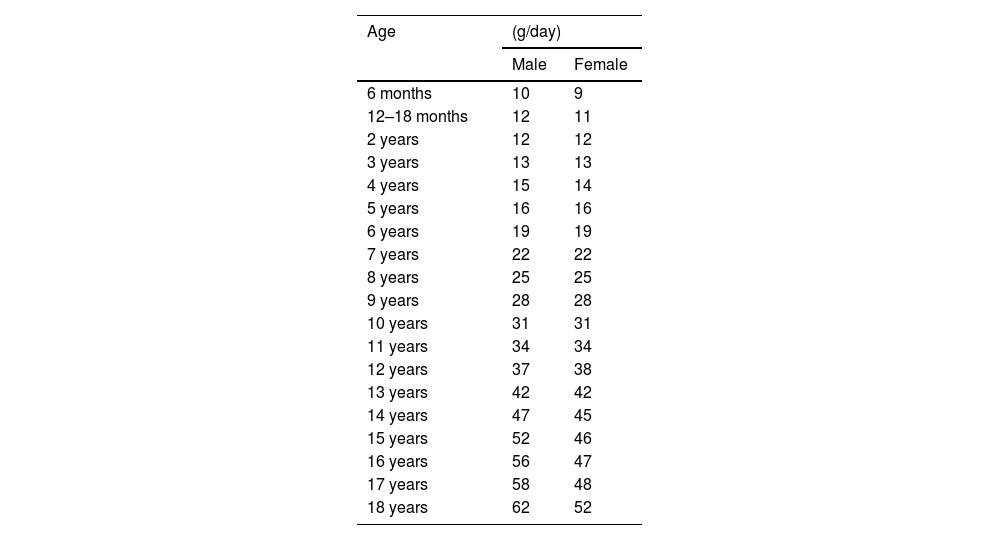
ProteinProtein intake should be limited to the protein requirements for age, which are listed in Table 2.14
Recommended daily protein intake, adapted from reference ranges.
| Age | (g/day) | |
|---|---|---|
| Male | Female | |
| 6 months | 10 | 9 |
| 12–18 months | 12 | 11 |
| 2 years | 12 | 12 |
| 3 years | 13 | 13 |
| 4 years | 15 | 14 |
| 5 years | 16 | 16 |
| 6 years | 19 | 19 |
| 7 years | 22 | 22 |
| 8 years | 25 | 25 |
| 9 years | 28 | 28 |
| 10 years | 31 | 31 |
| 11 years | 34 | 34 |
| 12 years | 37 | 38 |
| 13 years | 42 | 42 |
| 14 years | 47 | 45 |
| 15 years | 52 | 46 |
| 16 years | 56 | 47 |
| 17 years | 58 | 48 |
| 18 years | 62 | 52 |
Adapted from: EFSA Panel on Dietetic Products, Nutrition and Allergies.14
It is important to take into account that an excessive intake of protein, especially from animal sources, increases the urinary elimination of calcium and therefore the risk of kidney stones,15 in addition to being a significant source of phosphate.
FibreFibre is found in food in two forms: soluble and insoluble. Soluble fibre can be fermented by the gut microbiota, and its main sources are fruit, cereals (barley and oats) and legumes. Nonfermentable insoluble fibre is mainly found in wheat, rice and rye brans and in vegetables.16 The diet of children with PHP must contain soluble and insoluble fibre at a ratio of 1:3, taking into account that this ratio must be modified to increase the proportion of soluble fibre with decreasing age.17 The recommended daily fibre intake for children aged less than 2 years is 9 g. From this age, it can be calculated by adding 5 to the age of the child; for example, the recommended daily intake for a child aged 5 years would be of 10–15 g.17 It is worth noting that dietary fibre reduces the bioavailability of calcium, so in children with PHP, fibre intake must be adjusted for age and to the clinical condition of the patient. Supplemental Table 1S (Appendix B) presents the main dietary sources of soluble and insoluble fibre.12
MicronutrientsCalciumThe approach to the management of PTH resistance and hypocalcaemia present in some children with PHP includes initiation of treatment vitamin D analogues/active metabolites and oral calcium supplementation, depending on the dietary intake.2 In addition, the daily diet must include foods rich in calcium such as dairy products, legumes and fish. However, dietary calcium intake may decrease due to the restriction of foods rich in phosphorus, most of which also have a high calcium content. It is also important to remember that foods containing large amounts of oxalic acid (like spinach, chard or beets), phytic acid (cereal grains), dietary fibre, caffeine, tannins (tea and cocoa) and sodium reduce the bioavailability of calcium, so their consumption must be limited.
Calcium intake should not exceed the recommended allowance for age18 (Table 3), as excess calcium may interfere with the absorption of iron, zinc and other minerals, in addition to causing hypercalciuria and kidney stones.
Recommended daily calcium intake by age.
| Age | Calcium (mg/day) |
|---|---|
| 7–12 months | 280 |
| 1–3 years | 450 |
| 4–10 years | 800 |
| 11–17 years | 1.150 |
Developed based on the reference values published by the EFSA Panel on Dietetic Products, Nutrition and Allergies.18
Supplemental Table 2S (Appendix B) presents the main dietary sources of calcium.12
PhosphorusLimiting the dietary intake of phosphorus is one of the core interventions in the nutritional management of children with PHP. Phosphorus is found in food in 2 forms: organic and inorganic.
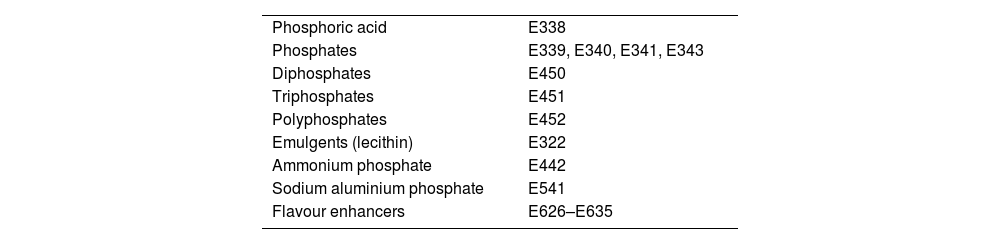
Inorganic phosphorus is found in the additives used to process foods.19 This has a substantial impact on blood phosphate levels, as nearly 90%–100% of ingested inorganic phosphorus is absorbed. Products rich in inorganic phosphorus must be eliminated from the diet, so it is important to educate families so they can identify additives rich in phosphorus in food labels20 (Table 4). In general, frozen, precooked or instant food products, processed cheeses, cold meats, industrial baked goods, sausages, breakfast cereals and sugary carbonated drinks contain large amounts of inorganic phosphorus.
Food additives containing phosphorus.
| Phosphoric acid | E338 |
| Phosphates | E339, E340, E341, E343 |
| Diphosphates | E450 |
| Triphosphates | E451 |
| Polyphosphates | E452 |
| Emulgents (lecithin) | E322 |
| Ammonium phosphate | E442 |
| Sodium aluminium phosphate | E541 |
| Flavour enhancers | E626–E635 |
Adapted from Lou-Arnal et al.20
Organic phosphorus is naturally present in animal protein (meat, fish, eggs, dairy) and plant protein (legumes and beans, seeds and nuts). It has a lesser impact on blood phosphate levels because only 30%–60% of the amount consumed is absorbed. Animal protein must be part of the daily diet due to its high biological value, but it is important to consider that the bioavailability of organic phosphorus is greater in animal protein sources than in plant protein. Consumption of fowl and lean pork or beef, egg white and dairy is recommended, never exceeding the recommended protein allowance for age. On the other hand, processed, precooked or cured meats must be completely eliminated from the diet. Current regulations do not require labels to reflect the amount of phosphorus added during processing, so the total phosphorus content of these foods, and the amount of inorganic phosphorus in particular, may be much higher than stated in the product label or in nutritional databases for that given food.19,20
Fish contain variable amount of phosphorus with a high bioavailability. Consumption of 3 servings of fish per week is recommended, of which 1–2 servings should be of oily fish, prioritising consumption of species with a lower phosphorus-to-protein ratio, that is, those with lower amounts of phosphorus per gram of protein (less than 16 mg of phosphorus per gram of protein).13 Some of the fish that meet this criterion are hake, grouper, cod, skate, sea bream, turbot and anchovies. In addition to anchovies, other oily fish, like horse mackerel and salmon, meet this recommendation, and are a good source of polyunsaturated fatty acids and have a low mercury content. On the other hand, the consumption of sardines, trout, swordfish and monkfish should be limited.
The recommended crustaceans and molluscs include prawns, cockles, clams, octopus, squid and baby cuttlefish, as long as they are not frozen or processed.
Whole eggs and dairy products have a high phosphorus-to-protein ratio, especially if processed, so the best choices are low-fat fresh cheese, cheese curds, low-fat milk and egg white.
In recent years, there has been a marked increase in the consumption of plant-based drinks in relation to the presence of food allergies or intolerances, the choice to follow a vegan diet or a variety of trends or fads. The phosphorus/protein ratio of soy milk is significantly lower compared to cow’s milk. However, it must be taken into account that these processed beverages may contain additives with phosphorus and large amounts of added sugar, so it is important to read the label.13
The bioavailability of phosphorus found in legumes and nuts is lower compared to phosphorus in animal protein sources. However, as is the case with animal protein, choosing legumes with the lowest possible phosphorus/protein ratio is recommended, such as lentils, peas or chickpeas. In general, the consumption of nuts should be limited as they contain large amounts of phosphorus with a high phosphorus/protein ratio, although it is also important to remember that they are good sources of polyunsaturated fatty acids.
Whole-grain cereals and foods contain double or even triple the amount of phosphorus compared to their refined counterparts and have a high phosphorus/protein ratio. For this reason, white bread and refined cereals should be consumed preferentially over whole-grain ones and consumed together with plant-based foods, protein or olive oil to slow down absorption of the refined carbohydrates, thereby decreasing their glycaemic load.
Supplemental Table 3S (Appendix B) provides information on the nutrient composition of foods rich in phosphorus in relation to the phosphorus/protein ratio.13
Diet compositionWith small modifications, food pyramids and the Harvard Healthy Eating Plate are practical visual models that can help educate families and children in the selection and elaboration of menus that are balanced and adhere to recommendations.21 These models can apply to children with PHP, save for the need of choosing cereals that are not whole grain and, while maintaining the indicated proportion of protein, choosing protein sources with the lowest possible phosphorus content.
Serving sizes must be adapted taking into account the age, sex, body composition, level of physical activity and clinical condition of the child. Supplemental Table 4S (Appendix B) presents another nutrition education model that may be useful, which includes the number of servings and the amount per serving (in grams or cooking measurements) of each nutrient group based on the age of the child.22
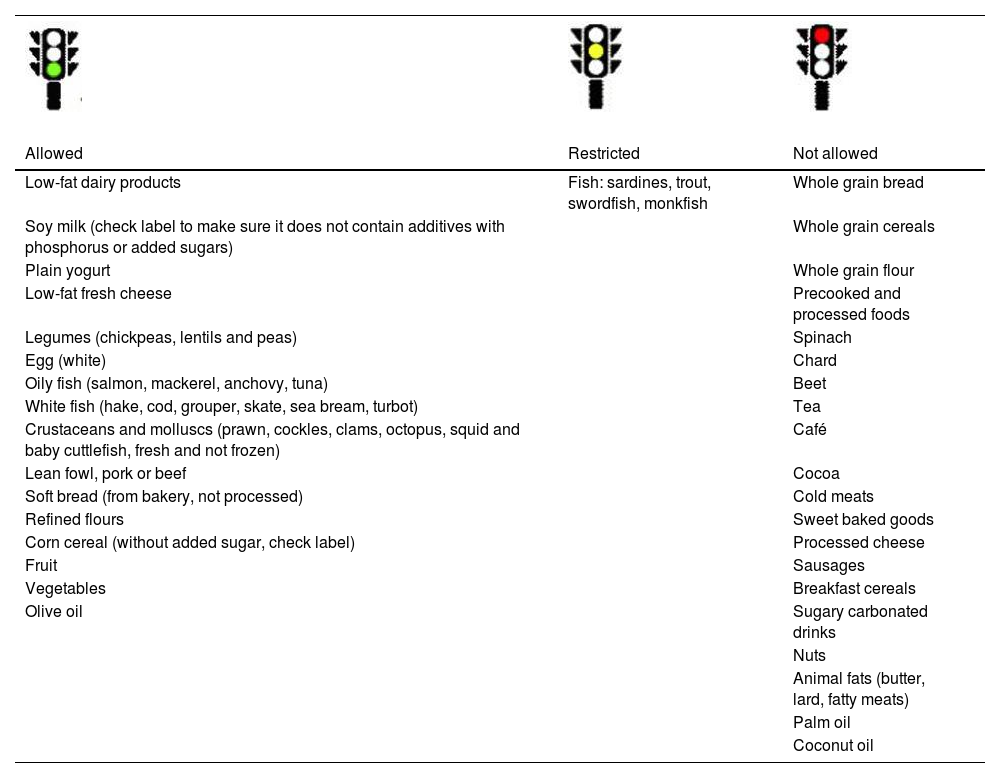
Table 5 presents a list of allowed, restricted and not allowed foods, and Supplemental Table 5S (Appendix B) and Table 6 give examples of menus for 3 days and a list of adequate options for breakfast, lunch, dinner and afternoon snacks that adhere to the daily energy, micronutrient and macronutrient intake recommendations for children with PHP.9,23
List of allowed, restricted and not allowed foods for children with pseudohypoparathyroidism.
| Allowed | Restricted | Not allowed |
|---|---|---|
| Low-fat dairy products | Fish: sardines, trout, swordfish, monkfish | Whole grain bread |
| Soy milk (check label to make sure it does not contain additives with phosphorus or added sugars) | Whole grain cereals | |
| Plain yogurt | Whole grain flour | |
| Low-fat fresh cheese | Precooked and processed foods | |
| Legumes (chickpeas, lentils and peas) | Spinach | |
| Egg (white) | Chard | |
| Oily fish (salmon, mackerel, anchovy, tuna) | Beet | |
| White fish (hake, cod, grouper, skate, sea bream, turbot) | Tea | |
| Crustaceans and molluscs (prawn, cockles, clams, octopus, squid and baby cuttlefish, fresh and not frozen) | Café | |
| Lean fowl, pork or beef | Cocoa | |
| Soft bread (from bakery, not processed) | Cold meats | |
| Refined flours | Sweet baked goods | |
| Corn cereal (without added sugar, check label) | Processed cheese | |
| Fruit | Sausages | |
| Vegetables | Breakfast cereals | |
| Olive oil | Sugary carbonated drinks | |
| Nuts | ||
| Animal fats (butter, lard, fatty meats) | ||
| Palm oil | ||
| Coconut oil |



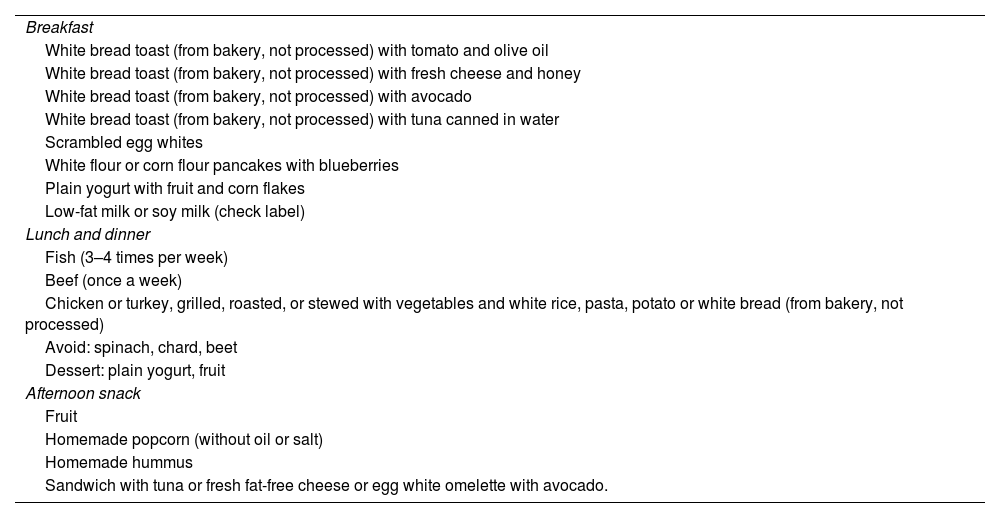
Suggested options for breakfast, lunch, dinner and afternoon snacks for children with pseudohypoparathyroidism.
| Breakfast |
| White bread toast (from bakery, not processed) with tomato and olive oil |
| White bread toast (from bakery, not processed) with fresh cheese and honey |
| White bread toast (from bakery, not processed) with avocado |
| White bread toast (from bakery, not processed) with tuna canned in water |
| Scrambled egg whites |
| White flour or corn flour pancakes with blueberries |
| Plain yogurt with fruit and corn flakes |
| Low-fat milk or soy milk (check label) |
| Lunch and dinner |
| Fish (3–4 times per week) |
| Beef (once a week) |
| Chicken or turkey, grilled, roasted, or stewed with vegetables and white rice, pasta, potato or white bread (from bakery, not processed) |
| Avoid: spinach, chard, beet |
| Dessert: plain yogurt, fruit |
| Afternoon snack |
| Fruit |
| Homemade popcorn (without oil or salt) |
| Homemade hummus |
| Sandwich with tuna or fresh fat-free cheese or egg white omelette with avocado. |
In conclusion, the principles to consider in adapting the nutrition of children with PHP are the following:
- 1.
The daily total energy intake must be controlled and physical activity promoted to prevent overweight and/or obesity and comorbidities such as carbohydrate metabolism disorders.
- 2.
The bulk of the diet must consist of fresh unprocessed foods, with daily consumption of vegetables, carbohydrates and proteins of high biological value in adequate proportions.
- 3.
The daily intake should be distributed into 4 or 5 meals a day, avoiding eating between meals.
- 4.
Foods should be prepared by steaming, boiling, stewing or grilling, avoiding frying and breading.
- 5.
It is essential to limit dietary intake of phosphorus, especially of inorganic phosphorus due to its substantial impact on blood phosphate levels.
- 6.
Patients and caregivers must know how to read food labels to recognise sources of phosphorus.
- 7.
Consumption of foods rich in calcium that are also rich in phosphorus must be limited.
- 8.
Processed, precooked or frozen foods and sugary carbonated beverages must be eliminated from the diet.
- 9.
Emphasis must be placed on encouraging the child to be physically active, engaging in at least 60 min of physical activity every day.
This research project did not receive specific financial support from funding agencies in the public, private or not-for-profit sectors.
Conflicts of interestThe authors have no conflicts of interest to declare.
María José Alcázar Villar, Luis Antonio Castaño González, Diego de Sotto Esteban, Silvia Marín del Barrio, José María Martos Tello, Lorena Miñones Suarez, Eduard Mogas Viñals, Guiomar Pérez de Nanclares Leal, Lourdes Rey Cordo, Isolina Riaño Galán.
Rosaura Leis Trabazo, Cristina Campoy Folgoso, Rafael Galera Martínez, Encina Gallego Mayo, Mercedes Gil Campos, David González Jiménez, Juan Rodríguez Delgado and Miguel Sáenz de Pipaón.
Olaya Fernández Seijas (Hospital Clínico Universitario de Santiago), Lucía Rivas Rodríguez (Hospital Clínico Universitario de Santiago), Belén Sarto Guerri (Hospital Vall d’Hebron) and Rocío Vázquez Cobela (Hospital Clínico Universitario de Santiago).
The following is Supplementary data to this article:
The members of the Grupo de Trabajo de Metabolismo Calcio-Fósforo de la Sociedad Española de Endocrinología Pediátrica and Comité de Nutrición y Lactancia Materna de la AEP present themselves at Appendix A.

