

Meconium aspiration syndrome (MAS) was first described by Cleary and Wiswell as respiratory distress in an infant born through meconium-stained amniotic fluid (MSAF) whose symptoms cannot be otherwise explained.1 Although the incidence of MSAF in term births is of 10% to 16%, the incidence of MAS in pregnancies with MSAF is low, ranging from 0.10% at 37 weeks’ gestation to 0.31% at 41 weeks.2
Its pathophysiology is complex and has yet to be fully elucidated, with the available evidence suggesting that mild and severe presentations of MAS are not part of a single disease spectrum but could involve different aetiologies and risk factors, with severe MAS presenting with other problems in addition to meconium aspiration such as infection or chronic asphyxia.3,4 The risk factors associated with severe MAS have been classified into maternal, intrapartum and neonatal factors,2 and many studies have been devoted to the subject, some with contradictory results.5
The presence of MSAF in itself does not explain severe cases of MAS, and given the importance of early diagnosis, we decided to carry out a study with the aim of identifying factors associated with more severe presentations of MAS in our catchment population.
We conducted a retrospective descriptive study including all cases of MAS managed in the neonatal intensive care unit (NICU) of our hospital between January 2012 and May 2018. We collected data by reviewing obstetric and neonatal electronic health records in our hospital’s system. We classified the risk factors under study into three groups: maternal variables, intrapartum variables and neonatal variables (Table 1). We classified MAS cases by severity into 2 categories using the scheme proposed by Cleary and Wiswell1: severe, defined as requiring mechanical ventilation (MV) for 48 h, and nonsevere (mild/moderate), defined as not requiring MV or MV lasting less than 48 h. We performed the statistical analysis with the software SPSS (version 23).
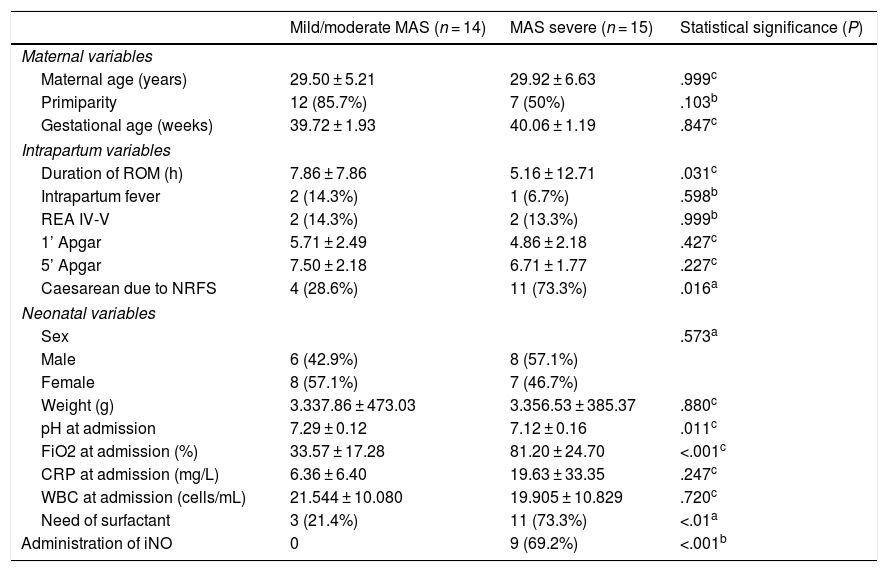
Maternal, intrapartum and neonatal variables associated with the severity of MAS.
| Mild/moderate MAS (n = 14) | MAS severe (n = 15) | Statistical significance (P) | |
|---|---|---|---|
| Maternal variables | |||
| Maternal age (years) | 29.50 ± 5.21 | 29.92 ± 6.63 | .999c |
| Primiparity | 12 (85.7%) | 7 (50%) | .103b |
| Gestational age (weeks) | 39.72 ± 1.93 | 40.06 ± 1.19 | .847c |
| Intrapartum variables | |||
| Duration of ROM (h) | 7.86 ± 7.86 | 5.16 ± 12.71 | .031c |
| Intrapartum fever | 2 (14.3%) | 1 (6.7%) | .598b |
| REA IV-V | 2 (14.3%) | 2 (13.3%) | .999b |
| 1’ Apgar | 5.71 ± 2.49 | 4.86 ± 2.18 | .427c |
| 5’ Apgar | 7.50 ± 2.18 | 6.71 ± 1.77 | .227c |
| Caesarean due to NRFS | 4 (28.6%) | 11 (73.3%) | .016a |
| Neonatal variables | |||
| Sex | .573a | ||
| Male | 6 (42.9%) | 8 (57.1%) | |
| Female | 8 (57.1%) | 7 (46.7%) | |
| Weight (g) | 3.337.86 ± 473.03 | 3.356.53 ± 385.37 | .880c |
| pH at admission | 7.29 ± 0.12 | 7.12 ± 0.16 | .011c |
| FiO2 at admission (%) | 33.57 ± 17.28 | 81.20 ± 24.70 | <.001c |
| CRP at admission (mg/L) | 6.36 ± 6.40 | 19.63 ± 33.35 | .247c |
| WBC at admission (cells/mL) | 21.544 ± 10.080 | 19.905 ± 10.829 | .720c |
| Need of surfactant | 3 (21.4%) | 11 (73.3%) | <.01a |
| Administration of iNO | 0 | 9 (69.2%) | <.001b |
Continues variables expressed as mean ± standard deviation. Qualitative variables expressed as n (%).
iNO, inhaled nitric oxide; NRFS, non-reassuring foetal status; RDR, resuscitation in delivery room; ROM, rupture of membranes; WBC, white blood cell count.
During the study period, the hospital managed a total of 31 324 deliveries and 48 cases of MAS, corresponding to an incidence of 0.15%. Of all cases, we were able to collect data for 29 patients, 51.7% female and 48.3% male. In terms of severity, 52% of the cases of MAS were severe (n = 15) and 48% nonsevere (n = 14). In the group of severe MAS, 1 patient died (6.6%) and 3 (20%) had long-term neurologic sequelae.
None of the maternal variables under study (maternal age, primiparity or duration of pregnancy), was associated significantly with severe MAS.
When it came to the intrapartum variables, intrapartum fever, the Apgar scores and resuscitation with intubation, chest compressions or vasoactive drugs were not significantly associated with severe MAS in our sample, either.
The intrapartum variables significantly associated with severe MAS were urgent caesarean section due to non-reassuring foetal status (NRFS) and the total duration of rupture of membranes (ROM).
The neonatal variables associated with severe MAS were the pH at admission, contrary to previous studies that did not find a significant association,2 a high fraction of inspired oxygen (FiO2) at admission (28.6% of infants with severe MAS required a FiO2 of 30%–60% and 85.7% a FiO2 > 60%), the need of surfactant and treatment with inhaled nitric oxide (iNO).
Although the association with the need for surfactant and with treatment with iNO were statistically significant, we did not consider these factors predictors of poorer outcomes, as their use intrinsically implies more severe MAS and therefore this would be an expected association.
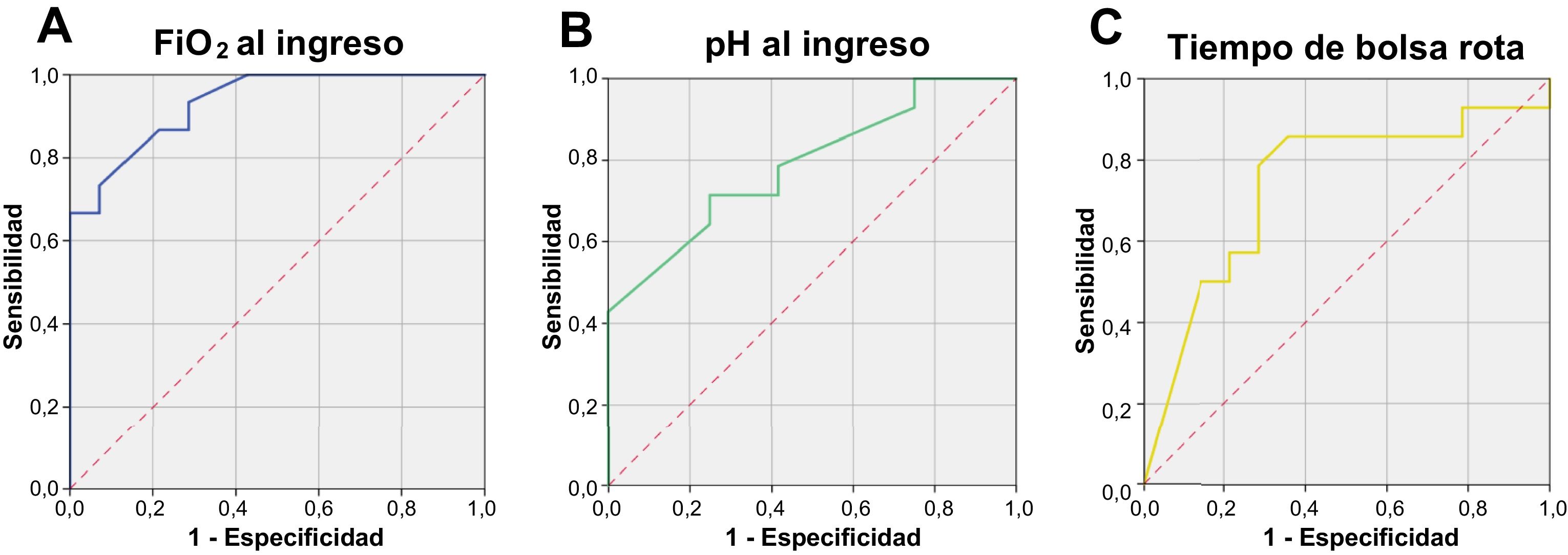
In the multivariate logistic regression analysis performed to identify predictors of severe MAS, the only variable that remained significant for prediction of severe disease after adjusting for all other variables (P < .01). We generated receiver-operating characteristic (ROC) curves to establish the optimal cut-off points for the FiO2 at admission, the pH at admission and the total duration of ROM (Fig. 1).
![ROC curves for FiO2 (A), pH at admission (B) and duration of ROM (C). A: FiO2 > 35% predicts severe MAS with a sensitivity (Sen) of 93% and a specificity (Spe) of 72%; FiO2 > 65% showed a Sen of 73% and a Spe of 93% for severe MAS, with an area under the curve (AUC) of 0.93 (95% confidence interval [CI], 0.85–1). B: A pH at admission <7.22 was associated with severe MAS, with a Sen of 71.4% and a Spe of 75%; a pH at admission <7.12 was associated with severe MAS with a Sen of 50% and a Spe of 91.7%, with an AUC of 0.789 (95% CI, 0.616–0.962). C: A duration of ROM < 6 h was associated with severe MAS with a Sen of 85.7%, a Spe of 64.3% and an AUC of 0.737 (95% CI, 0.541–0.933).](https://static.elsevier.es/multimedia/23412879/0000009400000005/v1_202105040835/S2341287921000405/v1_202105040835/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w9/qVHBXBqbSQ7FNUvNof+6+l4v03CmyaR9Rm+q8TRfDERovN5wMUmDVyYvA+rI0XvChhvsJahGSDZO4Z6vt1NI1CZGvHarFuAdZXRiZ1BsZTN4wbKCYL2TLpS/KU/Q6dKoMZxmmn+BzDIf7oU4lbyGe5vQlfRwETigFa7tNp8AsQtoxwrAkoxBipZ5hQTjRZYz04vRfvkwwPh4RqM9IMWLIDp1/3w8Q6rWqVmZC2gQvVRnH1rGxlAEYwcU+DSioU8t92bivcYi9+AAKrUM7VcZM= "ROC curves for FiO2 (A), pH at admission (B) and duration of ROM (C). A: FiO2 > 35% predicts severe MAS with a sensitivity (Sen) of 93% and a specificity (Spe) of 72%; FiO2 > 65% showed a Sen of 73% and a Spe of 93% for severe MAS, with an area under the curve (AUC) of 0.93 (95% confidence interval [CI], 0.85–1). B: A pH at admission <7.22 was associated with severe MAS, with a Sen of 71.4% and a Spe of 75%; a pH at admission <7.12 was associated with severe MAS with a Sen of 50% and a Spe of 91.7%, with an AUC of 0.789 (95% CI, 0.616–0.962). C: A duration of ROM < 6 h was associated with severe MAS with a Sen of 85.7%, a Spe of 64.3% and an AUC of 0.737 (95% CI, 0.541–0.933).")
ROC curves for FiO2 (A), pH at admission (B) and duration of ROM (C). A: FiO2 > 35% predicts severe MAS with a sensitivity (Sen) of 93% and a specificity (Spe) of 72%; FiO2 > 65% showed a Sen of 73% and a Spe of 93% for severe MAS, with an area under the curve (AUC) of 0.93 (95% confidence interval [CI], 0.85–1). B: A pH at admission <7.22 was associated with severe MAS, with a Sen of 71.4% and a Spe of 75%; a pH at admission <7.12 was associated with severe MAS with a Sen of 50% and a Spe of 91.7%, with an AUC of 0.789 (95% CI, 0.616–0.962). C: A duration of ROM < 6 h was associated with severe MAS with a Sen of 85.7%, a Spe of 64.3% and an AUC of 0.737 (95% CI, 0.541–0.933).
Based on our findings, patients with a diagnosis of MAS that required urgent caesarean delivery due to NRFS, duration of ROM of less than 6 h, a FiO2 at admission greater than 35% and a pH at admission of less than 7.22 are at higher risk of developing severe disease, and FiO2 was the best predictor after adjusting for the rest of the variables. These conclusions must be interpreted with caution, as the main limitation of the study was its small sample size.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Nogueira-Cobas C, Antúez-Fernández C, Saldaña-García N, Saldaña-García J, Sánchez-Tamayo T. Síndrome de aspiración meconial: factores sugerentes de mala evolución. An Pediatr (Barc). 2021;94:333–335.

