

To describe the different types of child deaths in Paediatric Intensive Care Units (PICU) in Spain, and to analyse the characteristics of those dying from a limitation of therapeutic effort (LET).
MethodA multicentre retrospective study by conducted by reviewing the hospital discharge reports corresponding to deceased patients in 8 Spanish PICUs between 2011 and 2017.
ResultsA total of 337 deaths were recorded, of which 151 (50.7%) occurred after a decision of LET, while 114 (33.8%) were due to an indicated, but failed, cardiopulmonary resuscitation, and 52 (15.4%) were due to brain death. The most common causes of hospital admission for those children that finally died were a heart-related problem (32.6%) or a respiratory problem (22.6%).
A total of 86 cases (25.5%) had a previous hospital admission, with 253 cases (75%) suffering from some type of chronical illness, and 78 (23%) had a serious disability at the time of the admission.
LET cases were more frequent among these children and those suffering from cancer. The predominant LET type consisted in: not starting the CPR in the event of a cardiac arrest (45%), withdrawal of the respiratory support (31.6%), and withdrawal of vasoactive drugs (21.6%).
ConclusionsAt the present time, at least half of the children dying in a PICU in Spain die after a LET decision, which is more frequent in those patients with previous hospital admissions, with a serious incapacity, and chronic or oncological disease. Health professionals should be aware of this situation, and be prepared to share decisions with the families, and to offer children at the end of their life the best possible caring quality.
Describir los modos de muerte de los niños en las Unidades de Cuidados Intensivos Pediátricos (UCIP) en España y analizar las características de aquellos que fallecen tras decidir una limitación del esfuerzo terapéutico (LET).
MétodosEstudio retrospectivo multicéntrico mediante revisión de informes de alta de los pacientes fallecidos en 8 UCIPs españolas entre 2011 y 2017.
ResultadosSe recogieron 337 fallecimientos, de los cuales 151 (50,7%) ocurrieron durante una decisión de LET, mientras que 114 (33,8%) fueron por reanimación cardiopulmonar indicada pero fallida (FRCP) y 52 (15,4%) por muerte cerebral. Los motivos más frecuentes de ingreso en los niños que luego fallecieron fueron cardíacos (32,6%) y respiratorios (22,6%). El 25,5% (86 casos) habían tenido ingresos previos, 253 (75.1%) padecían enfermedades crónicas y 78 (23,2%) presentaban al ingreso una discapacidad grave. La LET fue más frecuente en estos niños y en aquellos con cáncer. La LET consistió fundamentalmente en no iniciar la RCP en caso de parada cardíaca (45%), retirada de la ventilación mecánica (31.6%) y retirada de fármacos vasoactivos (21.6%).
ConclusionesEn el momento actual al menos la mitad de los niños que fallecen en una UCIP en España lo hacen tras una decisión de LET, que es más frecuente en aquellos con ingresos previos, discapacidad grave, enfermedad crónica u oncológica. Los profesionales debemos ser conscientes de esta realidad y prepararnos para compartir las decisiones con las familias y ofrecer la mejor calidad asistencial posible a los niños al final de su vida.
The death of a child at the paediatric intensive care unit (PICU) is an infrequent event that may take many forms, typically after failure of cardiopulmonary resuscitation (CPR), although it can be due to brain death or limitation of life-sustaining treatment (LoLST), the latter being a mode of death that has increased in recent years.1,3–5
LoLST involves a shared decision-making process resulting in the withdrawal or withholding of measures used for the purpose of life support in the PICU setting because they are deemed useless to the patient. The rationale is that while they could sustain certain vital functions and prolong life, they would not achieve recovery of function in the patient with a minimally acceptable quality of life,3,6 thus only prolonging the dying process.
In adult intensive care, it is increasingly frequent that patients that die do so as a result of limiting LST.7 There seems to be a similar trend in the paediatric population, albeit a less strong one, both internationally1,2,8 and in Spain,3,4 although the most recent data in our country are from 2011 and were obtained in a single hospital.4
In the past decade there have been multiple changes in the approach to the management of critically ill children, including the introduction of family-centred care,9 which promotes the continuous presence of the parents in the PICU and shared decision making by health care professionals and families.10
We conducted a multicentre study with the aim of analysing modes of death in children hospitalised in PICUs in Spanish hospitals in recent years, and the characteristics of the patients that died following a decision to limit treatment.
MethodsWe conducted a retrospective analysis of the minimum dataset included in the discharge summaries (death summary) of children deceased in the PICUs of 8 Spanish hospitals between January 1, 2011 and January 1, 2017. The inclusion criterion was death in the PICU, excluding those patients that arrived in the unit with vital signs incompatible with life.
The study was promoted by the Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos (Spanish Society of Paediatric Intensive Care) and was not funded by either public or private institutions. The study protocol was reviewed and approved by the Clinical Research Ethics Committee of Galicia. The chief physician of each PICU collected the data, which were anonymised, and the lead author of the study performed the data analysis.
We analysed the following variables: data and time of death, age, length of stay in PICU, underlying disease, chronicity, score in the Pediatric Cerebral Performance Category (PCPC) scale,11 which describes disability in 6 categories (from 1: normal to 6: brain death), previous history of hospitalisation, principal diagnosis at the time of admission to the PICU, mode of death, decision to limit LST and type (no CPR, no mechanical ventilation, no vasoactive drugs, other), request for consent of donation (and outcome), request for consent to an autopsy (and whether it was accepted or not) and consultation with the clinical ethics service.
We defined 3 modes of death in the PICU8: (a) Failed CPR, case where the patient dies despite use of all available life support measures; (b) Brain death,12,13 understood as the irreversible loss of all intracranial neurological functions, which in Spain is clinically and legally considered to correspond to the death of the individual; (c) Limitation or de-escalation of LST,3 process by which a joint decision is made to withhold or withdraw one or more measures or procedures that could support vital functions, including (if it were the case) the set of measures known as CPR.
The statistical analysis was performed with the software SPSS version 20 (SPSS Inc, Chicago, IL, USA). We have summarised the data as absolute frequencies and percentages, except for continuous data, for which we used the median and interquartile range (IQR). We used the chi square test and the Student t test for comparative analyses. We defined statistical significance as a P-value of less than .05 in any of the tests.
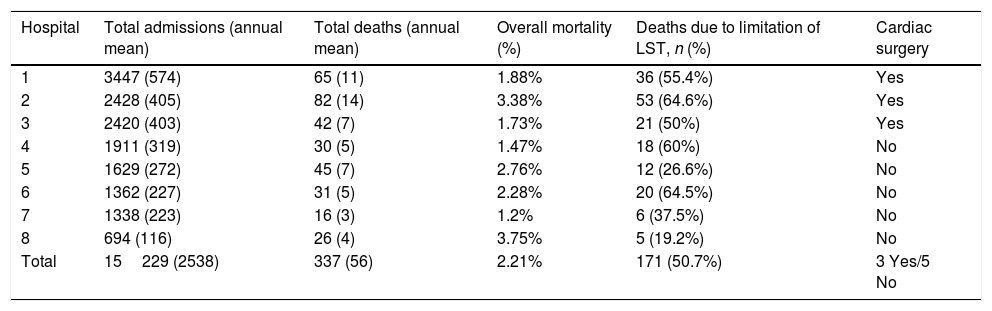
ResultsTable 1 presents a summary of the data obtained in the study. In the 6 years included in the analysis, 15229 patients were admitted to the 8 participating PICUs and 337 died, corresponding to a mean mortality of 2.2%.
Data for each hospital and overall for the MOMUCIP study. Period under study: 1/1/2011–1/1/2017.
| Hospital | Total admissions (annual mean) | Total deaths (annual mean) | Overall mortality (%) | Deaths due to limitation of LST, n (%) | Cardiac surgery |
|---|---|---|---|---|---|
| 1 | 3447 (574) | 65 (11) | 1.88% | 36 (55.4%) | Yes |
| 2 | 2428 (405) | 82 (14) | 3.38% | 53 (64.6%) | Yes |
| 3 | 2420 (403) | 42 (7) | 1.73% | 21 (50%) | Yes |
| 4 | 1911 (319) | 30 (5) | 1.47% | 18 (60%) | No |
| 5 | 1629 (272) | 45 (7) | 2.76% | 12 (26.6%) | No |
| 6 | 1362 (227) | 31 (5) | 2.28% | 20 (64.5%) | No |
| 7 | 1338 (223) | 16 (3) | 1.2% | 6 (37.5%) | No |
| 8 | 694 (116) | 26 (4) | 3.75% | 5 (19.2%) | No |
| Total | 15229 (2538) | 337 (56) | 2.21% | 171 (50.7%) | 3 Yes/5 No |
LoLST, limitation of life-sustaining treatment.
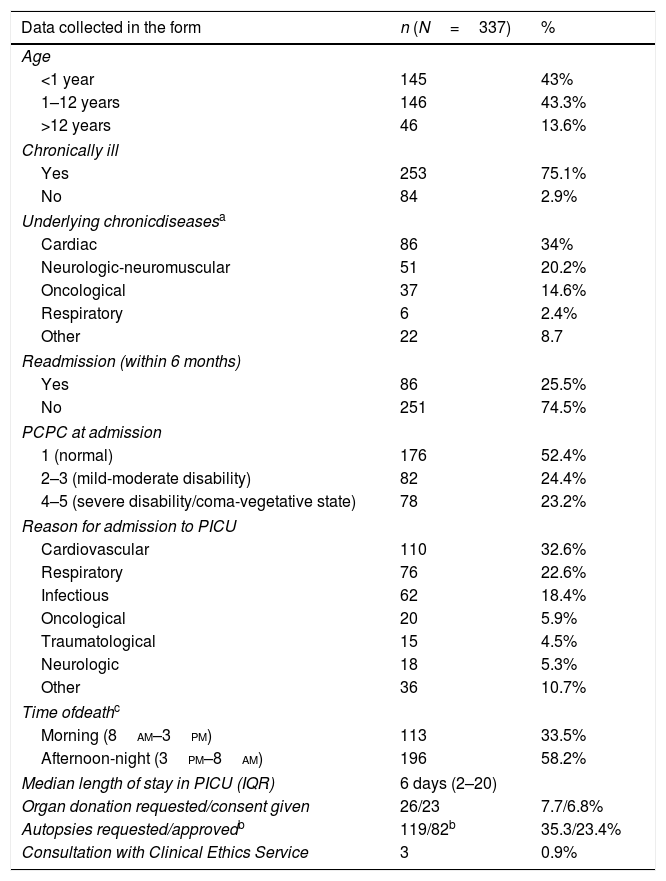
Table 2 summarises the data for the different variables analysed in the study. The deceased were aged less than 1 year in 145 cases (43%), 1–12 years in 146 cases (43.3%) and more than 12 years in 46 cases (13.6%). Of all the deceased, 253 patients (75.1%) had a chronic disease (34% cardiac, 20.2% neuromuscular, 14.6% oncological and 2.4% respiratory). In 86 cases (25.5%) the patient had been admitted to the PICU once or more in the last 6 months. The main reasons for admission to PICU in the hospitalisation that ended in death were cardiac (32.6%), respiratory (22.6%) and infectious (18.4%). At admission, based on the PCPC scale, 82 (24.4%) had mild to moderate disability, and 78 (23.2%) had severe disability or were in a vegetative state.
Summary of data collected in the form.
| Data collected in the form | n (N=337) | % |
|---|---|---|
| Age | ||
| <1 year | 145 | 43% |
| 1–12 years | 146 | 43.3% |
| >12 years | 46 | 13.6% |
| Chronically ill | ||
| Yes | 253 | 75.1% |
| No | 84 | 2.9% |
| Underlying chronicdiseasesa | ||
| Cardiac | 86 | 34% |
| Neurologic-neuromuscular | 51 | 20.2% |
| Oncological | 37 | 14.6% |
| Respiratory | 6 | 2.4% |
| Other | 22 | 8.7 |
| Readmission (within 6 months) | ||
| Yes | 86 | 25.5% |
| No | 251 | 74.5% |
| PCPC at admission | ||
| 1 (normal) | 176 | 52.4% |
| 2–3 (mild-moderate disability) | 82 | 24.4% |
| 4–5 (severe disability/coma-vegetative state) | 78 | 23.2% |
| Reason for admission to PICU | ||
| Cardiovascular | 110 | 32.6% |
| Respiratory | 76 | 22.6% |
| Infectious | 62 | 18.4% |
| Oncological | 20 | 5.9% |
| Traumatological | 15 | 4.5% |
| Neurologic | 18 | 5.3% |
| Other | 36 | 10.7% |
| Time ofdeathc | ||
| Morning (8am–3pm) | 113 | 33.5% |
| Afternoon-night (3pm–8am) | 196 | 58.2% |
| Median length of stay in PICU (IQR) | 6 days (2–20) | |
| Organ donation requested/consent given | 26/23 | 7.7/6.8% |
| Autopsies requested/approvedb | 119/82b | 35.3/23.4% |
| Consultation with Clinical Ethics Service | 3 | 0.9% |
IQR, interquartile range; PCPC, Pediatric Cerebral Performance Category scale; PICU, paediatric intensive care unit.
The time of day when deaths were most frequent was the afternoon-night (between 15pm and 8am; 58.2%). Deceased patients stayed a median of 6 days (2–20) in the PICU.
Consent for organ donation was requested in 26 cases (7.7%) and accepted by the family in 23 cases (88.4% of requests). The mode of death in the 26 cases where donation was requested was brain death in 22 cases (20 families consented to donation), failed CPR in 1 (1 family consented) and 3 LoLST (2 families consented).
In addition, an autopsy was requested in 119 cases (35.3% of total deaths), in 3 cases by a court (0.9%); and 82 autopsies were performed (70.6% of those for which consent was requested from families). The clinical ethics service was consulted in 3 cases (0.9% of total deaths).
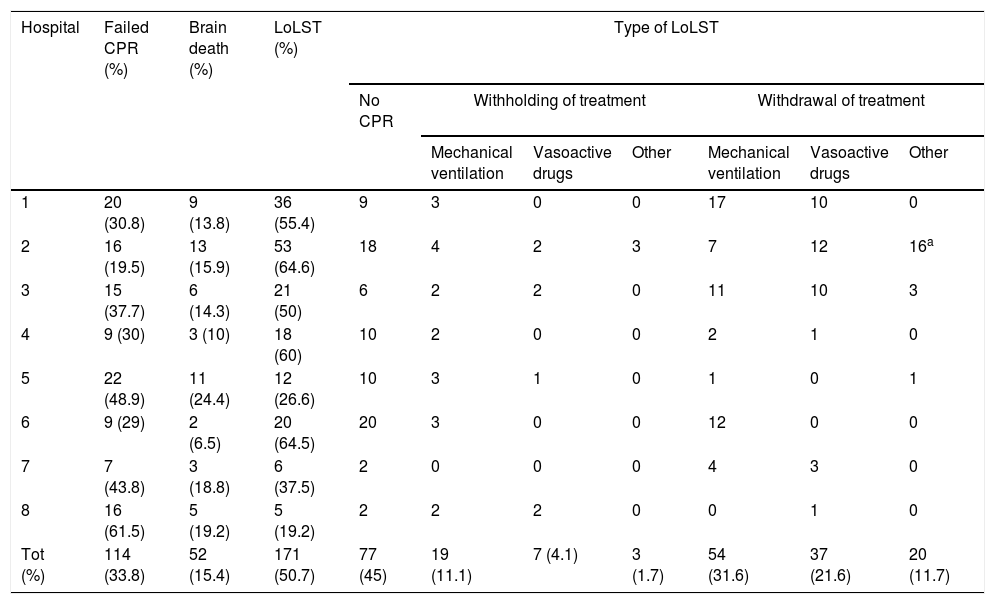
Table 3 presents the results of analysing the modes of death and types of limitation of LST. The most frequent mode of death was death following the decision tolimit LST (50.7% of total cases, with considerable variability between hospitals, with percentages ranging between 19.2% and 64.6%), followed by failed CPR (33.8%) and brain death (15.4%). The main type of LoLST was withholding CPR in case of cardiac arrest (45.0%), followed by withdrawal of mechanical ventilation (31.5%) and withdrawal of vasoactive drugs (21.6%).
Distribution of modes of death by hospital.
| Hospital | Failed CPR (%) | Brain death (%) | LoLST (%) | Type of LoLST | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No CPR | Withholding of treatment | Withdrawal of treatment | ||||||||
| Mechanical ventilation | Vasoactive drugs | Other | Mechanical ventilation | Vasoactive drugs | Other | |||||
| 1 | 20 (30.8) | 9 (13.8) | 36 (55.4) | 9 | 3 | 0 | 0 | 17 | 10 | 0 |
| 2 | 16 (19.5) | 13 (15.9) | 53 (64.6) | 18 | 4 | 2 | 3 | 7 | 12 | 16a |
| 3 | 15 (37.7) | 6 (14.3) | 21 (50) | 6 | 2 | 2 | 0 | 11 | 10 | 3 |
| 4 | 9 (30) | 3 (10) | 18 (60) | 10 | 2 | 0 | 0 | 2 | 1 | 0 |
| 5 | 22 (48.9) | 11 (24.4) | 12 (26.6) | 10 | 3 | 1 | 0 | 1 | 0 | 1 |
| 6 | 9 (29) | 2 (6.5) | 20 (64.5) | 20 | 3 | 0 | 0 | 12 | 0 | 0 |
| 7 | 7 (43.8) | 3 (18.8) | 6 (37.5) | 2 | 0 | 0 | 0 | 4 | 3 | 0 |
| 8 | 16 (61.5) | 5 (19.2) | 5 (19.2) | 2 | 2 | 2 | 0 | 0 | 1 | 0 |
| Tot (%) | 114 (33.8) | 52 (15.4) | 171 (50.7) | 77 (45) | 19 (11.1) | 7 (4.1) | 3 (1.7) | 54 (31.6) | 37 (21.6) | 20 (11.7) |
CPR, cardiopulmonary resuscitation; LoLST limitation of life-sustaining treatment.
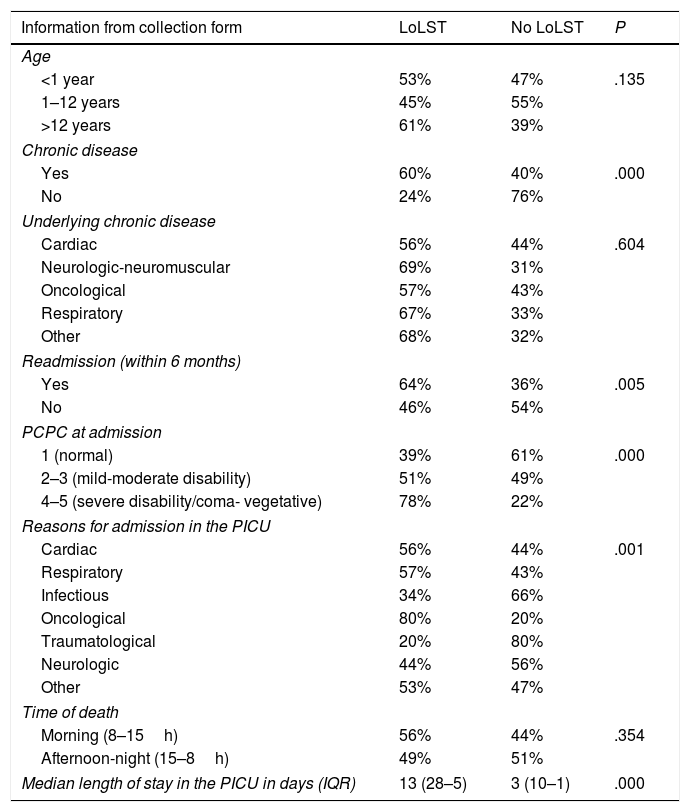
Table 4 compares deaths following LoLST and deaths due to failed CPR or brain death. Limitation of life sustaining treatment was significantly more frequent in patients with chronic disease (P=.000), readmitted patients (P=.005), patients with severe disability (P=.000) and oncological patients (P=.001). The median length of stay in the PICU was significantly longer in cases where the decision was made to limit support (13 vs 3 days) (P=.000).
Comparison of information from data collection form on deaths due to limitation of life-sustaining treatment.
| Information from collection form | LoLST | No LoLST | P |
|---|---|---|---|
| Age | |||
| <1 year | 53% | 47% | .135 |
| 1–12 years | 45% | 55% | |
| >12 years | 61% | 39% | |
| Chronic disease | |||
| Yes | 60% | 40% | .000 |
| No | 24% | 76% | |
| Underlying chronic disease | |||
| Cardiac | 56% | 44% | .604 |
| Neurologic-neuromuscular | 69% | 31% | |
| Oncological | 57% | 43% | |
| Respiratory | 67% | 33% | |
| Other | 68% | 32% | |
| Readmission (within 6 months) | |||
| Yes | 64% | 36% | .005 |
| No | 46% | 54% | |
| PCPC at admission | |||
| 1 (normal) | 39% | 61% | .000 |
| 2–3 (mild-moderate disability) | 51% | 49% | |
| 4–5 (severe disability/coma- vegetative) | 78% | 22% | |
| Reasons for admission in the PICU | |||
| Cardiac | 56% | 44% | .001 |
| Respiratory | 57% | 43% | |
| Infectious | 34% | 66% | |
| Oncological | 80% | 20% | |
| Traumatological | 20% | 80% | |
| Neurologic | 44% | 56% | |
| Other | 53% | 47% | |
| Time of death | |||
| Morning (8–15h) | 56% | 44% | .354 |
| Afternoon-night (15–8h) | 49% | 51% | |
| Median length of stay in the PICU in days (IQR) | 13 (28–5) | 3 (10–1) | .000 |
IQR, interquartile range; LoLST, limitation of life-sustaining treatment; PCPC: Pediatric Cerebral Performance Category; PICU, paediatric intensive care unit.
We compared the data collected in the data collection form with the deaths due to LoLST, using the chi square test except for the length of stay, for which we used the Student t test
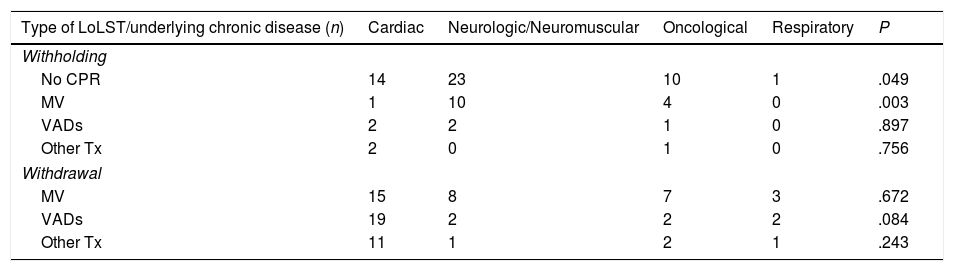
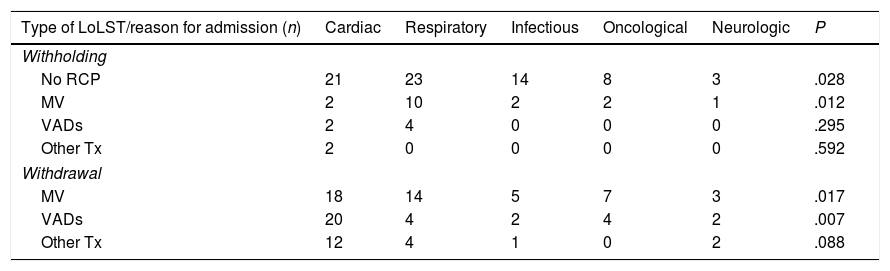
We found an association between the type of LoLST and the type of underlying disease (Table 5) as well as the reasons for admission (Table 6). Thus, withholding CPR or mechanical ventilation were more frequent in children with neuromuscular illness or admitted due to respiratory illness. On the other hand, withdrawal of ventilatory support or vasoactive drugs was more frequent in children admitted due to heart disease.
Comparison of types of limitation of life-sustaining treatment and type of underlying chronic disease.
| Type of LoLST/underlying chronic disease (n) | Cardiac | Neurologic/Neuromuscular | Oncological | Respiratory | P |
|---|---|---|---|---|---|
| Withholding | |||||
| No CPR | 14 | 23 | 10 | 1 | .049 |
| MV | 1 | 10 | 4 | 0 | .003 |
| VADs | 2 | 2 | 1 | 0 | .897 |
| Other Tx | 2 | 0 | 1 | 0 | .756 |
| Withdrawal | |||||
| MV | 15 | 8 | 7 | 3 | .672 |
| VADs | 19 | 2 | 2 | 2 | .084 |
| Other Tx | 11 | 1 | 2 | 1 | .243 |
LoLST, limitation of life-sustaining treatment; MV, mechanical ventilation; Tx, treatment; VAD, vasoactive drug.
Comparison of types of limitation of life-sustaining treatment and the reasons for admission.
| Type of LoLST/reason for admission (n) | Cardiac | Respiratory | Infectious | Oncological | Neurologic | P |
|---|---|---|---|---|---|---|
| Withholding | ||||||
| No RCP | 21 | 23 | 14 | 8 | 3 | .028 |
| MV | 2 | 10 | 2 | 2 | 1 | .012 |
| VADs | 2 | 4 | 0 | 0 | 0 | .295 |
| Other Tx | 2 | 0 | 0 | 0 | 0 | .592 |
| Withdrawal | ||||||
| MV | 18 | 14 | 5 | 7 | 3 | .017 |
| VADs | 20 | 4 | 2 | 4 | 2 | .007 |
| Other Tx | 12 | 4 | 1 | 0 | 2 | .088 |
LoLST, limitation of life-sustaining treatment; MV, mechanical ventilation; Tx, treatment; VAD, vasoactive drug.
Ours is the first multicentre study that has collected recent data on the modes of death in critically ill children in Spain. The most salient finding was that the average mortality in the 8 participating hospitals was much lower (2.2%) than those reported in international studies conducted in other countries2,14,15 and at the Hospital Sant Joan de Deu,3,4 conducted before 2011, but similar to the values reported recently by hospitals in the United States.1,5,8 This fact, which is unquestionably positive, has the relative downside that health professionals working in PICU settings are decreasingly exposed to death, which may affect their ability to appropriately approach the process of death in a child.10,16
On the other hand, as has occurred in other countries,1,2,5,17 the distribution of the modes of death in the PICU in Spain have shifted. While we found significant variability in the proportion of deaths due to LoLST between units (from 20% to 65%), at present most critically ill children (who amount to nearly 2/3 of patients in some PICUs) that die do so following withholding or withdrawing of life-sustaining measures.
Given the above, health professionals must be trained and ready to identify specific situations where LoLST is indicated and to carry out this process as correctly as possible, always involving the family of the patient in decision making. Our findings show that the decision to limit LST is applied most frequently to children with chronic illness, a previous history of admission to the PICU (so that the patient and family are already acquainted with the staff), with severe disability at the time of admission or admitted due to a severe complication of a solid or blood tumour.
The decision to limit LST is usually founded on 2 criteria: a low probability of survival or a poor quality of life in case of survival. The first is a clinical criterion: any measure that does not advance survival would be contraindicated, and thus it is logical that health professionals take the initiative to propose and explain this approach to families. The second criterion is usually more complex, as the evaluation of quality of life is subjective, and since paediatric patients are minors, it is usually the opinion of the parents that counts. The possibility of limiting LST should be presented to parents gently and with tact, as it is possible that they are not aware of this possibility and each family unit has a unique life plan that must be respected by health professionals as long as it does not result in serious harm to the child.18
In recent times, the clinical criterion has been reinforced by the emergence of so-called “death with dignity” laws,19 which provide legal protection for clinicians that practice limitation of LST. In any case, clinical practice guidelines for end-of-life care may be more useful to physicians. Broadly speaking, international guidelines20,21 can be applied in our country, but the recommendations developed by the Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos (Spanish Society of Paediatric Intensive Care, SECIP) are probably better suited to the specific circumstances of Spain.22
If we intend that LoLST be a process of decision making throughout time, these patients should stay in the unit as long as necessary for health professionals and parents to clearly identify the most appropriate option. This seemed to be the case in the units under study, as the length of stay in the PICU was much longer in patients that died following LoLST compared to patients that died after FCPR or from brain death. The new open-door policy of intensive care units for parents and their continuous presence in the unit is allowing ongoing interaction with the staff and probably improving agreement in shared decision making, although at the same time it may also increase the number of conflicts that arise between families and staff.23,24 A factor that may be relevant in the process of LoLST in this regard is the timing of the decision and of its implementation. In our study, in more than half of the cases, death occurred during the afternoon or at night. We do not have any data to determine whether this resulted from intentional shared decisions that took into account the time that the unit would be quieter or that family members could be present, or whether the decision was made in the morning and implemented within the after-hours care time frame.
In the PICUs under study, the most frequent form of LoLST was withholding of CPR in case of cardiac arrest, followed by withdrawal of ventilatory support, which was consistent with previous studies in other countries.1,12,23,25 In any case, a more detailed analysis of the types of limitation of support showed that limitation of more than one measure was frequent in the patients, usually withholding of CPR combined with withholding and/or withdrawal or mechanical ventilation. These findings were consistent with the data previously reported by the Hospital Sant Joan de Déu.4
We ought to highlight that in our sample, 3/4 of the deceased were chronically ill children, of who 60% died following limitation of LST, a percentage that was similar to those reported in other studies, ranging between 45% and 88%.3,4,25,26 This, combined with the fact that more than half had a history of previous admission to the PICU or severe disability, reflects a reality that is well known by health professionals in the PICU setting and in many instances allows accurate prognostication, and should facilitate early decision making, planning and implementation of care in agreement with the families (and in those cases where patients are mature enough, the patients themselves).
Organ donation is an option available to numerous families in the event of the death of a child, and many report feeling a degree of solace from knowing that they were able to help another family. In the participating PICUs, donation was requested in a small percentage of cases (7.7% of total deaths), and this percentage was lower in cases of death following LoLST (0.9%). It is possible that contraindications for transplantations existed in many cases, but considering the decrease in the number of paediatric donors27,28 and the increase in the proportion of deaths following limitation of LST, intensivists should take into account the option of controlled donation after circulatory death or Maastricht donor category III, which could apply to these patients, and discuss each potential case with the transplant coordinator of the hospital. At present, a working group coordinated by the Organización Nacional de Trasplantes (National Transplant Organization) is developing a guideline on the subject that will be very helpful to health professionals in the PICU setting.
In any case, it is worth mentioning that 88% of families consent to donation when it is requested.29
As for post-mortem examinations, autopsies were requested in slightly over 2/3 of the deceased patients, with substantial variability between hospitals and with 2/3 of requested autopsies being finally performed, which was a proportion comparable to that found in a multicentre study in the United States.1 It is a known fact that fewer autopsies are performed than would be advisable, and that efforts must be made to improve on this aspect.30,31
Last of all, we were surprised at the low frequency of consultation with the clinical ethics service, either because the care team and the family were in agreement with the process or because they did not consider consultation useful or necessary. It is well known that mediation by ethics committees may help both families and providers in situations where ethical dilemmas arise in clinical practice.32,33
There are limitations to our study, such as the inclusion of data from only 8 PICUs in Spain located in 7 different autonomous regions, so that we cannot safely assume that the data provide an accurate reflection of modes of death and the practice of limitation of LST nationwide. In each case, the analysis of the data was restricted to those variables recorded in the discharge summary of the patient (death summary), which usually does not include information about the process used for end-of-life decision making, so we lacked information that may be relevant to the subject under study. In this regard, we consider that a value history should be included in the clinical records of all children admitted to a PICU.34
ConclusionsAt present, at least half of the children that die in PICUs in Spain do so after a decision to limit LST, which is more frequent in children readmitted to the PICU or with severe disability, chronic disease or some form of cancer. As health professionals, we must be aware of this situation and be prepared to involve the families in decision making and offer the most suitable care plan and high-quality end-of-life care to children that have to die in an intensive care setting.
The members of the RETROSPECTIVE MOMUCIP group:
Francisco Javier Pilar Orive; Paediatric Intensive Care Unit. Hospital de Cruces, Barakaldo. Spain. Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos.
Elva Rodríguez Merino; Paediatric Intensive Care Unit. Hospital de Cruces, Barakaldo. Spain. Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos.
Jesús López-Herce Cid; Paediatric Intensive Care Unit. Hospital General Universitario Gregorio Marañón, Madrid. Spain.
Gema Manrique Martín; Paediatric Intensive Care Unit. Hospital General Universitario Gregorio Marañón, Madrid. Spain.
Paula García Casas; Paediatric Intensive Care Unit. Hospital General Universitario Gregorio Marañón, Madrid. Spain.
Arturo Hernández González; Paediatric Intensive Care Unit. Hospital Puerta del Mar, Cádiz. Spain. Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos.
Carmen Ramil Fraga; Paediatric Intensive Care Unit. Complexo Hospitalario Universitario de A Coruña. A Coruña. Spain. Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos.
Corsino Rey Galán; Paediatric Intensive Care Unit. Hospital Universitario Central de Asturias, Oviedo. Spain.
María Rosario Riestra Rodríguez; Paediatric Intensive Care Unit. Hospital Universitario Central de Asturias, Oviedo. Spain.
Ramón Hernández Rastrollo; Paediatric Intensive Care Unit. Hospital Materno-Infantil, Badajoz. Spain. Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos.
Francisco Fernández Carrión; Paediatric Intensive Care Unit. Hospital Clínico Universitario de Salamanca. Spain.
Antonio Rodríguez Núñez; Department of Paediatric Critical, Intermediate and Palliative Care. Section of Paediatrics. Complexo Hospitalario Universitario de Santiago de Compostela. CLINURSID (Universidad de Santiago) and Life Support and Simulation (FIDIS) research groups. Ethics Group of the Sociedad Española de Cuidados Intensivos Pediátricos.
The following are the supplementary data to this article:
The members of the MOMUCIP RETROSPECTIVE working group are presented at Appendix B.
Please cite this article as: Agra Tuñas MC. Modos de fallecimiento de los niños en Cuidados Intensivos en España. Estudio MOMUCIP (modos de muerte en UCIP). Arch Bronconeumol. 2019;91:228–236.
Previous presentations: This study was presented as an oral communication with the title “Modos de muerte en la UCIP. Estudio piloto para la propuesta de un registro nacional” at the 32 National Congress of the Sociedad Española de Cuidados Intensivos Pediátricos (SECIP); May 6, 2017; Granada, Spain. Also as a poster with oral presentation with the title “Ha cambiado el modo de morir de los niños en las unidades de cuidados intensivos pediátricos?” at the 66 Congress of the Asociación Española de Pediatría; June 7–9, 2018; Zaragoza, Spain.
- Documento de manejo clínico del paciente pediátrico con infección por SARS-CoV-2.
(Actualizado el 26 de Noviembre de 2020) - Test de diagnóstico rápido en las consultas de Pediatría de Atención Primaria y Urgencias Pediátricas en la era COVID-19: más que una recomendación
(Actualizado el 21 de septiembre de 2020) - Consenso nacional sobre diagnóstico, estabilización y tratamiento del Síndrome Inflamatorio Multisistémico Pediátrico vinculado a SARS-CoV-2 (SIM-PedS).
(Actualizado el 27 de Julio de 2020) - Recomendaciones para el manejo del recién nacido en relación con la infección por SARS-CoV-2.
(Actualizado el 27 de Mayo de 2020) - Manejo del paciente pediátrico ante sospecha de infección por el nuevo coronavirus SARS-CoV-2 en atención primaria (COVID-19). AEPap-SEIP/AEP-SEPEAP.
(Actualizado el 27 de Abril de 2020) - Propuesta de adaptación de las recomendaciones de reanimación cardiopulmonar pediátrica avanzada a la infección por coronavirus.
(Actualizado el 11 de Abril de 2020)


Anales de Pediatría (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals